
記住我


Randomization is at the level of the healthcare facility. A cluster-randomized design is used in which entire facilities are randomized because the intervention impacts CHW workflow and therefore affects all households under their care rather than individual clients. The comparison control treatment is the standard of care version of eCHIS which is currently being used by CHWs across Kenya. eCHIS guides CHWs through completing home visits, with a range of workflows including maternal health, child health, nutrition, malaria, and water sanitation and hygiene [46]. This version of eCHIS has no SMS communication between CHWs and clients. In both study arms, antenatal and maternal and child health clinical services continue to be provided through MOH clinics with minimal interactions with study personnel.
Intervention descriptionIntervention sites utilize a modified version of eCHIS which has SMS messaging incorporated as an additional module (CHV-NEO).
SMS curriculumThe CHV-NEO SMS intervention is based on the content of the Mobile WACh NEO intervention [41], with adaptations for this study guided by input from perinatal clients, nurses, CHWs, and CHW supervisors in formative interviews and focus groups. The intervention is based on the Information, Motivation, Behavioral skills model of behavioral change [47], with the goal of improving the provision of preventative ENC, identification of illness, and care-seeking if needed (Fig. 2). Clients receive a curriculum of pre-composed SMS messages automatically sent on a schedule starting at 28 weeks gestation and extending until 6 weeks postpartum. Clients can send an SMS at any time and their message will be read and manually responded to by the CHW who routinely conducts their home visits. Automated messages are sent in English, Luo, or Kiswahili depending on the participant’s preference. Sending and receiving SMS is at no cost to the participant or the CHW.
Fig. 2
Intervention conceptual framework
Automated SMS topics and schedule are summarized in Fig. 3, based on the client’s gestational age, date of delivery, and delivery outcome, obtained from eCHIS. From enrolment until 38 weeks gestation, automated SMS are sent weekly, encouraging facility delivery and birth planning, and providing anticipatory guidance about neonatal danger signs and emotional support. From 38 weeks gestation until delivery, automated SMS are sent daily, with similar content and highlighting neonatal danger signs and ENC practices, including immediate and exclusive breastfeeding, thermal, and cord care. From delivery to 2 weeks postpartum, two messages are sent per day: one message with screening questions regarding neonatal danger signs and encouragement to message if they have a concern and one message with educational content on postpartum care and complications, ENC practices, and emotional support. From 2 to 6 weeks postpartum, SMS are delivered every other day. Additionally, based on input from perinatal clients, CHWs, and policymakers in formative design activities, clients receive a reminder message when they are referred to the healthcare facility by the CHW, when they are due for their 6-week postpartum facility visit, and when a CHW is scheduled to conduct a home visit. All messages open with the participant’s name, state that the message is from their CHW, and contain a question to engage women in conversation. Clients who deliver a preterm or low birthweight baby receive a modified track of messages, which includes information about additional care for small and preterm babies, including Kangaroo Mother Care. Clients who experience a stillbirth or neonatal death receive a 4-week curriculum of weekly bereavement messages which provide condolences and emotional support; messages related to the infant are stopped. The message bank is available upon request.
Fig. 3
Message content and schedule were developed by a group of content experts on the study team. Messages are based on the Mobile WACh NEO intervention [41], with the following modifications to account for the shift from nurse to CHW delivery and to respond to stakeholder input in our formative design activities. Terminology in the messages was simplified to remove technical clinical terms and better align with lay vocabulary used by CHWs. To align with CHWs’ preventative service focus, additional messages were added antenatally providing anticipatory guidance for ENC, nutrition counseling, and reminders about family planning. To align with CHWs’ referral responsibilities and limited diagnostic role, message language requesting participants describe symptoms of illness was removed and replaced with a recommendation to seek facility-based care in case of health concerns. Discussion of mental health topics was removed due to CHW input that they did not feel comfortable responding to in-depth messages about mental illness; instead, emotionally supportive language such as “I am here for you” was increased. Additionally, based on findings from the Mobile WACh NEO trial, the frequency of antenatal messages with anticipatory guidance related to trial outcomes, particularly infant danger signs, was increased, while the frequency of messages encouraging facility delivery was decreased, given the high rates of facility delivery currently in Kenya (> 80%) [43].
Integration of SMS into eCHIS applicationIn partnership with the Kenyan Ministry of Health, SMS messaging functionality was integrated into the eCHIS software platform as a module of the existing interface (Fig. 4). Consenting and enrollment to communicate by SMS with the CHW was added as a required step in the standard antenatal home visit workflow among intervention CHWs, and an additional functionality was added to update client phone number, SMS language, or messaging preferences after enrollment as needed. Templates for CHW replies to frequently asked client questions were incorporated as a “FAQ” module with a topically organized bank of editable message templates in English, Swahili, and Luo (Fig. 4).
Fig. 4
Screenshots of SMS components of eCHIS
In addition to integrating SMS functionality into CHW workflows, we incorporated supervision of SMS messaging into the workflows of CHW supervisors. As part of their monthly supervision workflow, supervisors are prompted to review a CHW’s messaging, ask them if they have experienced any challenges with messaging, and support them in problem-solving any challenges.
Training and launch activitiesThe study provided training to CHWs and supervisors at the study launch on the following topics. All CHWs and supervisors in control and intervention clusters received a 2.5-day training on how to use eCHIS. Those in intervention clusters received an additional day of training on how to use the CHV-NEO SMS workflows in eCHIS. To ensure a baseline level of clinical knowledge related to maternal and neonatal health, all CHWs in both arms also received a half-day refresher training on their clinical responsibilities related to antenatal and postnatal care, newborn health, and maternal mental health.
As part of training, CHWs were instructed to sync their eCHIS application with the server daily, respond to clients by SMS within 24 h, refer to the facility if any unusual symptoms are reported by SMS or if they were unsure how to respond, seek advice from their supervisors if they have challenges with any workflows, and report any technical issues to the study team.
Criteria for discontinuing or modifying allocated interventions SMS withdrawalClients in the intervention group may withdraw from receiving SMS messages at any time by either sending a SMS with the word “stop” or asking their CHW to stop their messaging. Participants who withdraw from SMS can continue or withdraw from study activities.
Study withdrawalParticipants may withdraw from the study at any time for any reason. Study staff record the timing and reason for any early terminations. All data collection will be discontinued at the time of withdrawal. Participants who withdraw from study activities can continue or withdraw from the SMS program.
Strategies to improve adherence to interventionsCHWs in Kisumu County receive routine supervision to support their service delivery, in the form of monthly group meetings and individual meetings between CHWs and their supervisor. The study carries out the following additional quality assurance activities. At monthly group meetings, the study shares a report on aggregate CHW performance in terms of completeness of eCHIS data related to pregnancies and newborns and, at intervention facilities, SMS messaging process indicators. Additionally, the study team conducts a monthly review of a sample of CHWs’ SMS exchanges with clients. Clinical experts on the study team review CHW message timeliness and appropriateness per standards set forth in prior Mobile WACh studies [37, 41]. Summary data from these reviews and feedback for CHW responses are shared with CHWs and their supervisors at the monthly supervision meetings. The same data is also shared with Kisumu County leadership at separate regular meetings.
Relevant concomitant care permitted or prohibited during the trialPerinatal women participants in both arms continue to receive all standard healthcare services from local healthcare facilities. The study provides no clinical care.
Provisions for post-trial careParticipants continue with services as usual post-trial.
Outcomes Clinical outcomesPrimary, secondary, and exploratory clinical outcomes are summarized in Table 1. The primary outcome is neonatal mortality, defined as the death of a live-born infant within 28 days of birth, based on routine data abstracted from eCHIS during the study period. Secondary outcomes are ascertained among the in-depth perinatal cohort who complete study questionnaires. Secondary outcomes were selected based on the intervention’s hypothesized mechanism of action (Fig. 2) and their importance as intermediate outcomes in neonatal survival. These include initiation of breastfeeding within the first hour of life (ascertained by maternal self-report at the 6-week postpartum study visit); application of substances to cord (ascertained by maternal self-report at the 6-week visit); maternal knowledge of neonatal danger signs (defined as the number of the eight neonatal danger signs correctly named at the 6-week visit); and appropriate care seeking (defined as the proportion of illness episodes with danger signs where the infant attended the clinic, based on maternal self-report at the 6-week visit). Exploratory clinical outcomes include mothers’ identification of danger signs in their infants (defined as the proportion of all infants whose mothers report they ever exhibited a danger sign at the 6-week visit); infant hospital admissions (based on maternal self-report); and neonatal care delays (defined as the proportion of neonatal deaths attributable to each delay in the three delays model, based on review of adverse event reports by nurses and physicians on the study team).
Service delivery and implementation outcomesIn addition to clinical outcomes, we will compare service delivery outcomes between arms as exploratory outcomes (Table 1). These outcomes are ascertained from eCHIS data and self-report questionnaires from all CHWs (N = 700). These include home visit coverage (defined as number of home visits performed by CHWs); perinatal clinic referrals (defined as number of clinic referrals logged by CHWs in eCHIS for clients who are pregnant or up to 3 months postpartum); and CHW and supervisor workload (defined as time on all work duties, based on self-report questionnaire).
Within the intervention arm, CHV-NEO acceptability, adoption and fidelity of use by CHWs and their supervisors is determined using questionnaires and eCHIS data. Acceptability is defined as perception by CHWs that CHV-NEO is agreeable or satisfactory, using the AIM scale in CHW self-report questionnaire [48]; adoption is defined as the proportion of client SMS replied to by CHWs at all based on eCHIS data; and fidelity is defined as the proportion of client SMS responded to by CHWs in an appropriate and timely fashion, ascertained through monthly structured review and scoring of a sample of SMS conversations by clinically trained study team members. Quantitative data from CHW and supervisor questionnaires as well as qualitative interviews with CHWs and supervisors are used to define CHW-, supervisor-, and facility-level drivers of acceptability, adoption, and fidelity.
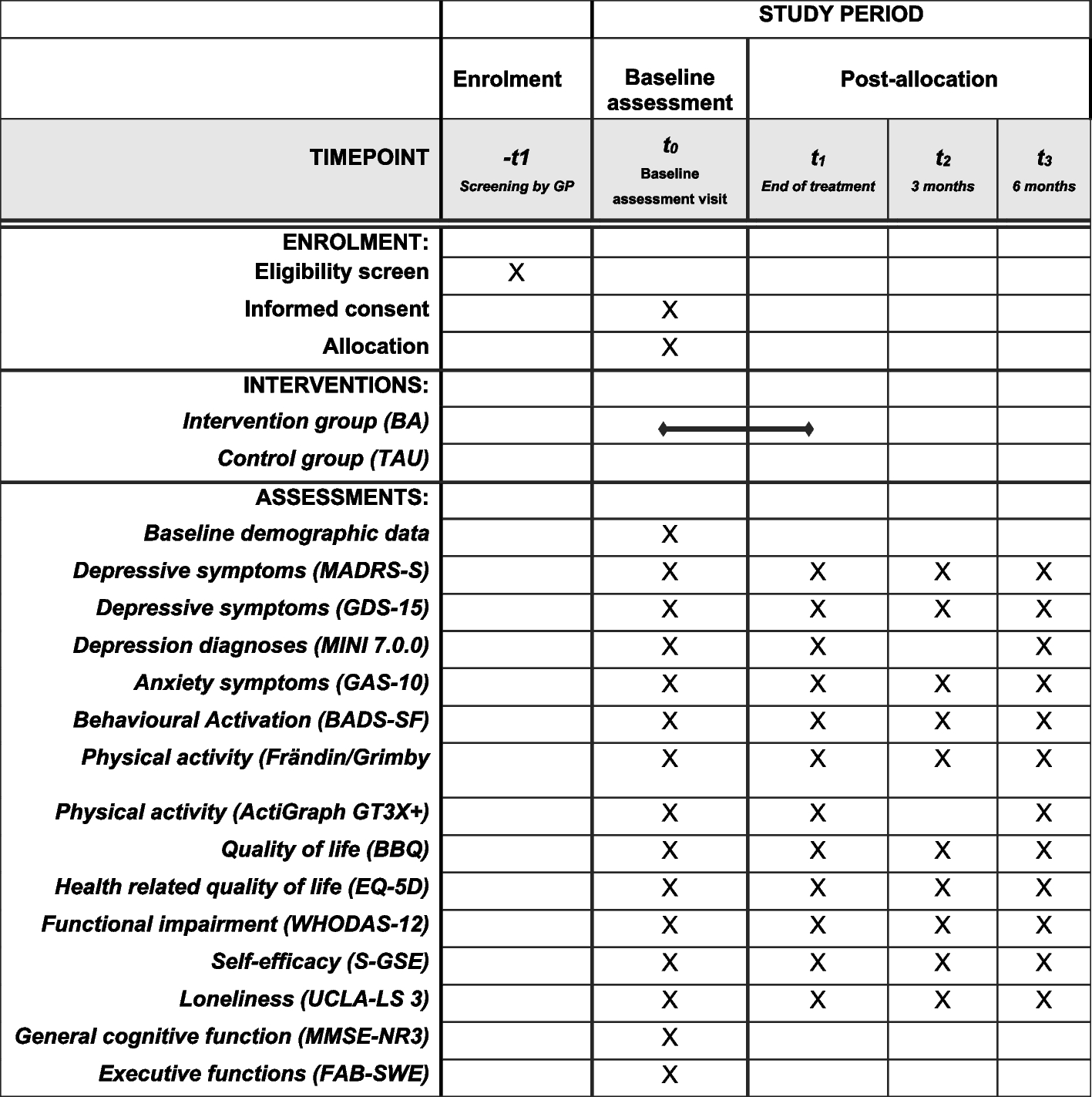
Participant timelinePeripartum women participants at control and intervention facilities complete questionnaires at enrollment into the study and at 6 weeks postpartum (Table 2). CHWs and supervisor participants complete questionnaires at study launch, 1 year after launch, and study close. CHW and supervisor qualitative interviews are conducted 1 year after launch and at study close.
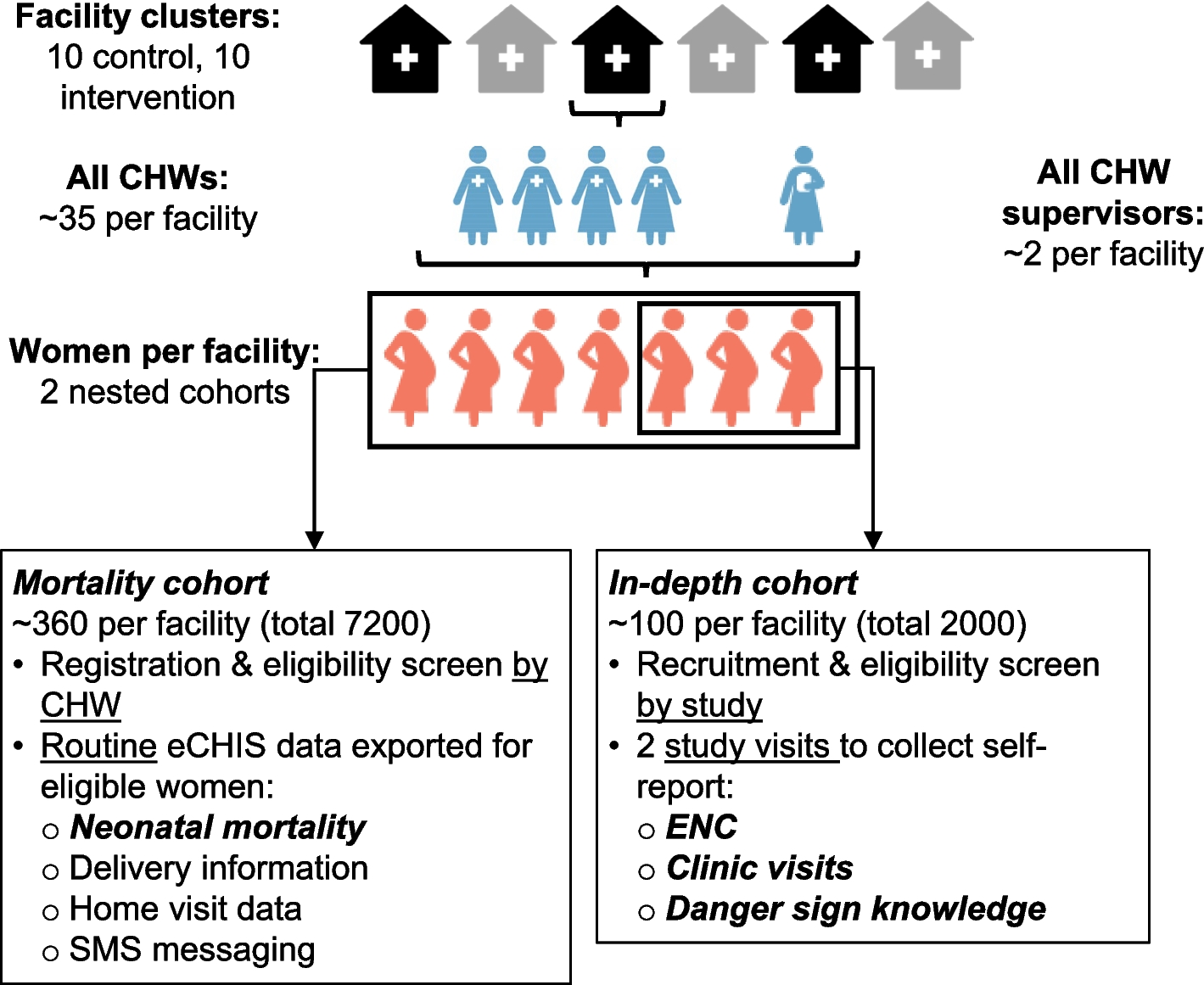
Table 2 CHV-NEO RCT participant scheduleSample sizeOur study is powered for primary and secondary clinical outcomes. The cluster-randomized trial includes 20 facility clusters, 10 interventions, and 10 controls. For ascertainment of our primary outcome of neonatal mortality, we will abstract outcomes from eCHIS on 7200 pregnancies ending in live births across the clusters. With this sample size, assuming α = 0.05, two-sided tests, 10% attrition, a conservative coefficient of variation of 0.25, and assuming unequal cluster sizes with an average cluster size 360, we have 80% power to detect a difference in neonatal mortality of 21.0 vs. 10.3 per 1000 live births [43]. For ascertainment of secondary outcomes, we will enroll 2000 pregnant clients in the in-depth perinatal cohort. With this sample size, assuming α = 0.05, two-sided tests, 10% attrition, coefficient of variation of 0.25, and unequal cluster sizes (ranging between 80 and 120 per cluster), we have 80% power to detect a difference in early initiation of breastfeeding, thermal care, and cord care of 50% vs. 72%. We expect the outcomes of appropriate care-seeking and knowledge of danger signs to be correlated so we will correct these analyses for multiple comparisons. Assuming a Bonferroni-adjusted α = 0.025, we will have 80% power to detect a difference between arms of 2.0 vs. 2.4 danger signs named and 0.5 vs. 0.9 appropriate clinic visits attended in the first 6 weeks [6, 37, 49, 50].
Service delivery and implementation outcomes are ascertained among the in-depth perinatal cohort as well as all CHWs and supervisors providing services over the 2-year period (estimated sample size 700 CHWs and 40 supervisors). Quantitative and qualitative analyses of implementation outcomes are intended to be exploratory; no formal hypothesis testing will be performed. We expect sample sizes for qualitative interviews will be sufficient to reach theoretical saturation of themes [51].
Recruitment Abstracted mortality cohortMortality is ascertained from the abstracted data from all perinatal clients enrolled in eCHIS in the study areas meeting the inclusion criteria. Clients are registered in eCHIS through CHWs’ routine home visit activities.
In-depth perinatal cohortParticipants in the in-depth perinatal cohort are recruited during ANC visits at the 20 randomized study facilities. Potential participants are approached by MCH facility staff and referred to the study staff at each clinic to obtain additional information. Study staff emphasize that participation is completely voluntary and will not affect their access to ANC, postnatal, or infant care services.
CHWs and supervisorsCHWs and supervisors at all study facilities are recruited by study staff for participation in questionnaires through facility-wide group meetings or announcements from facility leadership at study facilities. CHWs or supervisors who join the study facility part-way through the study are recruited to complete subsequent rounds of data collection (1 year or trial close). It is emphasized that participation is completely voluntary and would not in any way affect their employment.
A subset of 50 CHWs and 10 supervisors at intervention sites are selected for individual interviews 1 year after the study trial launch and at trial close. Interview participants are selected based on exhibiting below-median vs. above-median fidelity to contrast the experiences of the two groups and identify constructs associated with variations in implementation. Selected individuals are contacted through facility leadership and invited to contact the study to learn more about participation. They and facility leadership are not be told why they were selected, to avoid any negative consequences from their workplace.
Assignment of interventions: allocationSequence generation , concealment mechanism , and implementationFacility-level cluster randomization was conducted using a restricted randomization approach. Facilities were stratified into eight groups of two to six facilities, based on similar characteristics that may influence outcomes of interest, including facility level, patient volume, rural/urban designation, and services offered. Randomization was conducted through an interactive event using an online visual simulation of randomization [52]. A representative from each facility “spun” an online “wheel” to determine their order of assignment within stratified groups and a second wheel to determine final assignment within the randomization stratum.
Assignment of interventions: blindingWho will be blindedThis will be a non-blinded study. All facilities, trial participants, and analysts will have access to intervention assignment information. Study co-investigators will only review outcome data in aggregate across arms during the trial.
Procedure for unblinding if neededN/a. This study is unblinded.
Data collection and managementPlans for assessment and collection of outcomesData are collected through three primary modes: abstraction of eCHIS data, quantitative questionnaires with perinatal women, CHWs and supervisors, and qualitative interviews with CHWs and supervisors.
eCHIS data abstractioneCHIS data, including task completion and SMS messaging, is extracted directly from the eCHIS server.
Quantitative questionnairesQuantitative questionnaires are administered electronically to women, CHWs, and supervisors by study staff using the REDCap platform. Women complete questionnaires during study visits at the facility at enrollment in pregnancy and at 6 weeks postpartum (Table 2). At each visit, a standardized questionnaire is administered to record self-reported outcomes and sociodemographic and clinical characteristics that may be associated with them. Outcomes include timing of breastfeeding initiation, introduction of complementary foods, application of substances to the umbilical cord, knowledge of eight danger signs (not feeding, high temperature, low temperature, fast breathing, difficulty breathing, not moving, convulsions, and jaundice) [53], timing of first bath, attending facility-based care during illness episodes, and acceptability of CHV-NEO, using the AIM [48]. Associated demographic and clinical factors include maternal education, income, employment, parity, distance from home to clinic, intimate partner violence, depression symptoms, past healthcare experience, parental self-efficacy, and infant sex.
CHWs and supervisors complete questionnaires annually: at study launch, 1 year, and study close (Table 2). Questionnaires include outcomes as well as demographic and professional characteristics that may be associated with outcomes. Outcomes include acceptability of CHV-NEO, assessed using the AIM measure [48], and time spent on work duties in the prior 2 weeks. Characteristics that may be associated with outcomes include professional background, training, and experience and comfort with the eCHIS platform.
Qualitative interviewsWe conduct individual semi-structured interviews with a sample of CHWs and supervisors at intervention sites 1 year after the study trial launch and at the trial close. Interview guides explore determinants of implementation success, comparing CHWs exhibiting low vs. high fidelity delivery of the intervention. Discussion guides are based on constructs from the consolidated framework for implementation research (CFIR), adapted for use in LMIC settings [54]. IDIs are conducted by a trained social scientist fluent in English, Swahili, and Luo and audio-recorded, transcribed verbatim, and translated into English.
Plans to promote participant retention and complete follow-upA study staff member is stationed at each facility and is responsible for the recruitment and follow-up of participants. Participants who are 2 weeks late for their 6-week study visit are actively traced by phone call and home visit to maximize completeness of 6-week visit data. We successfully used this approach in previous RCTs [55]. Data from participants who discontinue the study will be included in the analysis up to the point of discontinuation.
Data managementAbstracted data is collected through direct extraction from eCHIS via a secure web-based login. Data is extracted and stored on a secure University of Washington server with restricted access. Questionnaire data is collected using the REDCap online version. Personal identifying information and consent forms are stored in a separate REDCap project from study data. All REDCap projects require login and password information unique to individual study staff. Data collectors receive study-specific training on all questionnaires and surveys. A data manager reviews all new enrollments and survey entries daily using quality control reports within REDCap and confirms end-of-day enrollments and questionnaire numbers with data collectors.
ConfidentialityPersonal identifying information is only collected for the in-depth cohort, CHWs, and supervisors. Personal information is stored separately from study data. Data abstracted from eCHIS does not include client identifiers such as names or phone numbers. Data is only collected and accessed by study staff who have received human subjects and data protection training through a secure server.
Plans for collection, laboratory evaluation, and storage of biological specimens for genetic or molecular analysis in this trial/future useN/a. This study will not be collecting any biological specimens.
Statistical methodsStatistical methods for primary and secondary outcomesStatistical analysis approaches for each outcome are summarized in Table 1. Analysis of primary and secondary outcomes will be by intention-to-treat. If participants relocate between facilities in different intervention arms during the course of the study, the original assignment is used in the analysis. For analyses that include random effects at the CHW level, if a participant’s assigned CHW changes, their data is analyzed under the CHW under whose care they are for the longest proportion of follow-up time preceding outcome ascertainment. Analyses will be adjusted for any baseline characteristics that differ significantly between study arms.
Interim analysesAn interim analysis for neonatal mortality will be performed using O’Brien-Fleming boundaries for benefit and harm when 50% of expected person time has been accrued. The study’s data safety monitoring board (DSMB) will meet to review the interim analysis and may conclude with recommendations to continue the trial without change, modify the trial, or terminate the trial.
Methods for additional analyses (e.g., subgroup analyses)We have no pre-specified subgroup analyses.
Methods in the analysis to handle protocol non-adherence and any statistical methods to handle missing dataBased on the Mobile WACh NEO RCT [41], we expect a 10% loss to follow-up between enrollment and the 6-week study visit. We anticipate that women who are lost to follow-up are more likely to be disengaged from care and have experienced adverse outcomes. We also anticipate missingness may differ by arm, with the intervention arm having higher retention. A secondary analysis of mortality will be performed in which missing mortality at 28 days will be imputed using multiple imputations by chained equations (MICE).
To explore any dose–response effects associated with variation in the fidelity of intervention delivery, we will conduct an exploratory analysis comparing primary and secondary outcomes between participants who received low vs. high fidelity of the intervention, defined based on the number of automated and CHW messages received. Propensity score matching will be used to control for confounding by participant or CHW characteristics.
Plans to give access to the full protocol, participant-level data, and statistical codeDe-identified data, statistical code, and the study protocol will be made available to the public upon publication of the results.
Oversight and monitoringComposition of the coordinating center and trial steering committeeThe University of Washington, Kenyatta National Hospital, and Medic teams all contribute to trial organization and daily support. Day-to-day trial operations are undertaken by data collectors, a data manager, and a research coordinator based in Kisumu County. This team meets with the rest of the team (research coordinator, research scientists, design specialists, co-investigators, and principal investigators) weekly to report on progress and review data.
Composition of the data monitoring committee, its role, and reporting structureThe CHV-NEO study has engaged an independent Data Safety Monitoring Board (DSMB) to act in an advisory capacity to monitor patient safety and evaluate the efficacy of the intervention. The responsibility of the DSMB is to review interim safety and efficacy at periodic intervals (6-monthly intervals after initiation of the trial). The Data Safety Monitoring Board consists of physicians, statisticians, neonatologists, and digital health specialists selected by the study team. Membership consists of persons completely independent of the investigators who have no financial, scientific, or other conflict of interest with the trial. Members are not current or past collaborators or associates of the University of Washington or Kenyatta National Hospital principal investigators.
Adverse event reporting and harmsAdverse events among perinatal women, CHWs, or supervisor participants are elicited at all study visits and may also be reported spontaneously if a participant contacts the team. All adverse events are recorded by study staff using an electronic REDCap questionnaire based on a phone conversation with the participant. Events to be monitored include maternal and infant death, maternal and infant hospitalization, pregnancy loss, experience of violence, losing housing, breach of confidentiality, and suicidal behavior. Adverse event monitoring in the mortality cohort is more limited because the study will not have direct contact with these individuals. Events monitored in this cohort include maternal and infant death, pregnancy loss, and report of maternal postpartum danger signs at home visits, abstracted from eCHIS. Adverse and severe adverse events will be monitored by the study team, reported to ethical review boards as needed, and unblinded results will be reviewed by the DSMB. The DSMB will make recommendations regarding any imbalances in safety outcomes.
Frequency and plans for auditing trial conductNo audits are planned.
Plans for communicating important protocol amendments to relevant parties (e.g., trial participants, ethical committees)Modifications and amendments to study protocols are submitted to the University of Washington Institutional Review Board and Kenyatta National Hospital Ethics Review Committee before implementation. Once approved, participants are informed and re-consented at scheduled study visits, as needed, to align with updated protocols. Changes are communicated to the DSMB at regularly scheduled meetings. Trial registries are reviewed and updated by the study team yearly during the study period.
Dissemination plansWe will disseminate results to a community advisory board, made up of medical providers and community members living in the study area, twice a year. Study findings will be shared with the participating facilities, Kisumu County leadership, and Kenyan Ministry of Health at the study conclusion as a presentation or written report. Findings will be disseminated to the research community in the form of conference presentations and journal articles.
留言 (0)