
記住我


The study will be conducted at Oslo University Hospital (OUH), Dept. of Physical Medicine and Rehabilitation. OUH is the trauma referral center for the South-eastern region of Norway and has a population base of more than half of the Norwegian population. The feasibility study was conducted from autumn 2023 until January 2024, while the recruitment of patients for the RCT started in January 2024 and will continue until the required sample size has been reached. All baseline assessments will be performed at OUH, interventions either at OUH or by telehealth, while follow-ups will be performed either at OUH or by phone.
Eligibility criteriaThe study population consists of persons aged 18–72 years residing in the southeast region of Norway, who are admitted to OUH directly or within 72 h after having sustained a moderate to severe traumatic injury, defined as a New Injury Severity Score (NISS) > 9 [22], who have at least a 2-day hospital stay, and report injury-related symptoms, functional impairment, and/or difficulties with daily life activities at discharge from the acute hospital stay. Those who consent to participation and are allocated or by self-selection choose to be in the treatment group, will receive SEMPO 3–4 months after the injury.
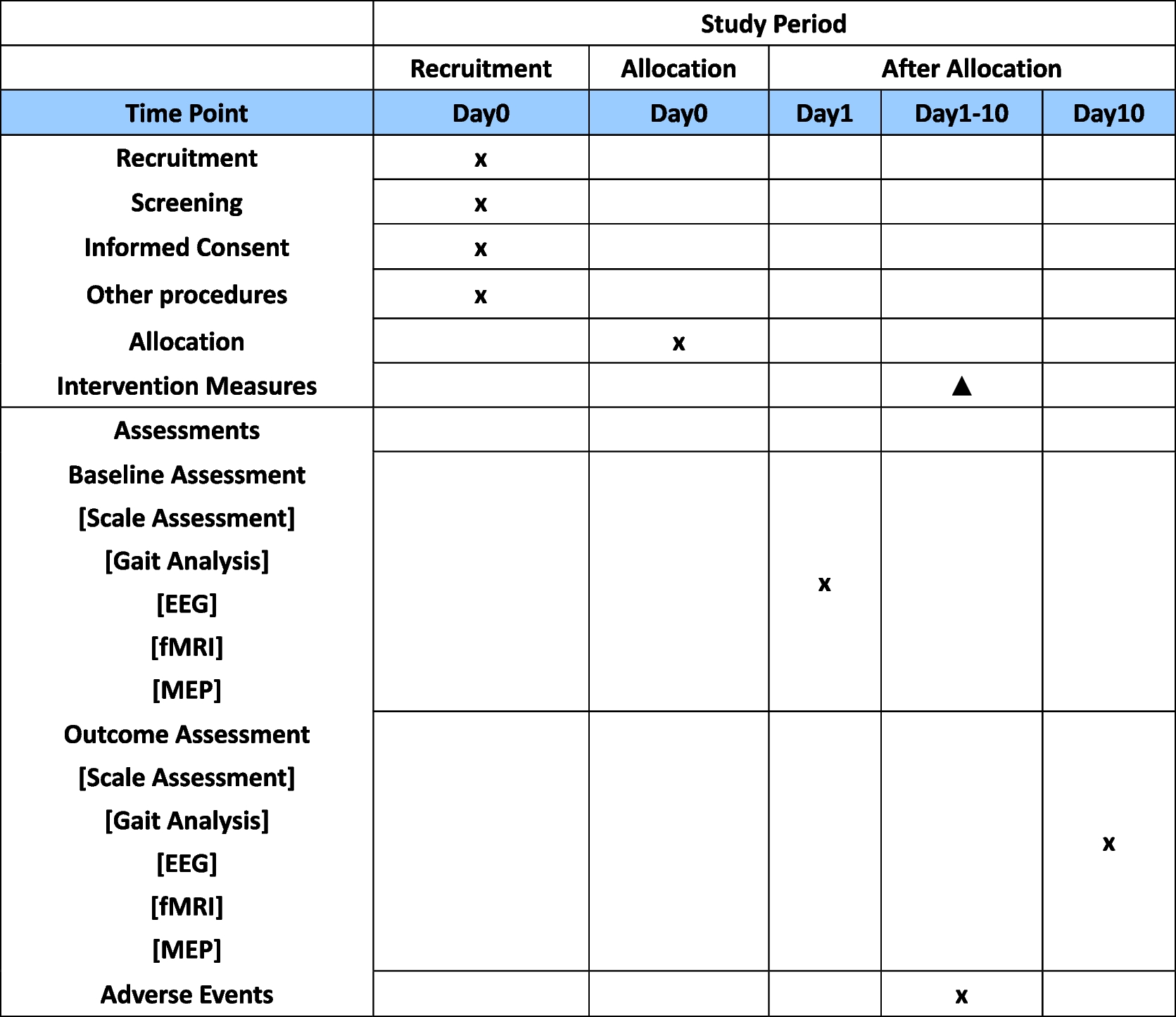
Exclusion criteria are cognitive functioning corresponding to a Mini-Mental Health Status [23] score < 20 points, severe psychiatric disease or drug/alcohol dependence requiring treatment, complete spinal cord injury or isolated abdominal or thoracic injuries, and insufficient command of Norwegian. The reason for excluding persons with complete spinal cord injuries is that these patients undergo comprehensive long-term rehabilitation of which we will not interfere. The reason for excluding persons with isolated abdominal or thoracic injuries is that a previous Norwegian longitudinal follow-up study demonstrated that these patients seldom have rehabilitation needs [24]. Severe psychiatric disease or drug/alcohol dependence requiring treatment will be excluded due to likely interference with participation and treatment outcomes (Table 1).
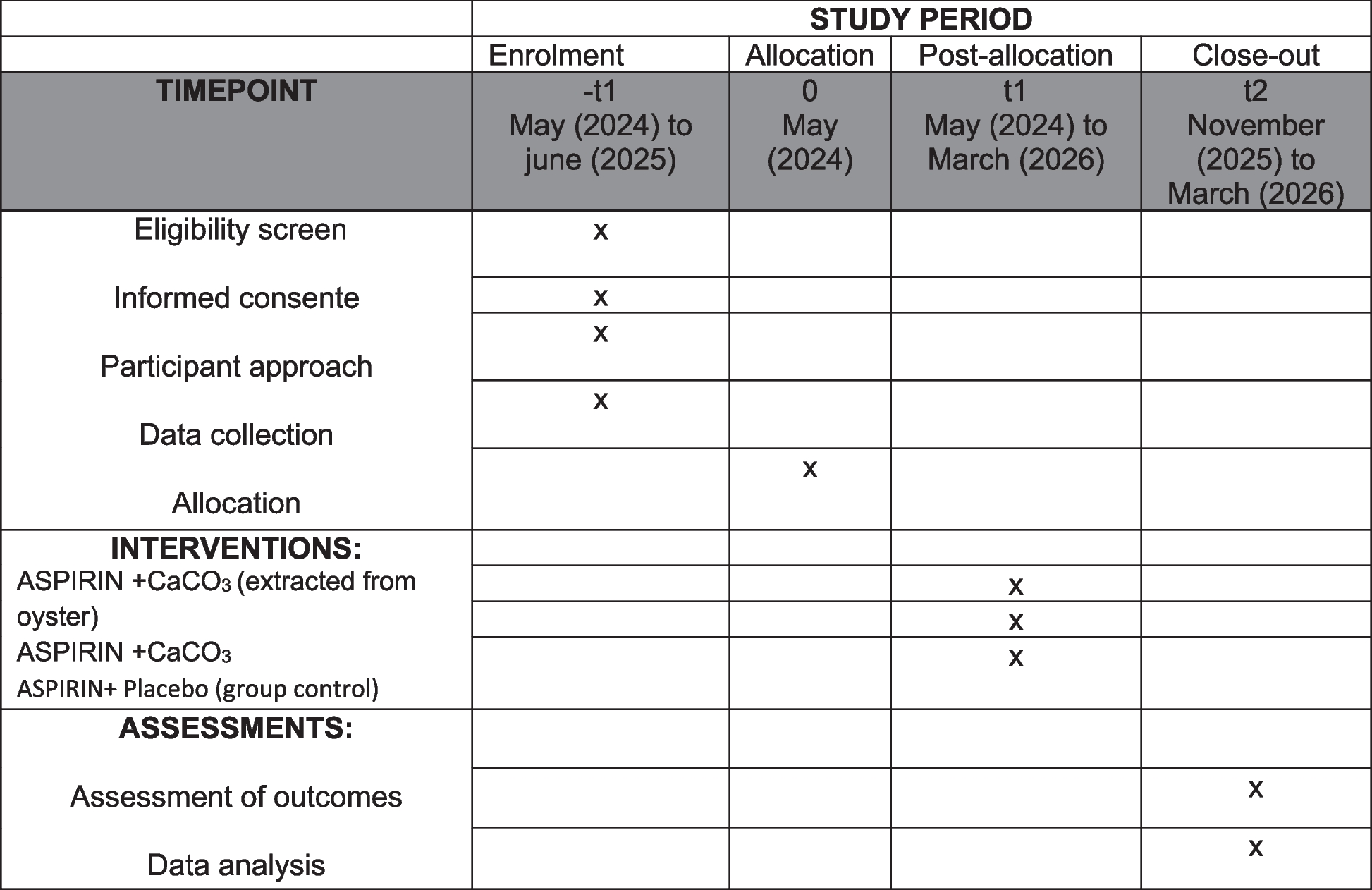
Table 1 Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT)OutcomesPatient characteristicsThe following sociodemographic variables will be registered at baseline: age, sex, marital status, educational level, living conditions, employment status, and annual income. Changes in living conditions, employment status and annual income will be recorded at the follow-ups.
Injury-related characteristicsClinical and injury-related variables included comorbidities, diverse injury characteristics, and the trauma severity scores: the Abbreviated Injury Scale (AIS), Injury Severity Score (ISS), and NISS [22], length of hospitalization and medical treatment modalities, discharge place, and symptom burden along with screening of cognitive function in patients with suspected impaired cognitive function (MMS < 20). The trauma severity scores will be validated by data registered by certified AIS registrars in the hospitals’ trauma registries.
Outcome measuresWhen evaluating the effectiveness of complex interventions, it is recommended to use more than one outcome measure [25]. As the intervention aims to improve patients’ level of self-efficacy, the Trauma Coping Self-efficacy Scale [26] was chosen as the primary outcome with the 6-month follow-up (T4) being the endpoint. Secondary outcomes comprise domains such as symptom burden, physical and cognitive functioning, emotional distress, and return to work. Patients will nominate their target problem areas in their own words [27]. They will also be asked to nominate one self-selected outcome measure based on a presented list of domain-related measurements related to fatigue, sleep, pain, physical functioning, cognition, emotional functioning, and vocation. The rationale for including a patient-preferred outcome measure to ensure participant involvement and patient-centered outcome measurement. Their preferred outcome domain will be established as their self-selected secondary outcome at baseline. Additional outcomes include health-related quality of life, resilience, disability and global functioning, and patient impression of changes. All outcome measures are validated and presented in Table 2. The Trauma Coping Self-Efficacy Scale, the communication with physicians, and the Health Literacy Questionnaire were translated into Norwegian using the established translation procedures by a professional translation service (Forward translation; Expert panel discussion; Back-translation; Final version) [28]. Data for cost-effectiveness and cost-utility will be based on patient-reporting surveys of the type and frequency of received health care services. See Table 2 for an overview of the included outcome measures.
Table 2 Description of outcome measures utilized in the RCTProcess evaluationConducting a process evaluation as part of a randomized trial is recommended by the British Medical Research Council as it can add valuable knowledge about causal mechanisms, fidelity, and contextual factors that may influence both implementation of the intervention and variations in outcomes [25, 45]. In this study, the process evaluation will be based on information from the interventionists and participants using a mixed method approach by combining quantitative and qualitative data. This includes registration of participation rate, number of consultations apart from sessions and follow-ups, and direct and indirect time use of each consultation. Further, the completion of intervention due to protocol, variations, and reasons for non-compliance will be recorded. After the completion of the SEMPO, patients will be asked to evaluate the content and their satisfaction with the intervention using a semi-structured interview form.
InterventionsIntervention group: self-management program (SEMPO)The SEMPO program was developed by experienced clinicians and researchers and is based on well-known principles from the self-management concept and established rehabilitation strategies [11, 46]. Thus, SEMPO adheres to theories of self-efficacy as a mean of coping [11, 47]. The program aims to enhance self-efficacy by strengthening patients’ skills and confidence in managing the persisting consequences of the injury, as well as enhancing their health literacy and problem-solving competence. The program integrates components from evidence-based rehabilitation strategies within relevant functional domains [48, 49] to fit the symptom burden of the trauma population. User involvement was an essential part of the development of the intervention, and we collaborated with a user panel consisting of persons living with persistent injury-related consequences and representatives from the involved user organization, the National Association of the Traumatically Injured (LTN). In addition, the program has been adjusted after feedback from a test trial of the intervention (n = 5 persons), where patients were interviewed at the end of the testing regarding perceived usefulness and feedback on program content.
The SEMPO is delivered through 8 weekly 2.5-h sessions to groups consisting of 4–7 patients. A group format is chosen because social encouragement is considered a powerful means of increasing self-efficacy, thus SMS intervention delivered in groups is regarded as effective for behavior change, skills enhancement, and modeling [11]. Different components, such as psychoeducation, guided skills mastery, learning and practicing helpful compensatory strategies, and problem-solving techniques are integrated. In the weekly group sessions, topics with tailored psycho-educative content are presented and action plans reviewed, modified, and discussed in the group to help with problem-solving and address challenges. The manual will provide a fixed framework for the intervention, but action plans will be individualized and based on self-reported problems and individual challenges. In each session, patients will establish their own action plans containing achievable short-term weekly goals and related strategies. The program also includes a workbook, containing material from each session, self-monitoring schemes of weekly goal setting and goal attainment, as well as practice tasks between sessions (e.g., problem-solving of personal difficult tasks, strategy training of emotional worries). According to Bandura’s theory of self-efficacy [47], these ingredients may enhance a person’s self-confidence in managing trauma-related symptoms, problems in daily life activities, and participation. A tele-health version of the SEMPO intervention will be available for patients who prefer this or have to travel long distance to the hospital. In the tele-rehabilitation version, all participants will attend digitally, and the intervention will be delivered with the same content, frequency, and in-group mode. An overview of the intervention topics is displayed in Table 3.
Table 3 Overview of the intervention topicsCriteria for discontinuing or modifying allocated interventionsThe intervention will be delivered by a multidisciplinary team including medical doctors, psychologists, and physical therapists, all trained in self-management support strategies by Bridges Self-Management [50]. In any case of adverse effects of the intervention or in case of detected medical or psychological health problems in need of treatment, suitable actions will be discussed and ensured by the research team. A procedure for handling severe psychiatric conditions is included in the project, where the therapist will immediately consult with senior researchers who are specialist medical doctors and/or psychologists for further management.
Relevant concomitant care permitted or prohibited during the trialPatients will not be withdrawn from any concurrent treatment during the trial.
Control group: treatment as usualThe control group will receive the usual health care and rehabilitation services provided in the municipality or other rehabilitation settings. Such services will potentially vary greatly depending on the patient needs and advice they receive at hospitals and services available in their municipalities, ranging from no services to regular contact with specialized or local rehabilitation teams. The services provided will be logged at baseline for all participants allowing comparison with the intervention group at all time-points in terms of content, extent, professionals involved, etc.
Sample sizeThe sample size was estimated based on the primary outcome, the Trauma Coping Self-Efficacy Scale questionnaire [26]. The questionnaire is a 9-item scale answered on a scale ranging from 0 (not capable) to 7 (totally capable). A mean difference in the Trauma Coping Self-Efficacy Scale of 0.6 between baseline and follow-up between the groups is considered as a clinical relevant difference (ref). In order to detect a mean between-group difference of 0.6 with an estimated standard deviation of 1, equal allocation to both groups, 80% power, and a significance level of 5%, we will need to include a minimum of 45 patients in each group and a total of 90 participants [51]. With an assumed attrition rate of 20%, 110 patients will be included (i.e., 55 patients in each group). The sample size calculation was done based on the classical randomization arm (RA), and we aim to achieve the same power in the self-selection (SA) arm. However, the SA is considered an exploratory part of this study to evaluate the influence of patients’ treatment preferences. According to a previous longitudinal study at OUH, approximately 310 patients with trauma-related disability from 18 to 72 years of age may meet the inclusion criteria [52]. Based on previous studies, approximately 70–80% will be eligible for inclusion, resulting in 218–249 eligible patients per year.
RecruitmentPatient recruitment is performed in collaboration with staff at the Department of Traumatology at OUH and the physicians allocated to the project through participation in the trauma report meetings and from lists of new hospitalized patients registered by the Department of Traumatology. One of the PhD candidates and a member of the project group (JNS + TH) will provide written and oral information to eligible patients, and those who agree to participate will be included upon discharge from the acute hospital stay or contacted by phone in cases of early discharge.
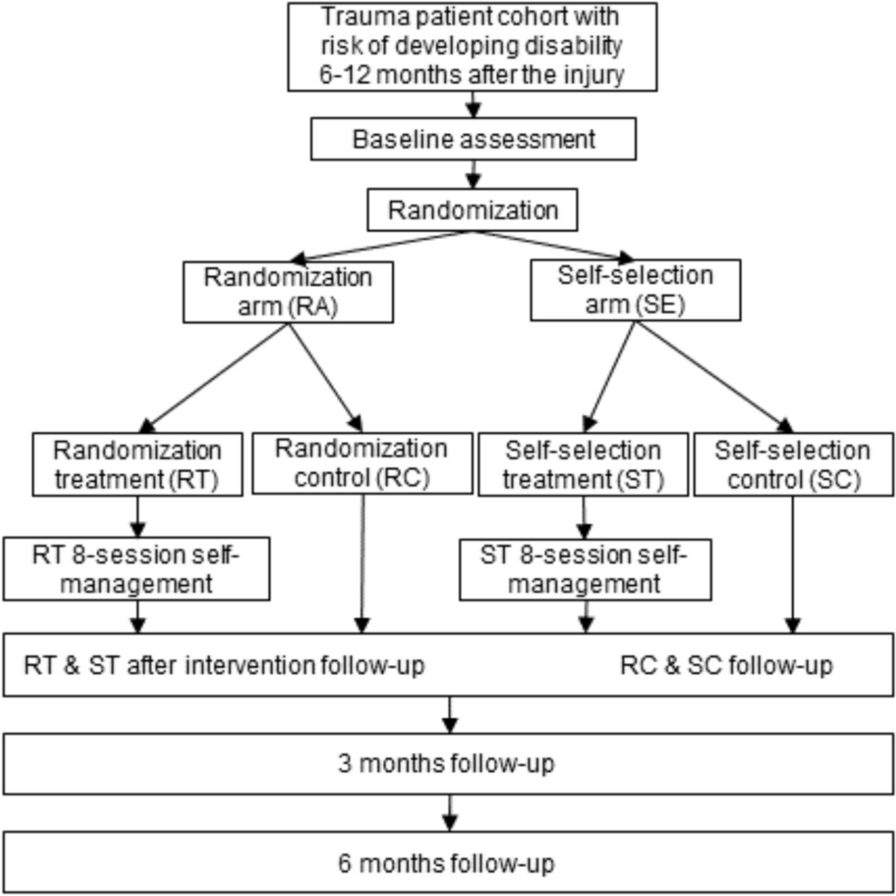
Allocation/randomizationSequence generation and allocation concealment mechanismThe allocation sequence will be computer-generated by VieDoc using permuted blocks with varying block sizes. Patients will be randomized immediately after baseline assessment to RA or SA (see Fig. 1). Patients allocated to the RA will further be randomized to the intervention and control group, while patients randomized to the SA will self-select allocation to either intervention or control group.
Fig. 1 Implementation
ImplementationEligible patients will be identified by project researchers (authors JSN and TH) in close collaboration with clinical staff at the Department of Traumatology at OUH.
Blinding/maskingBlinding of interventionists or patients will not be possible, but outcome assessors will be blinded for study allocation at follow-ups (T2–T4). The data analyst will be unaware of group allocation during the statistical analyses by assigning dummy codes to the study arms.
留言 (0)