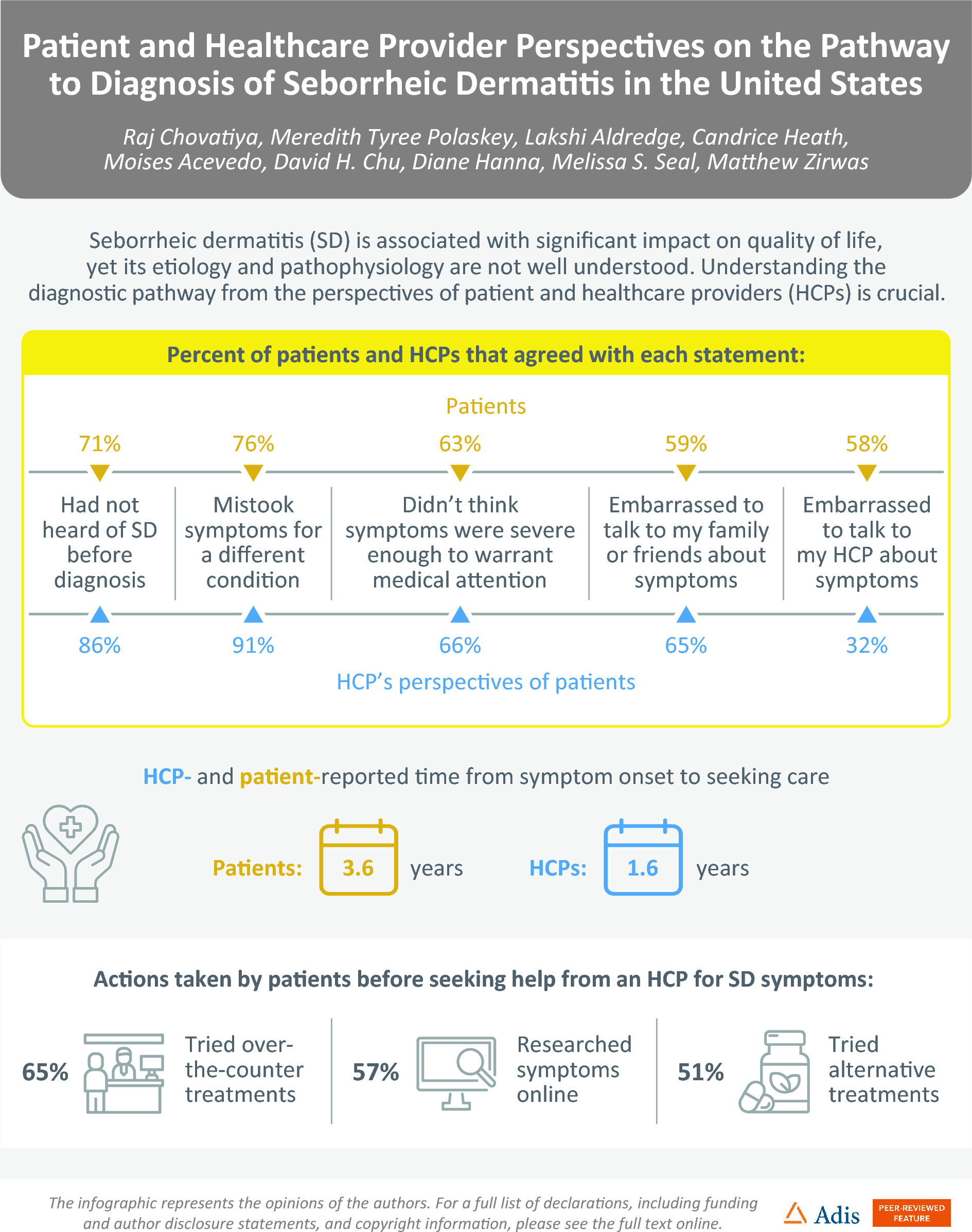
This study represents the first comprehensive exploration of the diagnostic and management pathways of SD from both the patient and HCP perspectives. We discovered a significant delay in patients seeking medical attention for their SD, with an average wait time of 3.6 years. This delay contrasts sharply with the more prompt response seen in other common inflammatory dermatologic conditions like psoriasis, where patients typically seek care within 3 months [11,12,13]. A majority of patients reported feeling embarrassed to discuss their SD symptoms with HCPs, which has been associated with delays in seeking medical care for a variety of conditions [14]. However, our results suggest that HCPs may significantly underestimate how much this factor impacts patients with SD.
Additionally, these findings indicate a prevalent attitude among patients that their symptoms do not warrant medical attention and in some cases may be considered a cosmetic condition, accompanied by a tendency towards self-management. Before consulting HCPs, patients commonly attempted to treat their symptoms independently, with an average of six over-the-counter treatments used. This tendency to self-manage and downplay the condition aligns with behaviors observed in hair loss disorders, where patients may frequently feel their symptoms do not warrant medical intervention, or in acne or fungal infections, where self-treatment is a common initial response [15]. These patterns mirror a wider tendency in dermatology for patients to downplay or delay addressing their own symptoms if perceived as medically non-urgent, despite their potential significant emotional and psychological impact [16,17,18].
Despite often being seen as a mild condition, SD is associated with considerable implications for QoL, particularly in female and younger patients [3,4,5, 19]. Feelings of shame, embarrassment, and self-consciousness are common among patients with SD, as are practical considerations like impacts to clothing choices [19], with significant emotional impact reported by nearly half of patients with SD in a large study from China [20].
However, the results of the present study highlight a disparity in HCPs’ understanding of patient experiences with SD. HCPs tended to overestimate the number of patients who were unaware of their SD symptoms or who mistakenly attributed symptoms to a different condition, while also frequently underestimating the duration of symptoms before patients sought care. This gap suggests a need for improved HCP awareness about the lived experiences of individuals with SD and points to the importance of enhancing patient-HCP communication.
Furthermore, we observed a striking disconnect between patient-reported symptom severity and the assessments of HCPs. Although 71% of patients reported their symptoms as moderate severity, HCPs estimated this figure to be substantially lower at 41%. This discrepancy suggests that the visible signs of SD might not accurately reflect symptom severity, a finding consistent with observations in atopic dermatitis, where patients with mild lesions can still experience increased disease severity due to non-visible disease burdens [21]. SD symptoms that are often clinically classified as mild may, in fact, impose a significant burden, highlighting the need for HCPs to recalibrate their perceptions to align more accurately with patient experiences.
This study sheds light on the challenges patients face in seeking information and guidance for SD. Although many patients reported a lack of familiarity with SD, there was a clear indication of their active pursuit of information, with the majority of patients researching their symptoms on the internet. However, scarcity of accurate and accessible information could drive patients to resort to less credible online resources for self-diagnosis and symptom management. Evidence suggests that patients are more likely to consult videos about SD on social media platforms where content is predominantly non-HCP-made, often featuring inaccurate and non-educational information [22]. This pattern is consistent with broader trends in dermatology, where patients frequently use online resources to address their skin conditions, impacting their willingness to seek professional medical care [23]. Self-treatment, despite its prevalence, has been linked to worse outcomes in dermatology [24], underscoring the need for improved access to trustworthy and accurate medical information.
Interestingly, the findings revealed that non-HCPs often play a crucial role in the initial identification of SD, emphasizing the importance of community awareness and knowledge about SD. Family members, nutritionists, hairstylists, barbers, estheticians, and others with SD or similar conditions were instrumental in recognizing symptoms in many patients, highlighting the value of support groups and community networks as vital resources. These findings suggest a need for public health education to facilitate earlier detection and treatment while also addressing and potentially reducing stigma, a strategy that has proven effective in several other medical conditions [25,26,27].
Despite a common perception that SD is straightforward to diagnose, these data suggest a more complex reality. Notably, 74% of the patients referred by non-dermatology HCPs received an initial misdiagnosis, highlighting a gap in SD recognition among general healthcare practitioners. The symptoms of SD can sometimes be confused with other skin conditions like psoriasis, atopic dermatitis, or rosacea [28], and its diagnosis can be particularly challenging in darker skin tones [29]. Additionally, our findings show that although most patients prefer seeing dermatology HCPs for SD management, they often consult > 2 HCPs, indicating a journey through multiple healthcare touchpoints before receiving effective treatment. These insights emphasize the need for enhanced training and awareness among all HCPs, advocating for a multidisciplinary approach in early SD detection and referral, especially in diverse populations where symptom presentation can vary significantly.
Limitations of the current study include potential challenges in fully capturing the diverse experiences and behaviors of individuals affected by SD using a cross-sectional online survey method. The weighting of demographic data might not completely account for the varied nuances in patient experiences across different demographic groups, and the self-reported nature of the survey could introduce bias in the responses. Insights from this study indicate a need for further prospective research focused on patient and HCP perspectives to inform better healthcare practices.





留言 (0)