Study Design
PIONEER REAL UK was a 34–44-week, non-interventional, multi-centre, phase 4, prospective, single-arm clinical study assessing use of oral semaglutide in adults with T2D in clinical routine practice. List of centres and physicians can be found in Supplemental Table S1. Participants received oral semaglutide based on the treating physician’s and participant’s decision; the decision to prescribe oral semaglutide preceded recruitment to participate in the study. Data were collected in accordance with local clinical practice without any additional diagnostic or monitoring procedures. The study protocol was approved by the UK National Health Services Health Research Authority (NHS HRA) and the Medicines and Healthcare products Regulatory Agency (MHRA) after review by the London-Chelsea Research Ethics Committee (for all sites). The study was conducted following good pharmacoepidemiology practices (GPP) [20] and good pharmacovigilance practices (GVP) [21] in accordance with the Declaration of Helsinki [22]. All participants signed an informed consent. Similar methodologies have been presented elsewhere in the other PIONEER REAL studies in different countries [15,16,17,18,19].
Participants
Adults with T2D were eligible for inclusion if a decision to initiate oral semaglutide treatment had been made, they were treatment naïve to injectable glucose-lowering drugs and had an available HbA1c value ≤ 90 days prior to visit 1 or taken at visit 1 in line with local clinical practice. All participants were ≥ 18 years old and could be male or female.
Study Procedures
Baseline data were collected either at the time of oral semaglutide prescription at visit 1 or from existing records collected prior to visit 1. Oral semaglutide dose titration and other treatment decisions were at the treating physician’s discretion. All data were collected in an electronic case report form (eCRF). The first visit occurring between weeks 34 and 44 was recorded as the end of study (EOS) visit. If an HbA1C value was not recorded during the 34–44-week window, the first available result thereafter was recorded. Any visits between visit 1 and the EOS visit were categorised as intermediate visits. If a participant discontinued oral semaglutide treatment, information on circumstances was recorded as close to the stopping date as possible. Unless consent was withdrawn, data collection continued until EOS regardless of treatment status.
Endpoints and Assessments
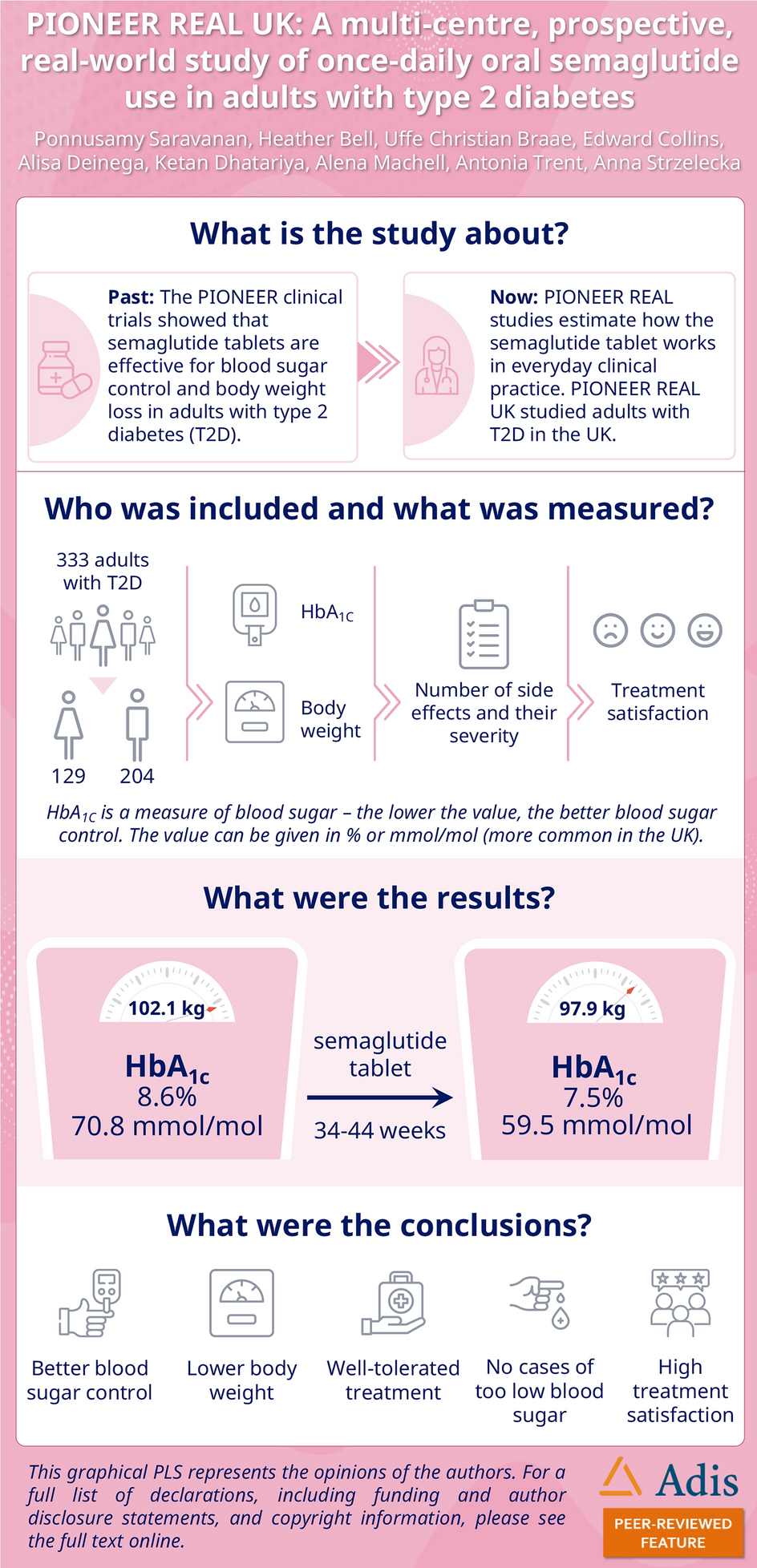
The primary endpoint was %-point change in HbA1C from baseline to EOS. Secondary endpoints were relative (%) and absolute (kg) change in body weight from baseline to EOS, proportion of participants with an HbA1C level < 7% (53 mmol/mol) at EOS, composite endpoints of HbA1C reduction ≥ 1%-points (approximately 11 mmol/mol) combined with body weight reduction of ≥ 3% or ≥ 5% from baseline to EOS and participant reported outcomes of change in relative (Diabetes Treatment Satisfaction Questionnaire change, DTSQc) and absolute (Diabetes Treatment Satisfaction Questionnaire status, DTSQs) treatment satisfaction at EOS. Exploratory endpoints included oral semaglutide dose (mg/day) at EOS, proportion of participants treated with oral semaglutide at EOS, addition of new glucose-lowering medication or increased dose of baseline glucose-lowering medication (other than oral semaglutide) during the study period, removal of glucose-lowering medication or reduced dose of baseline glucose-lowering medication during the study period, clinical success as assessed by physician at EOS, change in waist circumference (cm) from baseline to EOS and self-reported severe hypoglycaemia during the study period. Additionally, the change in HbA1C was analysed stratified by baseline HbA1C (< 7.0, ≥ 7 to < 8.0, ≥ 8.0 to < 9.0 and ≥ 9.0% or < 53, ≥ 53 to < 64, ≥ 64 to < 75 and ≥ 75 mmol/mol) and diabetes duration (≤ 1, > 1 to ≤ 5, > 5 to ≤ 10 and > 10 years) while the change in body weight was analysed stratified by baseline HbA1C, BMI (≥ 25 to < 30 and ≥ 30 kg/m2) and diabetes duration.
Subgroup Analysis
The study included a subgroup analysis on participants with a glucose-lowering treatment regimen of metformin and one OAD immediately prior to initiating oral semaglutide. Full definition of the subgroup is included in Supplementary Material and Methods. All endpoints mentioned in the above section except for HbA1C and body weight stratified by baseline data were analysed for the subgroup as well as the full analysis set (FAS).
Statistical Analysis
The sample size was determined based on a 90% probability of obtaining a 95% confidence interval for the primary endpoint of mean change in HbA1C from baseline with a half-width of maximum 0.30, assuming a SD of 1.7%. Based on these assumptions, 145 participants were needed for analysis. However, since data were collected as part of routine clinical practice, it was expected that only 75% of participants would have an EOS HbA1C measurement. Therefore, the sample size was increased to 194. Furthermore, the inclusion of a subgroup analysis of participants with baseline metformin and one OAD immediately prior to initiation of oral semaglutide had to be accounted for, and these participants were assumed to constitute 51% of participants (based on market research findings). To ensure sufficient power for the primary endpoint analysis in the subgroup, the plan was to enrol a total of 381 participants.
FAS included all eligible participants who signed the informed consent and initiated oral semaglutide treatment. During the ‘in-study’ observation period, participants were considered in the study regardless of potential discontinuation of oral semaglutide treatment, while participants were considered treated with oral semaglutide during the ‘on-treatment’ observation period. Primary analysis of the primary, secondary and exploratory endpoints was based on the FAS and in-study observation period while the secondary analysis of the primary, secondary and exploratory endpoints was based on the FAS and on-treatment observation period. For the stratified HbA1C analyses, all participants in the FAS with at least one post-baseline HbA1C in the in-study observation period were included while all participants in the FAS with at least one body weight measurement in the in-study observation period were included in the stratified body weight analyses. If number of subjects in a category was < 30, the category was combined with the corresponding next or preceding level.
While the EOS visit could take place anywhere between weeks 34 and 44, the analyses of HbA1C and body weight change from baseline to EOS were estimated from baseline to week 38. For other endpoints, data from EOS visit were used. It should also be noted that not all participants had data available for all analyses; therefore, the n varies between endpoints and is reported with the results.
Random coefficient mixed model for repeated measurements (MMRM) with random intercept and time (slope) based on the in-study observation period was used for primary analysis of the primary endpoint. Secondary analysis of the primary endpoint was otherwise similar but based on the on-treatment observation period. All MMRM models were performed both as crude and adjusted models. Crude models were adjusted for baseline values of the dependent variable, i.e. baseline HbA1C or body weight, respectively. Covariates included in the adjusted analysis of the primary endpoint were baseline HbA1C, age and BMI as well as time and time square. A sensitivity analysis of the primary endpoint was completed using a pattern-mixture model (PMM) fitted to all participants in FAS and in-study observation period. Additional post hoc sensitivity analyses, similar to the primary analyses, were performed where participants with an EOS visit outside of weeks 34–44 were excluded because their EOS visit was affected by the COVID-19 pandemic.
MMRM or analysis of covariance (ANCOVA) was used for primary and secondary analyses of secondary and exploratory continuous endpoints. Primary analyses were based on the in-study observation period while secondary analyses were based on the on-treatment observation period. Continuous secondary endpoints relative and absolute change in body weight as well as the exploratory endpoint waist circumference were analysed in the same manner as the primary endpoint. Change from baseline to EOS in DTSQs and EOS score for DTSQc were analysed using an ANCOVA model. For secondary and exploratory categorical endpoints, proportions at EOS are displayed. HbA1C stratified by baseline HbA1C and diabetes duration as well as body weight stratified by baseline HbA1C, BMI and diabetes duration are presented as the adjusted mean estimated change from baseline to week 38 with 95% CI based on MMRM and a p-value testing the null-hypothesis of no change in HbA1C and body weight, respectively. All statistical analyses were also performed separately for the subgroup. All statistical analyses were performed using SAS, Version 9.3 (SAS Institute, Cary, NC). All statistical testing was two-sided with a significance level of 0.05.





留言 (0)