
記住我




Follicular lymphoma (FL) is a lymphoproliferative neoplasia typically considered incurable. It is most often characterized by a slow, indolent disease course with a long-estimated survival period that may span decades [1, 2]. However, even with new therapies, progressive disease events are associated with markedly poorer clinical outcomes, requiring intensified therapy [3, 4]. As of currently, no biomarker or risk model has yet been able to reliably predict patient outcome; thus, the need to identify predictive biomarkers remains. Progression of disease within 24 months of initial FL diagnosis (POD24) has emerged as a strong prognosticator in FL patients, associated with poorer outcomes [5,6,7]. POD24 may serve as a useful tool in identifying high-risk FL patients, however, challenges remain, as POD24 is a post-treatment endpoint, and so, cannot be used to guide upfront treatment decisions [6,7,8]. The introduction of the CD20-targeting antibody rituximab in standard treatment regimens for FL has led to impressive improvements in patient outcomes, both regarding overall survival (OS) and the reported incidence of progression and histological transformation [1, 9]. With the present study, we aimed to describe real world data on POD24 in a national Danish cohort of FL patients diagnosed in the rituximab era, divided into POD24-positive (POD24-pos) and POD24-negative (POD24-neg) patients, in relation to risk factors and outcome.
Patients diagnosed with biopsy-proven FL in Denmark between January 2005 and July 2020 were identified through the Danish National Pathology Registry [10] and the Danish Lymphoma Registry [11], yielding 3366 patients, Fig. 1. Pathology reports of all patients were reviewed based on the existing WHO classification, updated in 2017, leaving 3146 patients to be included [2]. For analyses in the present study, we excluded patients with discordant/composite disease, as well as patients with a primary diagnosis of FL grade 3B resulting in 2422 patients. Patients allocated to a watch-and-wait strategy were excluded as well as those who passed away within 24 months from treatment initiation without a POD24 event. POD24 was defined as primary refractory disease, disease progression, transformation, or relapse within 24 months from treatment initiation. Cases of transformation were based on histologically-assessed biopsies. A total of 2389 patients had registered data eligible for POD24 analyses based on this definition, Fig. 1. Of these, 1836 patients (77%) were POD24-neg, while 553 patients (23%) were POD24-pos. The median follow up time was 6 years. Clinicopathological data on a subset of the present study population has previously been described by Madsen et al. [12]. To ensure that study cases were selected from the time after systematic nationwide rituximab treatment was adopted throughout Denmark, and to avoid inconsistencies in the introduction-phase, only patients diagnosed from 2005 onwards were included. The study was approved by the Danish National Committee on Health Research Ethics (1-10-72-276-13) and the Danish Data Protection Agency (1-16-02-407-13).
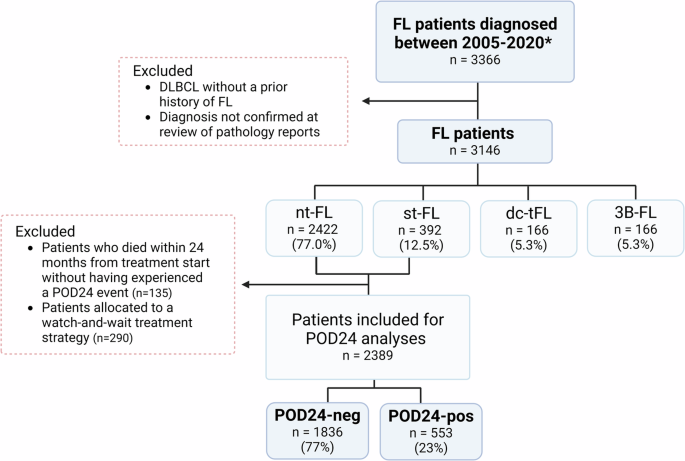
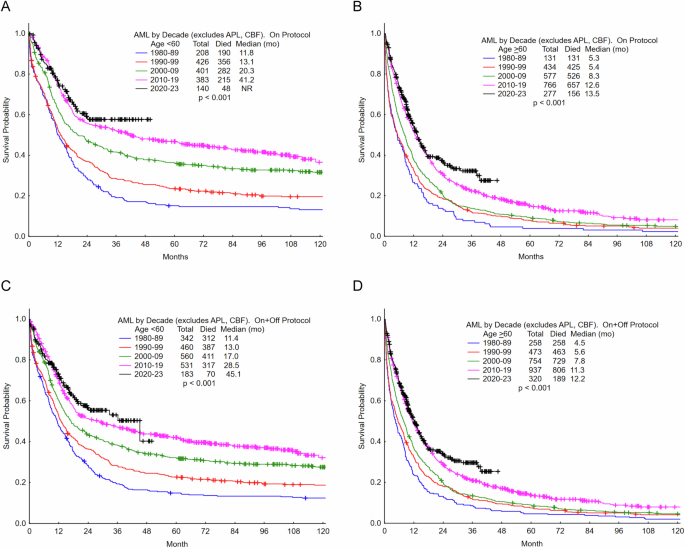
Fig. 1: Overview of the study cohort.
*Not included if not registered in both the Danish Lymphoma Registry and the Danish Pathology Registry. The study cohort consisted of a total of 3,146 patients diagnosed with FL in Denmark between 2005–2020. From these, patients with data registered eligible for the POD24 analyses were identified, resulting in 2389 cases. Thus, the final study cohort consisted of 1836 POD24-neg patients and 553 POD24-pos patients. 3B-FL primary diagnosis of FL grade 3B, dc-tFL discordant/composite transformed FL, DLBCL diffuse large B cell lymphoma, FL follicular lymphoma, POD24 progression of disease within 24 months of diagnosis, nt-FL non-transforming FL, POD24-neg POD24-negative patients, POD24-pos POD24-positive patients, st-FL subsequently-transforming FL.
Patient characteristics were compared using a chi-squared test. Time-related endpoints were analyzed using the Kaplan Meier and log rank method with OS or progression-free survival (PFS) as endpoints. OS from a risk-defining event was defined as survival from time of a progression event for POD24-pos patients and 24 months after treatment initiation for POD24-neg patients [7]. PFS was defined as time from diagnosis to progression, relapse, transformation, or death. Cutoff values were determined by a ROC analysis with the optimal cutoff point calculated using Youden’s index. Potential confounders and factors of potential relevance regarding risk of POD24 were selected based on the current literature and available recorded clinicopathological data in the Danish Lymphoma Registry. The effect of these covariates on the cause-specific hazards was estimated in both a univariate and an adjusted multivariate analysis using a Cox proportional hazards model. The mice package in R was used for multiple imputations to account for missing values under the assumption that data were missing at random. P-values below 0.05 were considered statistically significant. All statistical analyses were performed using R Statistical Software (version 4.1.2).
The study included 49% males and 51% females with a median age at FL diagnosis of 65 years (range 22–93), Supplemental Table S1. In total, 73% of patients were treated with rituximab, and the majority of patients allocated to a chemotherapy-based strategy received it in combination with rituximab. The median time to treatment initiation was 28 days (range 0–1056 days), with POD24-pos patients receiving treatment at an earlier time point than POD24-neg patients (p = 0.023), which may reflect the more adverse clinical presentation, Supplementary Table S1. Noticeable, rituximab maintenance was administered to 27% of the POD24-neg group compared to 12% in the POD24-pos group. To investigate whether the POD24 difference related to the number of patients receiving rituximab maintenance, analyses were re-run excluding patients who received rituximab maintenance. This yielded an overall POD24 distribution of 72% POD24-negative patients and 28% POD24-positive patients (versus 77 and 23%, respectively, before exclusion). Analyses from Table S1 showed comparable results independently of excluding R maintenance-treated patients with the exception of high Ann Arbor stage in which the 52% of POD24-negative group had Ann Arbor stage III-IV as compared to 73% before the exclusion. In the POD24-pos group, 120 patients (22%) experienced histological transformation within the first 24 months, with 103 patients (19%) experiencing transformation as the initial POD24 event. Of the remaining 433 POD24-pos patients, 69 patients (16%) experienced transformation after the time period of 24 months. Among POD24-neg patients, 172 (9%) of patients experienced transformation after the 24-month time period.
Generally, POD24-pos patients presented with more adverse risk profiles at diagnosis compared with POD24-neg patients with differences in FLIPI risk scores (p < 0.001), Ann Arbor stage (p < 0.001), LDH-elevation (p < 0.001), number of involved nodal sites (p < 0.001), bone marrow involvement (p < 0.001), extra-nodal disease (p < 0.001), β2-microglobulin (β2m) levels (p = 0.027), and leukocytosis (p < 0.001), Supplementary Table S1. In Denmark, β2m was not routinely measured at FL diagnosis throughout the study period, which is reflected by the large number of missing values. Thus, in these analyses, there is a risk of selection bias in those patients who were selected for β2m measurement by the treating physician. In a univariate analysis between POD24-neg and POD24-pos patients, the cause-specific hazard ratios (HRs) showed marked differences in parameters associated with aggressive disease, including high FLIPI risk scores (HR 1.69, p < 0.001), age above 60 (HR 1.48, p < 0.001), Ann Arbor stage III-IV (HR 1.39, p = 0.005), nodal involvement (HR 1.20, p = 0.036), hemoglobin levels (HR 1.33, p = 0.018), LDH-elevation (HR 1.42, p < 0.001), extra-nodal disease (HR 1.33, p < 0.001), performance score of 2 or greater (HR 2.12, p < 0.001), and β2m-elevation (HR 1.59, p < 0.001), Fig. 2A. Following multivariate analysis, high FLIPI risk scores (HR 1.33, p = 0.007), age above 60 years (HR 1.71, p < 0.001), Ann Arbor stage III-IV (HR 1.55, p = 0.006), LDH-elevation (HR 1.40, p = 0.003), performance score of 2 or greater (1.75, p = 0.008), and β2m-elevation (HR 1.47, p < 0.001) retained their significant impact as well as. Of note, grade 3 A (HR 1.12, p = 0.002) became significantly associated to POD24, though with a low HR. Surprisingly, bone marrow involvement (HR 0.73, p = 0.024) became significantly inversely associated with risk of POD24.
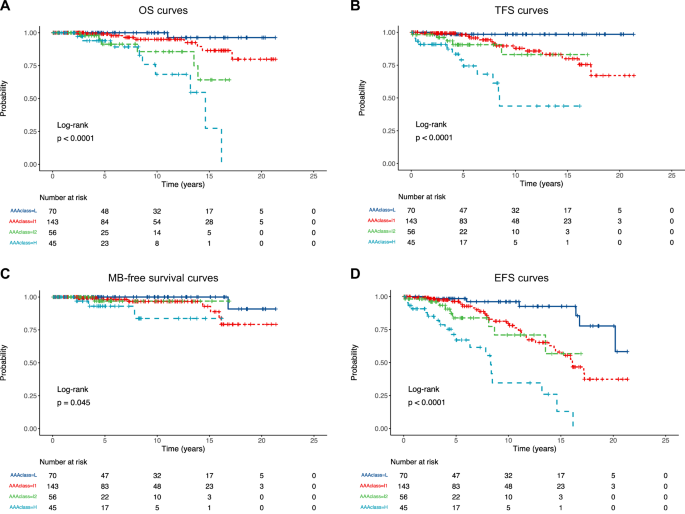
Fig. 2: Risk factors and survival for POD24.
A Hazard ratios and forest plots comparing clinicopathological factors between POD24-neg and POD24-pos patients. Multivariate analysis was performed with imputated missing values under the assumption that data were missing at random. *Adjusted for risk factors not included in the FLIPI score. B Overall survival from a risk-defining event was defined as survival from time of a progressive event for POD24-pos patients and 24 months after treatment initiation for POD24-neg patients. C Progression-free survival in the POD24-neg patient group. β2m β2-microglobulin, BM bone marrow, CI confidence interval, FL follicular lymphoma, FLIPI follicular lymphoma international prognostic index, HR hazard ratio, LDH lactate dehydrogenase, NA not applicable, NS not significant, OS overall survival, PFS progression-free survival, POD24 progression of disease within 24 months from diagnosis, R rituximab.
The ten-year OS in the entire cohort was 81%, with 86% in the POD24-neg group and only 66% in the POD24-pos group. Inferior outcome was observed among POD24-pos patients compared with POD24-neg patients in terms of OS from a risk-defining event (p < 0.001), Fig. 2B. However, with the predefined criteria stating that the POD24-neg comparison group had to be alive for the first 24 months after treatment initiation, one should consider the risk of introduced immortal time bias. In total, 135 patient were excluded from the total cohort based on this criteria. The five-year PFS for the POD24-neg group was 82%, Fig. 2C.
We analyzed real-world data for the event of POD24 in Danish FL patients diagnosed in the rituximab era. In this cohort, the incidence of POD24 during the study period was 23%, which is in accordance with other recent studies generally reporting incidences of 20–30% [5,6,7, 13]. Also as previously demonstrated [5, 7, 14], inferior outcome was observed with a ten-year OS of 86% in the POD24-neg patient group and 66% in the POD24-pos group. We defined POD24-pos as biopsy-proven, thereby excluding clinically-suspected but histologically-unconfirmed events. In addition, we set T0 calculated from treatment initiation in accordance with other studies, while other larger studies have set T0 as time of diagnosis. To facilitate global comparison of findings, reaching a consensus on the definition of POD24 is warranted.
As expected, we found notable differences in the majority of clinicopathological parameters generally considered to be associated with aggressive disease. Among these were performance score, as was also identified previously by Sortais et al., however, in the present study this was based on rather few events. Oppositely, we also identified FLIPI score and its two contributors, age and disease stage, as predictors for POD24 [5]. In agreement with our results, several studies have suggested that patients who experience POD24 have poorer outcomes [8, 13, 15]. This emphasizes the need for close monitoring in patients who experience POD24 to improve their prognosis. Time to treatment initiation of POD24-pos patients was significantly shorter compared with that of POD24-neg patients, probably reflecting the indolent nature of the lymphomas directed to less aggressive treatment management. Furthermore, a significant difference in OS was observed when comparing POD24-pos with POD24-neg patients calculated from a risk-defining event, supporting the suggestion that POD24 is a clinically relevant endpoint when identifying high-risk FL patients.
Considering the clinical heterogeneity of FL, patient outcomes will vary depending on a number of factors including the underlying tumor genetics, and the composition of the tumor microenvironment [3]. Thus, for future risk stratification, it is likely that clinically validated, comprehensive molecular analyses at time of FL diagnosis will be needed in order to determine an individual patient’s probable prognosis and decide upon an appropriate treatment. Future predictive tools must rely on molecular biomarkers as well as clinical and pathological features. However, given the clinical heterogeneity of FL, it is no surprise that molecular analyses of FLs have already shown considerable heterogeneity. Thus it remains to be shown what combination of clinical, pathological and molecular biomarkers will prove most accurate for guiding FL-treatment strategies.
留言 (0)