
記住我

PrimaCare_P3 is a project funded by the European Union (NextGenerationEU, project code n. PNRR-MAD-2022–12376781), and it includes 4 partners: (i) Galliera Hospital (EOG), Genoa, Italy, which is the coordinating center; (ii) the Italian National Institute of Health (Istituto Superiore di Sanità (ISS)), Rome, Italy; (iii) Paolo Giaccone University Hospital (AOUP), Palermo, Italy; (iv) “Aldo Moro” University of Bari (UNIBA), Bari, Italy.
The study is a cluster-randomized controlled trial, with 33 general practitioners (GPs) as clusters. GPs selected by voluntary participation among four GPs cooperatives, i.e., Desenzano del Garda (Brescia), Florence, Naples, and Putignano (Bari), will identify a list of potentially eligible subjects from their electronic records based on an age 65 years and older and the presence of at least one NCD. GPs were randomly allocated to either the intervention group (IG) or the control group (CG). A centrally generated random list of 1216 participants (in 1:1 ratio) will be selected by the Italian National Institute of Health and encouraged by their own GPs to take part of the project. Participants will be required to meet the following inclusion criteria: (1) any gender, (2) age 65 years or older, (3) at least one NCD, (4) willing to participate in the study, and (5) provide signed informed consent. Participants will be excluded based on the following criteria: (1) age lower than 65 years; (2) the absence of at least one NCD; (3) unwilling to participate and provide signed informed consent.
The IG (n = 608) will receive a PPP, and at baseline saliva samples will be collected in this group. The CG (n = 608) will receive usual care. Both groups will be followed up to 12 months after enrolment by research staff including physicians, nurses, and health educators.
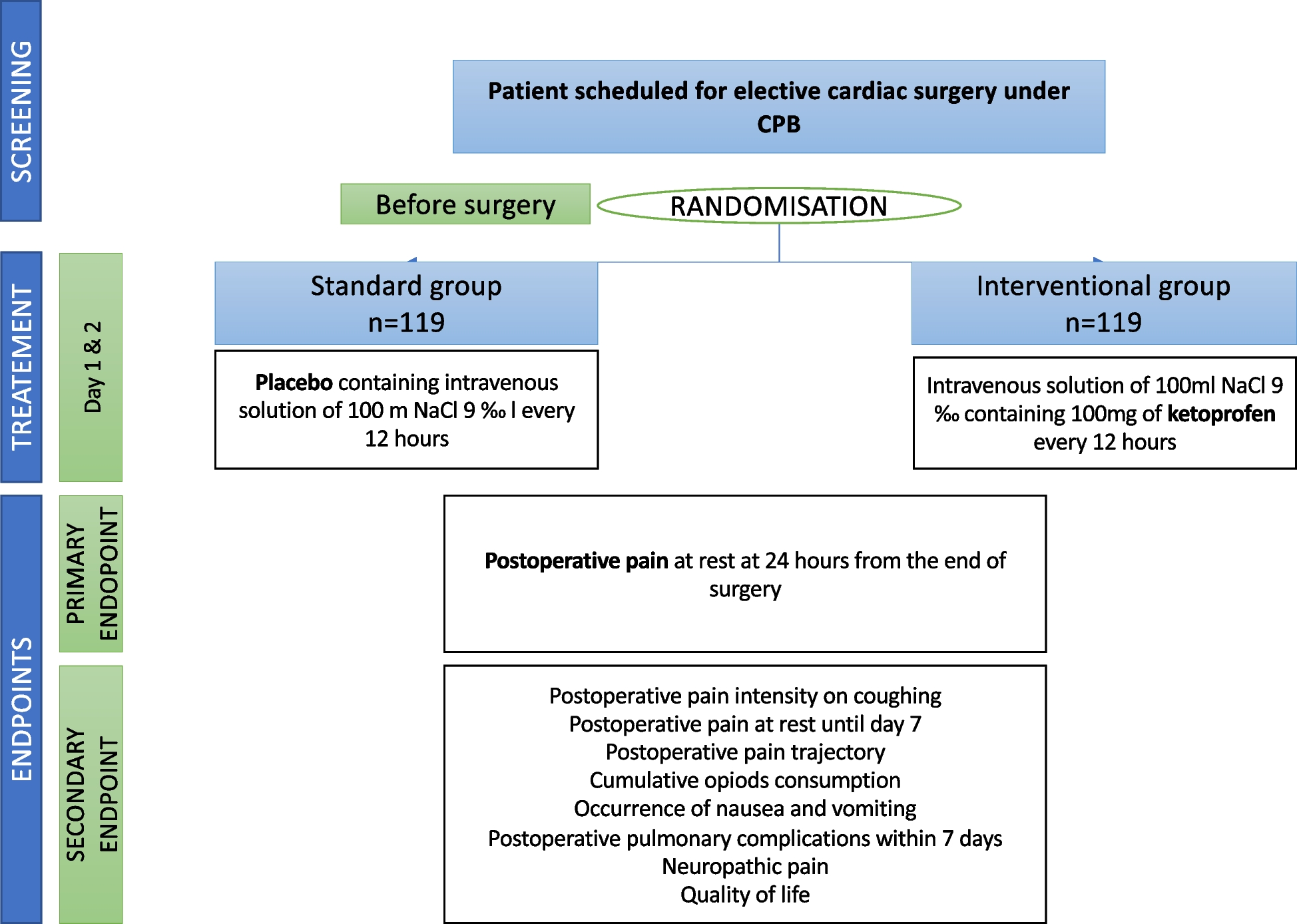
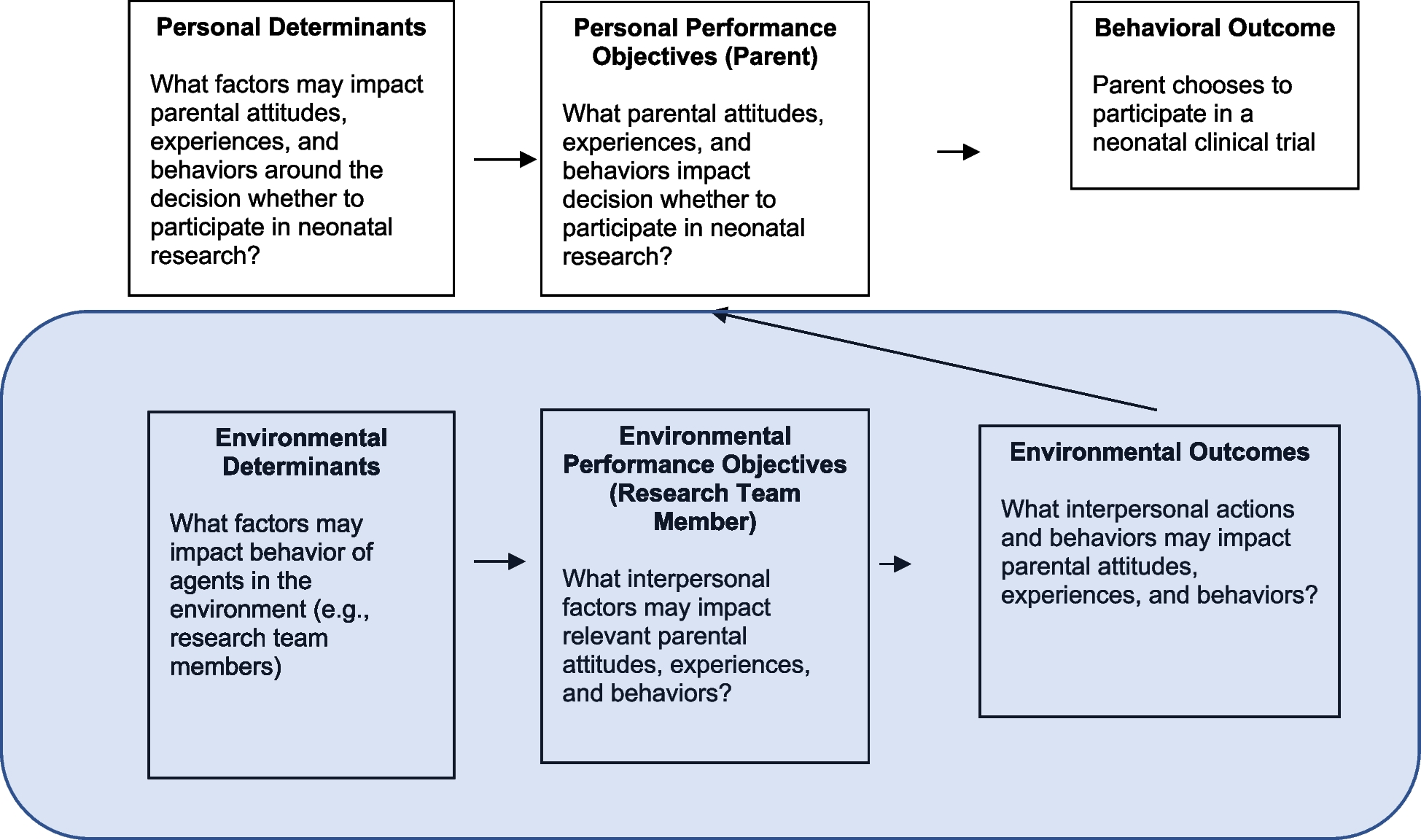
In both IG and CG participants, the rate of unplanned hospitalizations during 1-year of follow-up will be collected (main aim of the study). Moreover, the rates of institutionalizations, the number of admissions to emergency department (ED), number of visits to GP clinics (except those planned by GPs), and death rate will be collected at 6- and 12-month follow-ups (secondary aims of the study). Figures 1(a, b) and 2 show the study design. The process for auditing trial will be conducted by the four principal investigators which belonged to the four involved project’s partners; it will be independent from investigators and the sponsor, and it will last for the entire project period. No data monitoring committee (DMC) is foreseen by the NPRR (National Plan of Recovery and Resilience) call, investment 2.1 Enhancement and strengthening of biomedical research in the National Health System (NHS).
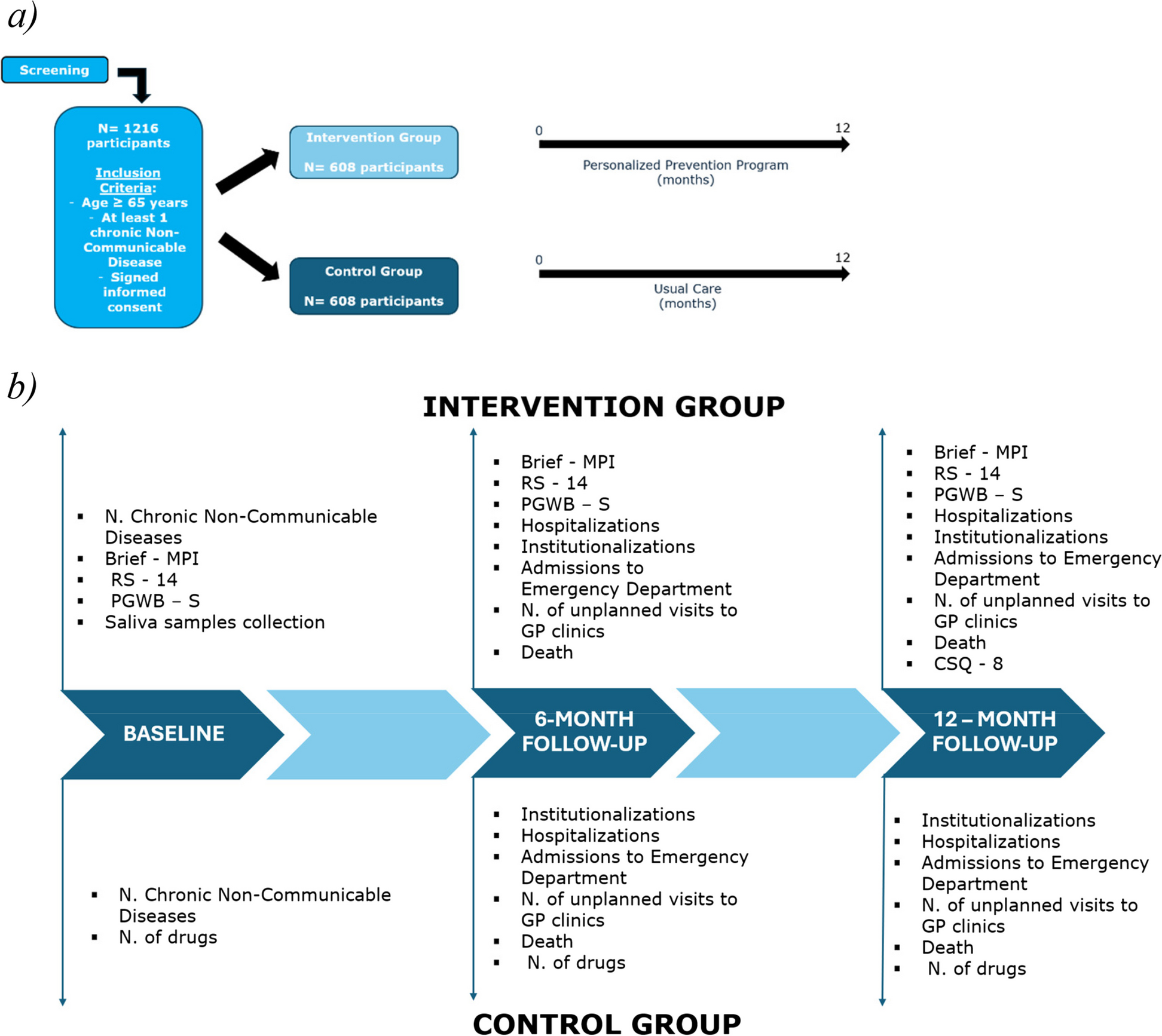
Fig. 1
a Study design and inclusion criteria. b Timeline of the PrimaCare_P3 project related to the Intervention Group and the Control Group. Abbreviations: Brief-MPI, Brief- Multidimensional Prognostic Index; RS-14, Resilience Scale—14 Items; PGWB-S, Psychological General Wellbeing index—Short version; CSQ-8, Client Satisfaction Questionnaire—8 items; GP, General Practitioner
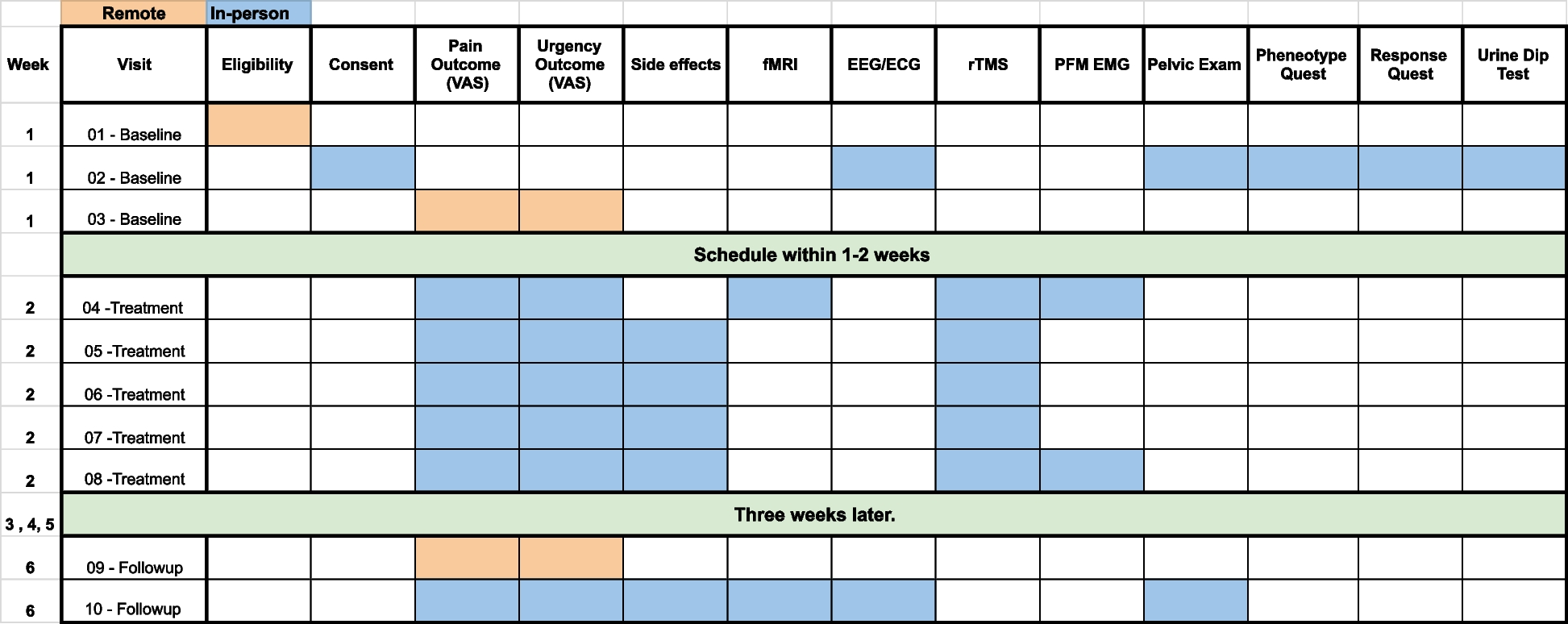
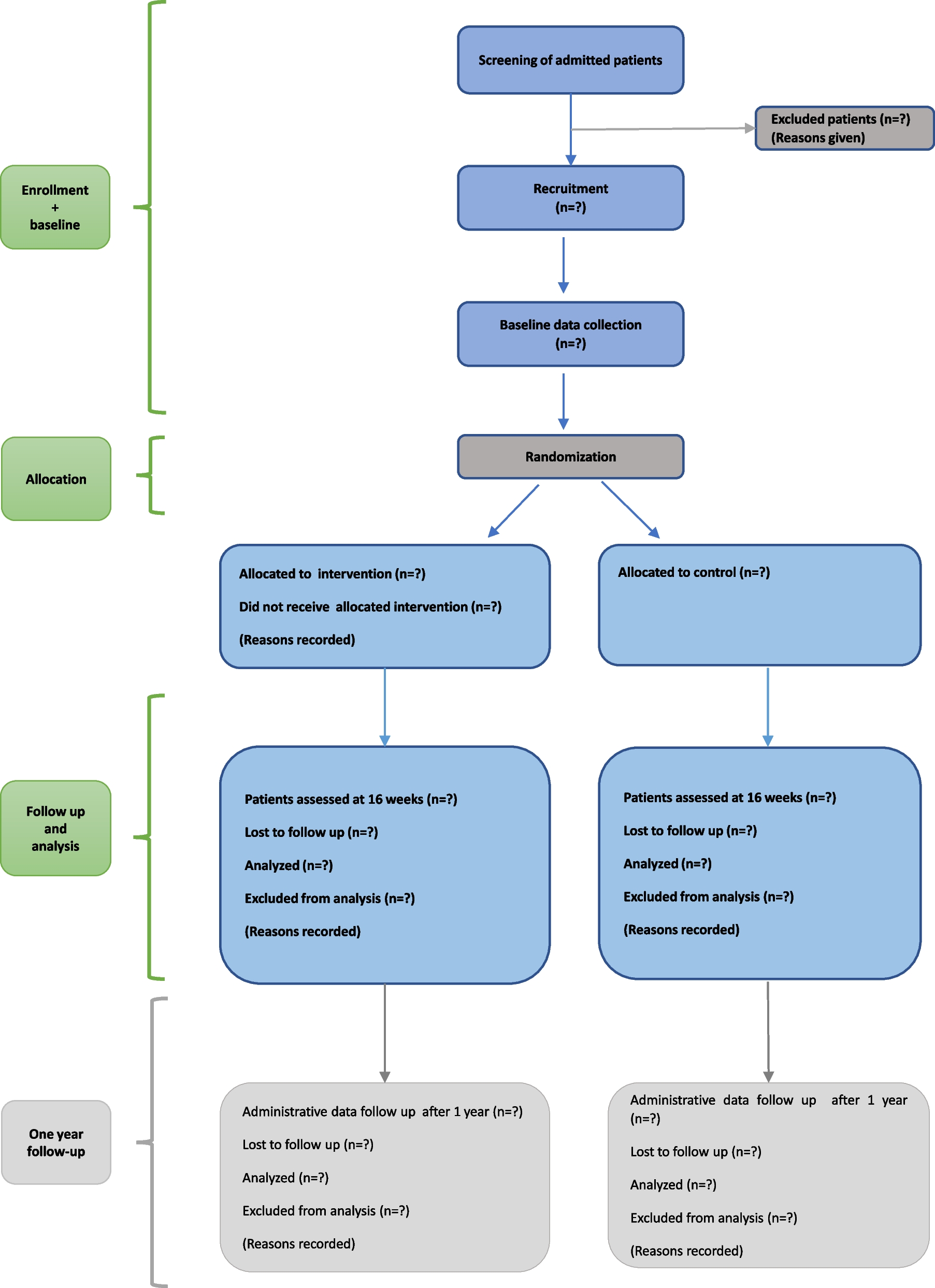
Fig. 2
SPIRIT figure. Schedule of enrolment, interventions, and assessments
Intervention groupClinical evaluationParticipants included in the IG will undergo at baseline and after 6 and 12 months a CGA-based Brief-MPI (Multidimensional Prognostic Index) assessment [13] that is the abbreviated version of the standard version of the MPI (Multidimensional Prognostic Index) [14], a well-known and validated prognostic tool of several negative outcomes, including institutionalization, hospitalization, and mortality. As the MPI standard version, the Brief-MPI explores eight domains: (1) basal, (2) instrumental activities of daily living, (3) mobility, (4) cognition, (5) nutrition, (6) comorbidity, (7) number of medications, and (8) cohabitation status. The Brief-MPI evaluates the level of risk related to each domain (0 = no problems; 0.5 = minor problems; 1 = major problems) and, through a specific algorithm, provides a global score ranging from 0.0 (lowest risk) to 1.0 (highest risk of multidimensional frailty). According to a pre-defined algorithm, the Brief-MPI identifies three classes of risk multidimensional frailty, i.e., MPI 1 class (score between 0.00 and 0.33 = low risk of frailty); MPI 2 class (score between 0.34 and 0.66 = moderate risk of frailty; and MPI 3 class (score ≥ 0.67 = high risk of frailty). Further details on MPI and the Brief MPI calculation and clinical significance have been reported elsewhere (13, 17).
Moreover, at baseline and after 6 and 12 months, the IG participants will undergo the following:
The Resilience Scale—14 items (RS-14) [15], a 14-statement questionnaire based on a 7-point scale assessing the level of resilience. Resilience scores range from 14 to 98, and scores lower than 56 are considered as very low;
The Psychological General Wellbeing Index—Short (PGWB-S) [16], a self-administered 6-item questionnaire for health-related quality of life, including assessment on a scale from 0 to 5 (with 0 as the minimum score) of the following domains: anxiety, vitality, depressive mood, self-control, general health, and positive well-being.
After 6 and 12 months follow-up visit, the IG participants will report the grade of adherence to the PPP, and at the end of the study, they will fill the Client Satisfaction Questionnaire—8 items (CSQ-8) [17], a tool that evaluates the general satisfaction about the intervention through a scale from 1 to 4, with a possible score ranging from 8 to 32, with higher scores indicating higher satisfaction.
Participants who will show a cognitive impairment at the Brief-MPI (see the paragraph 2.2.3 on PPP) will undergo the General Practitioner Assessment of Cognition—Italian (GPCOG-It) test [18], the validated Italian version of GP assessment of cognition. It is a tool used by GPs to screen patients for cognitive decline or dementia. The GPCOG is structured in two sections: one for the patient (“Section A”) which includes a 6-item cognitive test with possible total scores between 0 (indicating severe impairment) and 9 (indicating no impairment) and one for the relative/caregiver (“Section B”) including 6 questions on patient history with possible total scores between 0 (indicating severe impairment) and 6 (indicating no impairment). The GPCOG will be conducted in two stages; if Section A scores between 5 and 8, Section B is not required.
Participants who will show a nutritional deficit at the Brief-MPI (see the paragraph 2.2.3 on PPP) will undergo the Malnutrition Universal Screening Tool (MUST) [19], a screening tool developed and validated by the British Association for Parenteral and Enteral Nutrition (BAPEN) to assess for potential nutritional risks in community-dwelling people. It includes assessment of 3 items: body mass index (BMI), weight loss over time, and acute diseases on a scale from 0 to 2. The total MUST score indicates the overall risk of malnutrition, with 0 indicating a low risk, 1 a moderate risk, and ≥ 2 a high risk.
Laboratory dataSaliva samples will be collected to assess selected biomarkers of oxidative stress and inflammatory status. Specifically, unstimulated whole saliva (UWS) samples will be collected in two plastic sterile tubes. Samples will be stored in the GP clinic at − 20° C until delivery, through dry ice (− 80 °C), to the central laboratories (University of Bari Aldo Moro and ISS) for the analysis. One tube will serve for the analysis of biomarkers of oxidative stress, including (1) lactate (Cell biolabs, MET-5012), (2) NAD/NADH (nicotinamide adenine dinucleotide/nicotinamide adenine dinucleotide hydrogen) ratio (Abcam, ab65348), and (3) products of lipo-peroxidation using ThioBarbituric Acid Reactive Substance analyses (TBARS) Assay Kit (Zeptometrix, 0801192). The second tube will be used for the analysis of levels of salivary inflammatory cytokines, including TNF-α, IL-1β, IL-6, and IL-8 measured by specific Enzyme-Linked ImmunoSorbent Assay Kits—ELISA Kits (Salimetrics, L.L.C).
In a subsample of 210 participants, stratified across the three risk classes of risk (low, moderate, and high risk) of the Brief-MPI scale, the oral microbiome composition will also be analyzed. In this case, the samples will be stored at room temperature and sent to the central laboratory (ISS) by refrigerated transport. Bacterial genomic DNA will be extracted and 16S rRNA gene amplicons amplified using the special fusion primer set specific for V3-V5 hypervariable regions.
Personalized prevention program (PPP)Participants in the IG group will receive a multicomponent PPP based on results of the CGA-based Brief-MPI (see Table 1). PPP is structured as a series of interventions: (i) to improve functional, physical, cognitive, and nutritional status; (ii) to better manage NCDs; (iii) to improve vaccinations adherence; and (iv) to prevent the social isolation.
Table 1 The personalized prevention program interventions based on the CGA impaired domainsFor the physical status, a set of standardized exercises have been made available online to be performed at home by participants.
As for cognitive and nutritional status, decision-making algorithms were created based on the domain score of the Brief-MPI to guide physicians in assigning specific interventions to each participant.
In detail, if at least one question is wrong at the cognition section of the Brief-MPI, the GPCOG-It will be administered [18]. According to its results, four clinical categories of subjects will be identified: (a) participants with a “Section A” score of 9 points will receive a list of suggestions for cognitive health and scheduled to repeat the GPCOG-It after 1 year; (b) participants with a “Section A” score between 5 and 8 and a “Section B” score between 4 and 6 will receive instructions on life-style and a follow-up re-assessment after 6 months; (c) participants with a “Section A” score between 5 and 8 and a “Section B” score ≤ 3 will be recommended to the specialist center, i.e., the Cognitive Disorders and Dementia Centre (CDCD); (d) participants with a “Section A” ≤ 4 will be referred to a specialist center, i.e., CDCD.
For nutritional status, in case of at least one error in the nutrition questions of the Brief-MPI, participants will be stratified according to their BMI. Participants with BMI less than 30 kg/m2, we will perform the MUST [19], and they will be categorized into three risk classes: (a) malnutrition low risk class (MUST score = 0): participants will be reassessed after 12 months; (b) malnutrition medium-risk class (MUST score = 1): participants will be monitored for food intake during the following three days and then they will be reassessed after 3 months or, in case of low food intake, will receive an intervention to improve the overall nutritional intake; (c) malnutrition high-risk class (MUST score ≥ 2): participants will be referred to a specialist in nutrition. On the other hand, participants with BMI score between 30 and 34.9 kg/m2 (class I obesity) will receive dietary suggestions based on the principles of Mediterranean diet, while participants with BMI ≥ 35 kg/m2 (class II obesity) will be referred to a specialist in nutrition.
As regards the management of NCDs, subjects will receive instructions on the prevention rules of the NCDs and instruction on appropriate drugs use according to the STOPP/START criteria (3rd version) for potentially inappropriate prescribing [20]. Similarly, depending on the vaccination profile of each participant, indications will be provided based on the recommendation of the Italian National Plan of Vaccination Prevention (Piano Nazionale Prevenzione Vaccinale (PNPV)) for older adults [21].
For the prevention of the social isolation and loneliness, opportunities for socialization will be suggested through the frequency of community centers and the use of technology (i.e., videocall, and online meetings).
For the functional status, in case of impairment in basic and instrumental autonomy, we will intervene organizing assistance by formal or informal caregivers or activating integrated home care programs or if needed suggesting specialist consults.
Control groupParticipants in the control group will receive standard usual care by their GP. At baseline, data will be collected on chronic diseases (number and category), number of visits to GP clinics (except those planned by GPs), and number of drug prescriptions. At 6- and 12-month follow-ups, data on rates of institutionalization, hospitalization, admission to ED, unplanned visits to GP clinics, on number of drugs, and mortality will be collected.
Training of GPsAll GPs included in the study will be involved in a general training on the project about the following: (i) study objectives, (ii) timeline, (iii) electronic case report form (eCRF), (iv) data entry into the eCRF. GPs assigned to the IG will also receive an additional specific training on study procedures for the following: (1) multidimensional assessment using the Brief-MPI and other clinical scales, (2) administration of the PPP, (3) methods for collecting salivary samples and their storage and delivery to the laboratories for analysis,
Sample sizeA recent Cochrane systematic review [22] reported a significantly lower risk of unplanned hospitalizations in community-dwelling older people treated with CGA compared to standard clinical practice (relative risk (RR) = 0.83; confidence interval (CI) 95%: 0.70–0.99), with a proportion of unplanned hospitalizations at 12 months of 47.7%.
Based on a comparison of proportions between two samples, with a pre-determined number of clusters consisting of 33 general practitioners, assuming an intra-cluster correlation coefficient of 0.004 [23], 28 patients per cluster will be necessary to detect an improvement in the proportion of unplanned hospitalizations at 12 months of approximately 9% in the intervention group, assuming a power of 80% and a type I error of 5%. Taking into account a drop-out rate of 20% over the 1-year of follow-up period, a total of 1216 participants, 608 in IG and 608 in CG, will be enrolled, corresponding to 34 patients per cluster.
Statistical analysis planBaseline characteristics of participants in the IG and the CG will be described and compared. Continuous variables will be compared using Student’s t-test; categorical data will be analyzed using the chi-square test.
We will use generalized estimating equations (GEE) analysis with exchangeable correlation matrix to estimate the association between the primary outcome (secondary outcomes) and the study group; this method takes account of the correlations between observations within the same cluster. The estimates will be adjusted for baseline characteristics that significantly correlated with the primary outcome (secondary outcomes) by including these variables as covariates in the model. Moreover, we will use both intention-to-treat (IIT) and per-protocol (PP) analyses to avoid potential biases related to missing data.
The incidence rate ratios of hospitalization, institutionalization, admissions to ED, and mortality will be estimated using Poisson regression random effects model.
The scores of clinical scales (Brief-MPI, RS-14, PGWB-S) will be compared between baseline and follow-up using Student’s t-test for paired samples. The linear mixed-model analyses will be used to assess if the baseline characteristics and biomarkers will be associated with different trajectories of clinical scales, accounting for the clustering of participants.
留言 (0)