
記住我








The control group will receive “usual care” at the MipAC unit. This encompasses a broad spectrum of assessments and medical interventions, each tailored to the individual patient’s specific needs. While attending physicians may seek to optimize the general medication regimen also for some patients in the control group, the nature of any medication review in this arm will vary, reflecting the diverse clinical practices among different physicians at the MipAC unit. Such reviews will not include the structured approach characteristic of the intervention arm, which involves systematic discussions with geriatricians and GPs to improve medication management. This choice of comparator aligns with the study’s primary objective of evaluating the effect of the intervention. Usual care at the MipAC unit offers the most direct comparison and is ethically acceptable.
Intervention descriptionThe intervention consists of three main parts: (1) clinical assessment of the participant and medication review by a MipAC intervention physician, (2) supervision by geriatrician, and (3) a telephone meeting between the MipAC physician and the participant’s GP.
(1)Clinical assessment and medication review
We aim to recruit 1–4 MipAC intervention physicians who are specialized in General Practice to take part in the study, and patients randomized to the intervention group will be assigned to one of them as their attending physician. In addition to providing usual care, these intervention physicians will conduct structured clinical medication reviews aimed at optimizing the patients’ total medication use.
The framework for conducting the medication reviews draws upon previous experiences from the previous COOP study, incorporating recommendations from the Norwegian Directorate of Health’s guidelines on medication reviews and polypharmacy [22], as well as the Scottish NHS’s polypharmacy guidance [23]. The cornerstone of the medication reviews is a personalized approach, tailored to each patient’s unique combination of health conditions, symptomatology, medication use, and individual preferences.
The MipAC intervention physician will obtain information regarding the patient’s medical history and medication use, ensure the availability of necessary supplementary diagnostics (e.g., blood analyses, electrocardiograms, and blood pressure measurements), and conduct a physical examination. All medications in use will be approached systematically to ensure medication appropriateness, optimize disease control, ensure correct dosing, and reduce the risk of adverse effects and drug interactions. Tools such as drug interaction databases will be employed routinely to support this process [24]. Furthermore, explicit tools like lists of anticholinergic drugs [25, 26], STOPPFrail [27, 28], and STOPPFall [29] may be consulted; however, these tools are supplementary rather than integral to the medication review process.
(2)Geriatric supervision
For clinical supervision, the MipAC intervention physician will consult a geriatrician (RR; TBW) to review patient findings and proposed medication adjustments. They will discuss the optimal timeline for these adjustments and evaluate any needs for new medications. This consultation will take place prior to the meeting with the patient’s GP.
(3)Telephone meeting between the MipAC intervention physician and the FP
After conducting the clinical medication review, the MipAC intervention physician will arrange a telephone meeting with the patient’s GP to discuss the findings. This collaborative medication review aims to optimize the patient’s medication plan, considering both the geriatric insights and the GP’s knowledge of the patient’s history. The two physicians will discuss potential adjustments as well as the patient’s need for further follow-up, and collaboratively develop a step-by-step plan for adjusting medications. This interaction can alternatively be conducted via digital communication platforms according to the GP’s preferences. If for any reasons direct contact is not established, the GP will receive a written summary of the clinical medication review (steps 1 and 2).
Criteria for discontinuing or modifying allocated interventionsAllocated interventions will neither be discontinued nor modified. Usual care does not inherently entail risks and may sometimes include components of the intervention. The intervention will be administered by designated MipAC intervention physicians who are also familiar with routines at the MipAC unit, ensuring that usual care is consistently provided. Inability to establish contact with the GP will not be considered a reason for modifying or discontinuing the allocated interventions since the medication review will still be conducted in collaboration with the geriatrician, and the GP will be informed through written documentation.
Strategies to improve adherence to interventionsPatients in the intervention group receive a structured discharge conversation focused on medication management. Any modifications to their medication regimen are recorded in the medication system, home care services (if relevant) are informed, and a review summary is sent to their GP. For participants with multiple medication adjustments or other clinical indications, a follow-up appointment with their GP will be recommended.
Relevant concomitant care permitted or prohibited during the trialParticipants will resume their usual care after discharge. There will be no recommendations regarding concomitant care. The GP remains responsible for post-discharge care decisions and will assess participant needs independently of the study.
Provisions for post-trial careCompensation for individuals who may suffer harm related to the MipAC unit admission will be covered by the Norwegian Patient Injury Act independently of participation in the study.
Outcomes Primary outcomeThe primary outcome measure is HRQoL, measured by the 15D instrument at 16 weeks, adjusted for baseline score [30]. The 15D instrument is a validated patient-reported outcome measure that has been used in similar geriatric interventions [31, 32], including the previous COOP study [12]. It encompasses 15 dimensions including mobility, vision, hearing, breathing, sleeping, eating, speech, elimination, usual activities, mental function, discomfort and symptoms, depression, distress, vitality, and sexual activity [33]. Each dimension is rated on a five-level ordinal scale, with the respondents choosing the level that best describes their present health status. The 15D instrument offers both a profile measure and a single index representing overall HRQoL. For the purpose of this study, the single index version will be utilized. Scores are calculated by population-based utility weights and range from 0 (poorest HRQoL) to 1 (excellent HRQoL) [30, 33]. A change of ± 0.015 or more is considered the minimum important change (MIC), and a change of more than 0.035 in the positive direction represents “much better HRQoL” [34]. Since acute illness can impact HRQoL, patients are asked at baseline to provide responses reflecting their typical condition prior to the acute episode that led to admission.
Secondary outcomesSecondary outcomes are assessed 16 weeks after baseline and include physical and cognitive function, oral health, falls, admissions to healthcare facilities, and mortality. Details on these outcomes are listed in Table 1.
Table 1 Detailed description of secondary outcomesOther pre-specified outcomesWe will calculate the carbon footprint of the intervention and usual care by conducting a life cycle assessment based on ISO standards [40]. We will include data such as types and quantities of medications administered, types and quantities of medical equipment used during the MipAC unit stay, number and length of admissions to healthcare facilities, and number of outpatient and GP consultations in the period from discharge until 16 weeks. These data will be converted to carbon dioxide equivalents.
The primary study period will end after 16 weeks. However, we will also evaluate long-term outcomes in terms of mortality rates and admissions to healthcare facilities up to 1 year.
Descriptive variablesDemographics and diagnoses according to ICD-10.
Charlson Comorbidity Index (CCI) [41].
Clinical Frailty Scale (CFS) [42].
Oral health: Number of teeth, tooth mobility, number of patient-referred implants, the Revised Oral Assessment Guide [43], and the Mucosal-Plaque Score [44].
Medication details: Information on medications utilized at baseline and after 16 weeks, medication discrepancies, changes to medications initiated during admittance and post-discharge, and recommendations on medication adjustments outlined in the discharge letter. Medications will be registered according to the Anatomical Therapeutic Chemical classification system [45].
Nutritional status: Measurement of mid-upper arm circumference [46].
Details on the MipAC unit stay: Number of attending physicians, length of stay, reasons for admittance, discharge diagnoses, severity of acute illness as assessed by National Early Warning Score 2 (NEWS2) scores [47, 48], and types and quantities of medical equipment used.
Post-discharge healthcare service utilization: This will encompass the frequency of consultations with FPs, the number of outpatient visits, and admissions to various healthcare facilities including hospitals, MipAC units, nursing homes, and rehabilitation institutions.
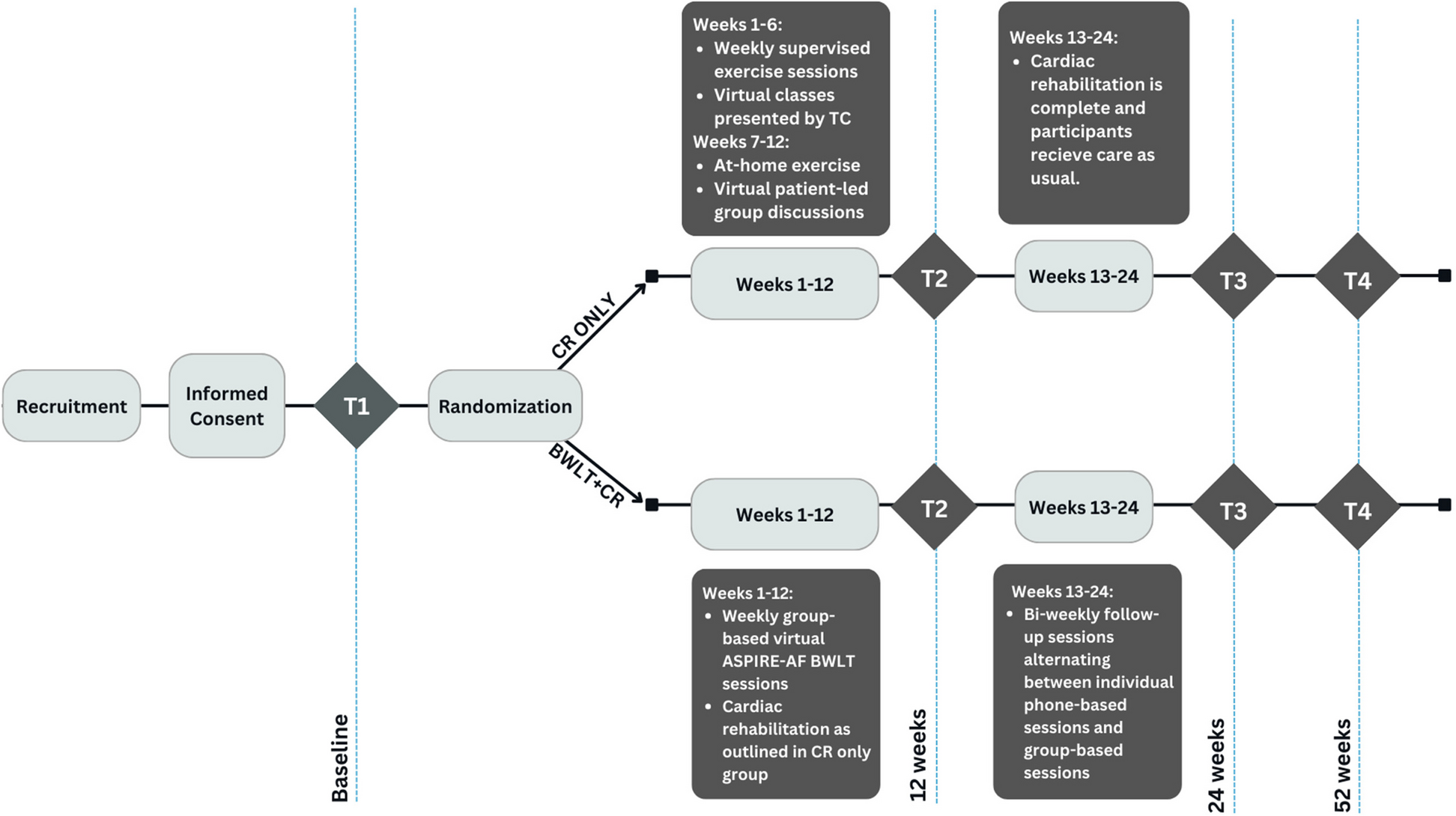
Participant timelineThe participant timeline is illustrated in Fig. 2.
Fig. 2
Schedule of enrolment, interventions and assessments
Sample sizeBased on the results of the previous COOP study, we hypothesize a mean difference between groups of 0.04 on 15D, and the standard deviation of the change in 15D from baseline to 16 weeks is assumed to be 0.13 [12]. With inclusion of a total of 350 patients (whereof 175 in the intervention group), the power to detect a difference of 0.04 on 15D will be at least 80% with a significance level of 5% [11].
RecruitmentThe recruitment team combines the clinical expertise of health personnel familiar with the MipAC setting with the research experience of those skilled in clinical trial recruitment. This ensures efficient and effective participant enrolment.
留言 (0)