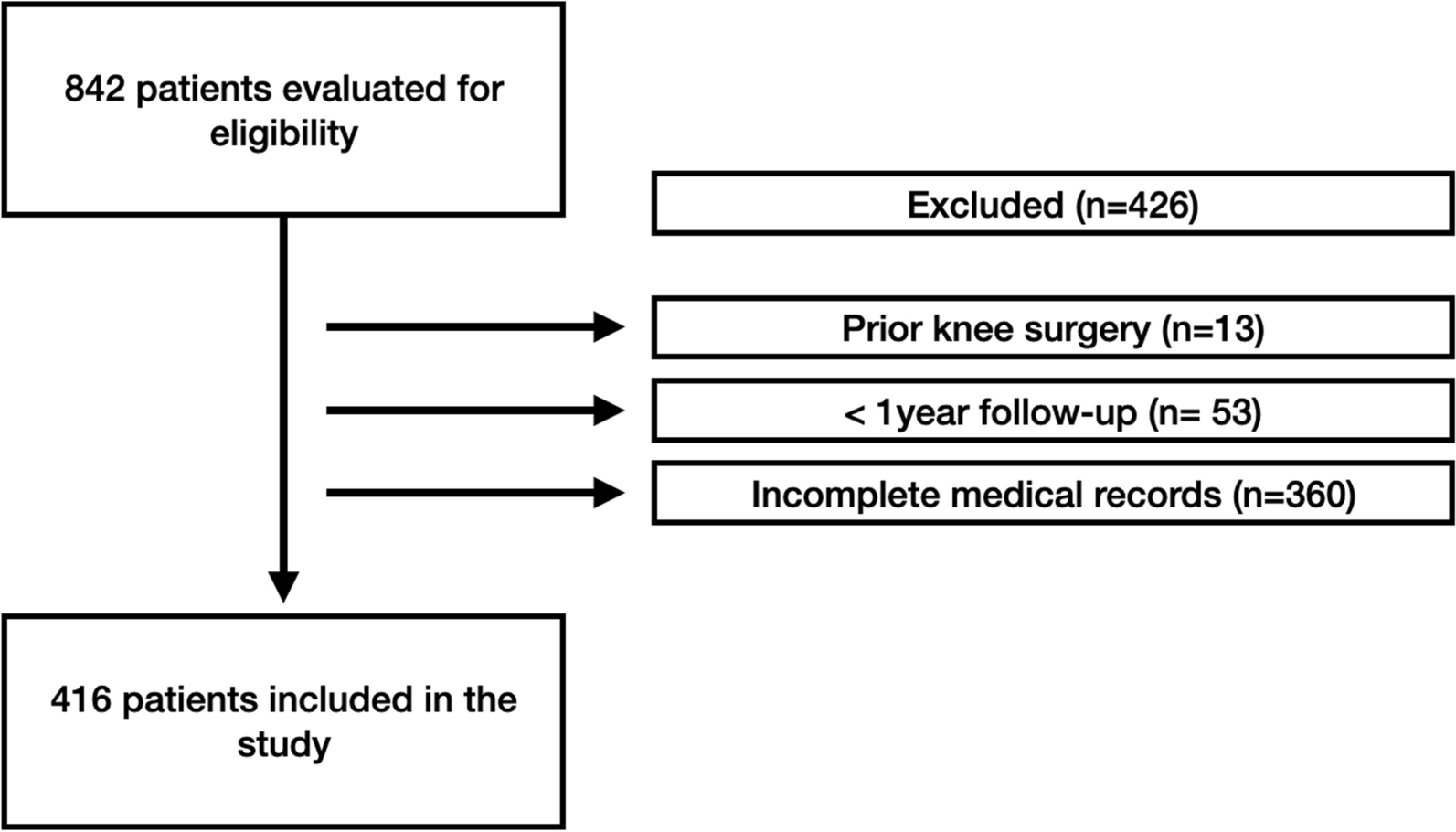
This is a case–control study of One hundred and one consecutive adolescents (aged 18 years or younger at the time of surgery) who underwent surgery for major thoracolumbar/lumbar idiopathic scoliosis (Lenke 5C and 6C) with posterior approach at our hospital and were prospectively followed for four years or more.
The inclusion criteria were: 1. AIS Lenke 5C and 6C. 2. LIV and L3 and L4. 3. The lower end vertebra (LEV) was at L4 in all patients. 4. DVR and non-DVR techniques. Exclusion criteria were as follows: (1) Patients above 18-year-old. (2) Patients with anterior or other types of approach. (3) Patients with revision surgery.
Thirty patients had AIS Lenke 6C, and seventy-one had AIS Lenke 5C. The initial 52 patients without DVR comprised the control group (N-DVR), while the subsequent 49 consecutive patients using DVR formed the DVR group, all under the same surgeon’s directive between 2010 and 2017.
Patients were categorised into two groups based on the lowest instrumented vertebra (LIV) level. In Group DVR, the lowest instrumented vertebra (LIV) was defined as the Lower End Vertebra-1 (LEV-1), while in Group N-DVR, the lowest instrumented vertebrae (LIV) were considered to be the lowest end vertebrae (LEV). To minimise selection bias, all patients in both groups had their lowest end vertebra at the fourth lumbar vertebra.
The institutional review board approved this study, and consent was obtained from patients before this study was conducted.
Study design
In this study, patients were divided into two groups based on the surgical technique employed for the correction of AIS Lenke 5C and 6C curves. The design was structured so that the non-DVR group (n = 52) was treated first, establishing a baseline for comparative prospective data collection, followed by the DVR group (n = 49).
Clinical medical records, radiography films of the spine, and health-related quality of life assessments of the patients (SRS-22) were prospectively recorded, and none of the patients were lost during the minimum 4-year follow-up. Two experienced spine surgeons performed follow-up examinations before surgery, the day of patient discharge from the hospital, 6 months, and four years after surgery. Standing posteroanterior, side bending films and sagittal radiography films of the whole spine were obtained preoperatively and 6 and 48 months postoperatively. Furthermore, two experienced spine surgeons measured all radiography films using the Surgimap software application.
Surgical techniques
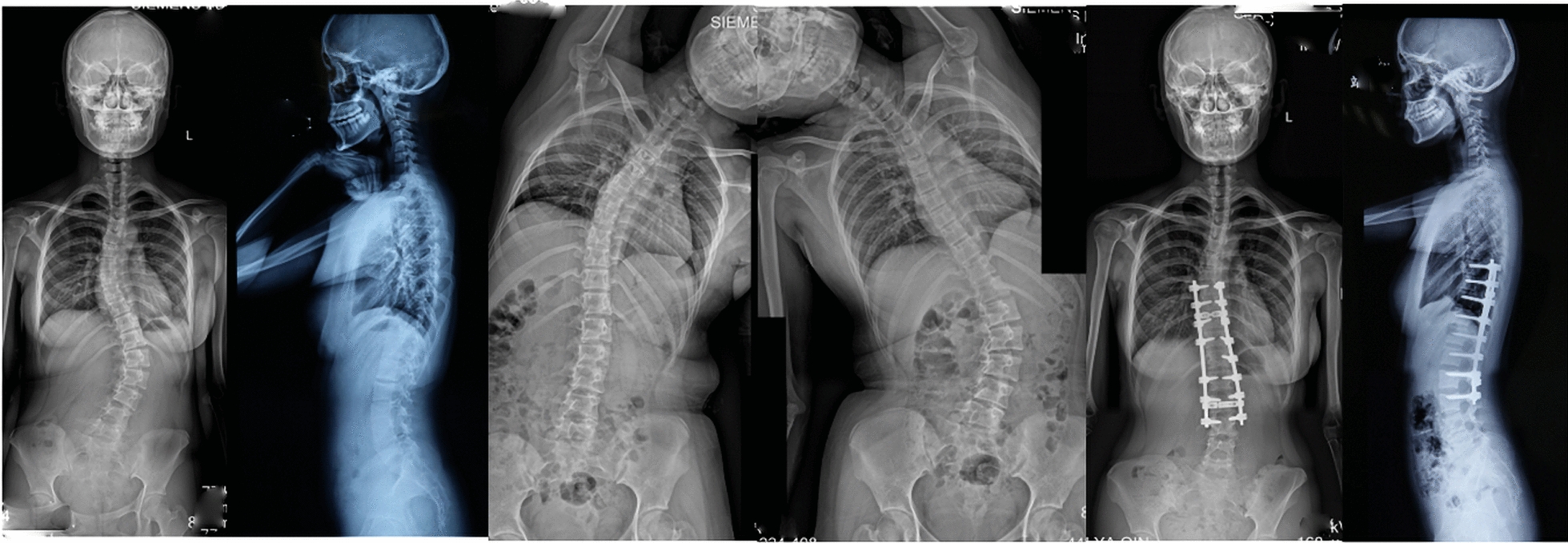
The patients underwent surgery in the prone position, during which the posterior elements of the spine were carefully exposed using electrocautery. Those with DVR underwent the Ponte procedure. Pedicle screws were inserted using the freehand technique based on posterior bony elements. All patients were fitted with 5.5 mm. The concave rod was slightly over-contoured into kyphosis to accommodate possible rod flattening during rod rotation. Rod insertion began from the top to the bottom in both groups. The correction of spinal deformity in the N-DVR group was achieved by concave rod derotation. Final correction in both groups involved using coronal in situ bending, with the handles of the coronal in situ benders held as low as possible to produce both scoliosis and hypokyphosis correction. The convex rod was inserted in situ without compressing the main thoracic curve to prevent flattening of the thoracic kyphosis. Compression of screw heads was performed as necessary in cases of structural upper thoracic and/or thoracolumbar/lumbar curves (concave rod). The DVR procedure in the DVR group involved using the SmartLink device (Medtronic). The SmartLink instrument was inserted into three axial pedicle screw pairs in the main lumbar curve, typically bilaterally into L3, L2, and L1 vertebral bodies. The device was used to derotate the lumbar spine by lifting up the low-lying apical major lumbar concave area, providing both DVR and hyperlordosis correction. Spinal fusion was performed using the patient’s bone material from facetectomies, osteotomies, tricalcium phosphate, and hydroxyapatite graft extenders.
Spinal cord monitoring during surgery with the use of somatosensory evoked potentials (SSEPs), motor evoked potentials (MEPs), and electromyography (EMG) involves various neurophysiological techniques to assess the functional integrity of susceptible neural elements, including the spinal cord and nerve roots.
Clinical and radiological data evaluation
A thorough physical examination was performed on the patients prior to surgery, at the time of discharge, and during follow-up appointments. This comprised a neurological examination of the lower limbs and a coronal and sagittal balance assessment.
Before and after the procedure, the patient’s spinal alignment and curvature were assessed using upright posteroanterior (PA) and lateral radiographs. Preoperative supine side-bending (SB) coronal concave and convex radiographs were also analysed. The measurements included coronal balance, sagittal balance, thoracic kyphosis (TK), lumbar lordosis (LL), L3 translation on PA film and concave SB film, L3 rotation and L4 tilt on convex SB film, L3/4 disc opening or closing on convex SB film, curve flexibility, Distal junctional angle (DJA), L3-S1 Lumbar Lordosis, Radiography shoulder height (RSH), Pelvic Obliquity, Adding-on phenomenon, Proximal Junctional angle (PJA) and apical vertebral translation (AVT) of the thoracic and lumbar curves.
The distance between the central sacral vertical line (CSVL) and the midpoint of the apical vertebral body defines apical vertebral translation (AVT). L3 translation is measured by the distance between the CSVL and the midpoint of the L3 vertebra on PA film and concave SB film. L3 rotation is defined by Moe–Nash’s method [12, 13]. Thoracic kyphosis (TK) is measured by the angle between the upper endplate of T1 and the lower endplate of T12, while the upper endplate of L1 and S1 measures lumbar lordosis (LL). Coronal balance is determined by the coronal C7 plumb line (C7PL) deviation from the CSVL, with a value > 20mm defined as an imbalance. Sagittal balance is measured by the deviation of the sagittal C7PL from the posterior edge of the sacrum, with a value > 50mm defined as imbalance. Flexibility is calculated using the formula: (preoperative Cobb angle − preoperative SB Cobb angle)/preoperative Cobb angle × 100 (%), and curve correction is calculated as follows: (preoperative Cobb angle − post-operative Cobb angle)/preoperative Cobb angle × 100 (%). The coronal balance and sagittal balance are averaged using absolute values. Furthermore, LIV tilt (the angle between the inferior endplate of LIV in a horizontal plane), LIV translation is the horizontal offset from the centre of LIV to the CSVL (L3-CSVL and L4-CSVL), and LIV disc angle is assessed as the disc angle immediately adjacent to LIV. Distal junctional angle (DJA) was defined as the angle between the LIV's upper end-plate and the vertebra's lower endplate below. DJA ≥ 10° was defined as distal junctional kyphosis (DJK). L3-S1 Lumbar Lordosis (refers to the angle of curvature in the lumbar spine measured between the superior endplate of the L3 vertebra and the superior end plate of the S1 vertebra.
We evaluated adding-on (AO) and proximal junctional kyphosis (PJK). PJK was assessed using the proximal junctional angle (PJA) from the lateral whole spine upright radiographs taken before surgery and during follow-up. PJK is defined as an increase of at least 100 in the proximal junction sagittal Cobb angle, with the postoperative angle being 100 greater than the preoperative measurement. This is taken between the upper endplate of the upper instrumented vertebra (UIV) plus two and the lower endplate of the UIV. Adding-on is characterised by an increase in the number of vertebrae involved in the distal curve, measured from the upright radiograph to the most recent one. This condition is identified by two criteria: (1) an increase of more than 5mm in the deviation of the first vertebra from the central sacral vertical line (CSVL) below the instrumentation, and (2) an increase of more than 5 degrees in the angulation of the first disc below the instrumentation level.
Furthermore, we assessed the radiographic shoulder height (RSH) evaluates shoulder balance and is defined as the difference in the soft tissue shadow observed on a standing anteroposterior radiograph located directly above the acromioclavicular joint.
All measurements were performed using Surgimap software, and the last vertebra touching the CSVL (last touching vertebra, LTV) was determined for each patient.
SRS-22 evaluation of quality of life
All patients had to complete the Scoliosis Research Society questionnaires (SRS-22) before surgery and during follow-up visits. These questionnaires measure clinical outcomes in five domains: function/activity, pain, self-perceived image, satisfaction with treatment, and mental health.
Statistics analyses
The values are ranges, means, and standard deviations (SD). The degree of significance for continuous variables (unpaired for between and paired for within-group comparison) was determined using a 2-tailed independent t-test. The χ2 test was applied to categorical variables. P values were deemed statistically significant if they were less than 0.05.


留言 (0)