
記住我
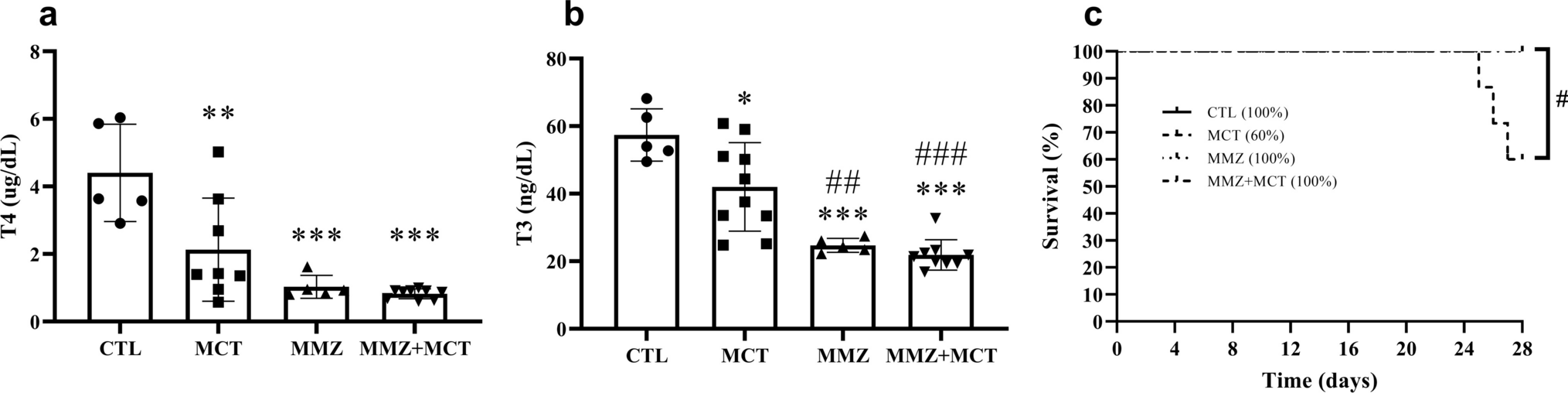
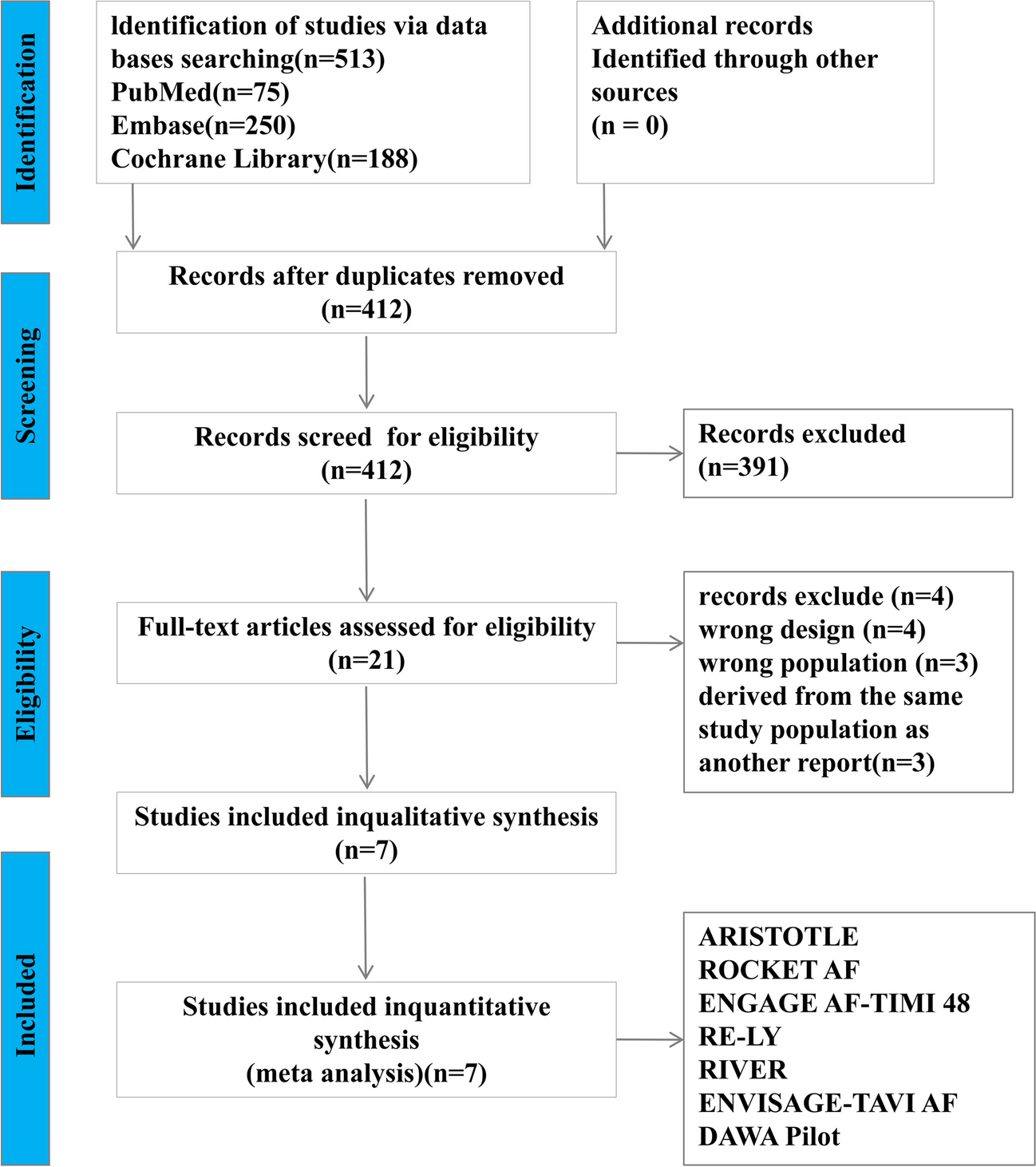
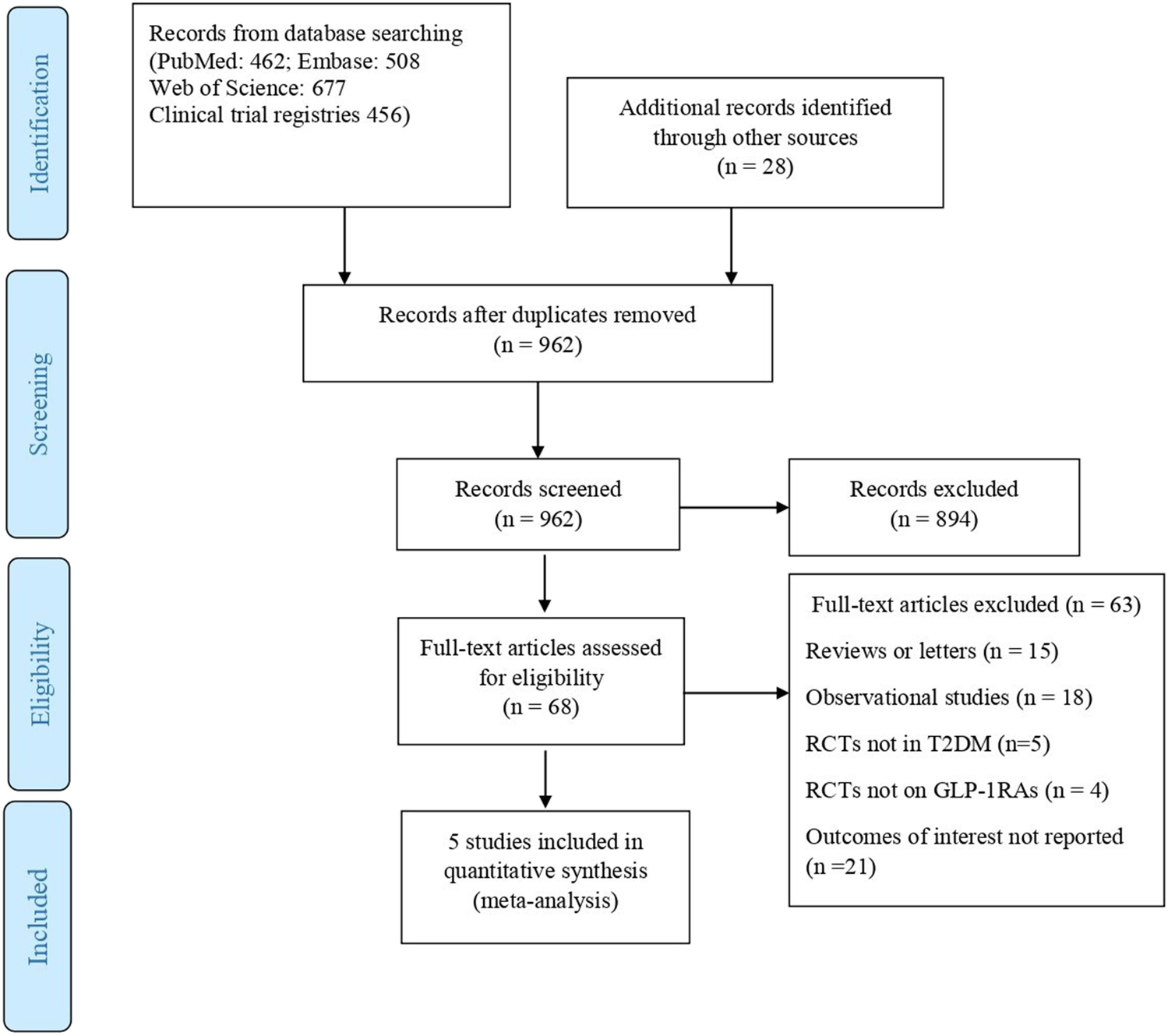
The literature retrieval and screening processes are shown in Fig. 1. Using this search strategy, 513 articles from the PubMed, LILACS, and MEDLINE databases were identified and recorded. After reading their titles and authors, 101 duplicate articles were excluded; further careful review of the abstract excluded 391 articles that included reviews, systematic reviews, and conference articles and did not conform to the inclusion criteria regarding study content, intervention measures, and control measures. After careful reading of the full text to review the study design and outcomes, studies were excluded, and 14 studies were subsequently removed because their original text could not be retrieved. Finally, seven studies were included in this meta-analysis [17,18,19,20,21,22,23]. Figure 1 illustrates the flowchart of the study selection and inclusion as a flowchart. A total of 16,070 patients (9176 in the new oral anticoagulant group and 6894 in the warfarin group) were included.
Fig. 1
Flow diagram for the study search process
Study CharacteristicsAmong the studies included in the analysis, four were retrospective post-hoc subgroup analyses of RCTs, and three were double-blind experimental RCTs, with a subset of three studies focusing exclusively on patients with a bioprosthetic heart valve (BHV), either aortic or mitral. As depicted in Table 1, the trials encompassed a range of VHD types. The predominant form of type 2 VHD was native valvular heart disease, with over 2800 individuals having received bioprosthetic valve replacements or valve repair. The NOACs included in the studies were dabigatran, rivaroxaban, edoxaban, and apixaban. The first three drugs were compared in patients with various types of type 2 VHD, and the last drug was used for only native type 2 VHD cases.
Table 1 The different types of type 2 VHD in the included studiesPatient CharacteristicsTable 2 details the principal clinical features and risk factors associated with bleeding and thromboembolic events among patients with AF and VHD treated with NOACs. The lowest and highest mean (± standard deviation) ages were 48.8 ± 10.4 and 82.1 ± 5.4 years, respectively. The results showed that patients with type 2 VHD often had heart failure, coronary artery disease, diabetes, history of stroke, systemic embolism, transient ischemic attack, and hypertension. Most types of atrial fibrillation were persistent. Approximately 60% of patients were taking warfarin at baseline but were randomized to either group. The mean or median percentage of time with an INR in the therapeutic range in the VKA group is > 60%.
Table 2 The baseline characteristics in the included studiesOutcome AssessmentEfficacy Outcomes: Stroke and Systemic EmbolismNOACs proved to be more efficacious than VKAs in patients with AF and type 2 VHD, exhibiting a reduced RR for stroke/SE (RR, 0.75; 95% CI, 0.64–0.89; P = 0.0006). The evidence from the studies was of high quality, with no heterogeneity (I2 = 0%; P = 0.68).
Safety Outcome: Major Bleeding and Intracranial HemorrhageThere was no significant decrease in major bleeding events among patients with type 2 VHD treated with NOACs compared with those on VKAs (RR, 0.88; 95% CI, 0.64–1.21; P = 0.43). The evidence quality for this finding was low, with a high degree of heterogeneity across the studies (I2 = 85%; P < 0.0001).
Compared with VKAs, NOACs reduced the risk of ICH in patients with type 2 VHD (RR, 0.46; 95% CI, 0.27–0.77; P = 0.003). The evidence quality for this finding was low, with a high moderate heterogeneity across the studies (I2 = 60%; P = 0.03).
The forest plot for stroke/SE, major bleeding, and intracranial hemorrhage in patients with atrial fibrillation and type 2 valvular heart disease on anticoagulation is shown in Fig. 2, and the funnel plot is respectively shown in Fig. S1-3 (Appendix 2 in the supplementary information).
Fig. 2
The forest plot illustrates the individual and pooled estimates of the risks associated with stroke/systemic embolism, major bleeding, and intracranial hemorrhage in patients with atrial fibrillation and type 2 valvular heart disease on anticoagulation. CI confidence interval, M–H Mantel–Haenszel, NOACs new oral anticoagulants, VKAs vitamin K antagonists; the asterisks indicate that the DAWA pilot study conducted by Rodrigues Duraes et al. (2016) only reported bleeding in the warfarin and dabigatran groups, and no reports of major bleeding and intracranial hemorrhage in the warfarin and dabigatran groups were reported, so they were not included in this analysis
Significant heterogeneity was observed in the safety analysis comparing NOACs to VKA in patients with type 2 VHD and AF, leading to the use of a random effects model to pool effect sizes. Given the potential differences in outcomes between bioprosthetic and native valves, a secondary analysis was performed for patients with bioprosthetic valves and AF.
Bioprosthetic Heart Valves and Secondary AnalysesFor patients with bioprosthetic heart valves (BHV), five studies furnished comprehensive data: a subset from the ARISTOTLE trial [22, 24] involving BHV replacement or native valve repair (87 in the apixaban group vs. 69 in the VKAs group), a designated subgroup from the ENGAGE AF-TIMI trial [25] with 191 patients with BHV (121 in the edoxaban group vs. 70 in the VKAs group), a DAWA trial [21] pilot study including post-operative AF patients with bioprosthesis (15 in the dabigatran 110 mg twice daily group vs. 12 in the VKAs group), 1426 patients with AF from the ENVISAGE-TAVI AF trial [17] post transcatheter aortic valve replacement (713 in the edoxaban group vs. 713 in the VKAs group), and the RIVER trial’s [18] 1003 participants with bioprosthetic mitral valves (500 in the rivaroxaban group vs. 503 in the VKAs group). Aggregated data revealed that compared with VKAs, NOACs were more effective in reducing stroke and systemic embolism risks (RR, 0.65; 95% CI, 0.44–0.96), with no significant difference in major bleeding (RR, 0.76; 95% CI, 0.38–1.54) and ICH risks (RR, 0.61; 95% CI, 0.34–1.09) between NOACs and VKAs. The findings from the secondary analyses were consistent with the primary outcomes.
The sensitivity analysis of this group showed that the ENVISAGE-TAVI had a greater effect on heterogeneity. Compared with VKAs, NOACs reduced the risk of major bleeding in patients with bioprosthesis after this trial was excluded (RR, 0.53; 95% CI, 0.30–0.94; P = 0.03). The evidence quality for this finding was no heterogeneity (I2 = 0%; P = 0.64).
The forest plots for stroke/SE, major bleeding, ICH, and sensitivity analysis excluding the ENVISAGE-TAVI AF trial of major bleeding in patients with AF and BHV on anticoagulation are shown in Figs. 3 to 4 and the funnel plots are shown in Fig. S4–S7 (Appendix 2 in the Supplementary Information).
Fig. 3
The forest plot illustrates the individual and pooled estimates of the risks associated with stroke/systemic embolism, major bleeding, and intracranial hemorrhage in patients with atrial fibrillation and bioprosthetic heart valves on anticoagulation. CI confidence interval, M–H Mantel–Haenszel, NOACs new oral anticoagulants, VKAs vitamin K antagonists
Fig. 4
The forest plot illustrates the sensitivity analysis excluding the ENVISAGE-TAVI AF trial of the risks associated with major bleeding in patients with atrial fibrillation and bioprosthetic heart valves on anticoagulation. CI confidence interval, M–H Mantel–Haenszel, NOACs new oral anticoagulants, VKAs vitamin K antagonists
Risk of Bias in Individual StudiesIn terms of bias assessment for the included studies in this meta-analysis, the Cochrane collaboration tool was employed. All seven studies utilized randomization and transparently reported the random sequence generation and allocation concealment. One study had a relatively high risk of bias and was of low quality. This was a prospective phase II pilot study with no blinding to outcome evaluation and with selective reporting. The remaining six studies were high quality, exhibiting low bias risk, complete outcome data, absence of selective reporting, and minimal biases related to follow-up and publication. The increased risk of bias was mainly due to the open-label design of three trials, and four trials conducted post-hoc analysis, which mainly explains the increase in “other bias.” The overall risk of bias was deemed mild to moderate (Appendix 3 in the supplementary information).
留言 (0)