
記住我

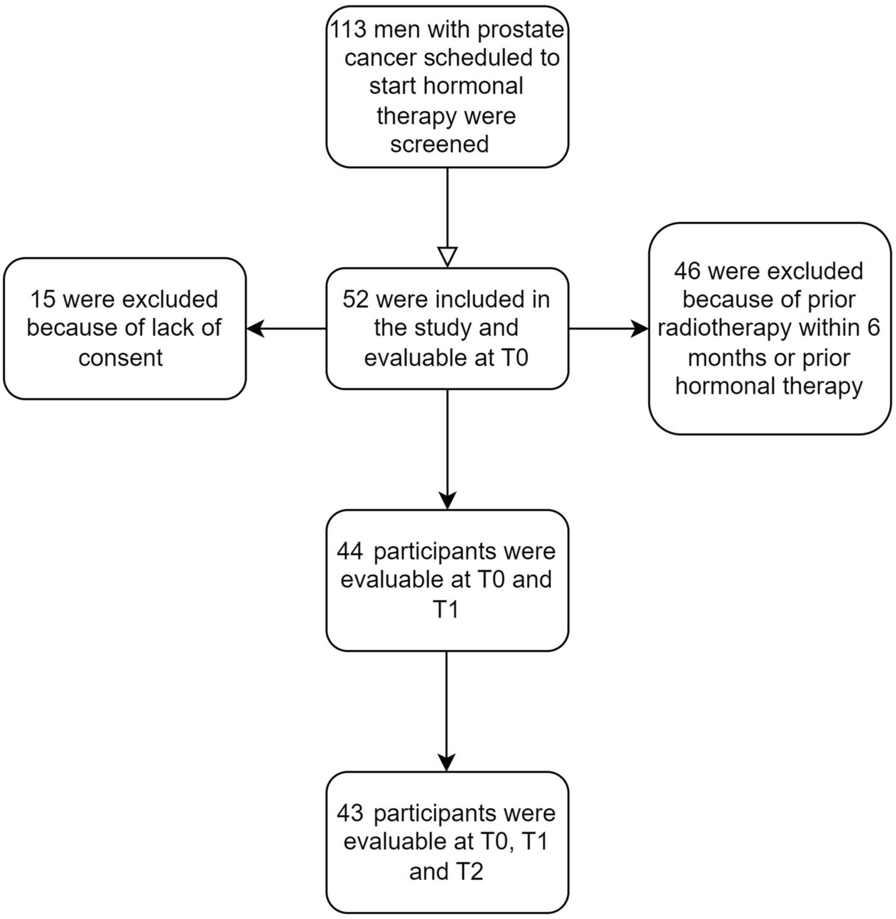

Of the 325 total patients with aRCC included in the study, 219 received NIVO + IPI (67.4%) and 106 received PEM + AXI (32.6%) during months 1–6 (see Fig. 2 for the sample selection flowchart). Of these patients, 210, 119, and 81 receiving NIVO + IPI and 103, 48, and 25 receiving PEM + AXI were included during months 7–12, 13–18, and 19–24, respectively.
Fig. 2
Sample selection of adult patients with aRCC who received 1L therapy of NIVO + IPI or PEM + AXI. Note: aThe list of 1L treatments included avelumab + axitinib, cabozantinib, nivolumab + ipilimumab, pazopanib, pembrolizumab + axitinib, and sunitinib. Abbreviations: 1L first line, aRCC advanced or metastatic renal cell carcinoma, AXI axitinib, FDA Food and Drug Administration, HMO health maintenance organization, IPI ipilimumab, NIVO nivolumab, PEM pembrolizumab, POS point of service, RCC renal cell carcinoma
Characteristics of the Study PopulationsThe median follow-up times were 14.0 (interquartile range 9.4, 23.1) months in the NIVO + IPI cohort and 11.9 (9.3, 17.9) months in the PEM + AXI cohort. The baseline characteristics were generally similar between the two cohorts (Table 1). In both the NIVO + IPI and the PEM + AXI cohorts, the majority of patients were male (75.3% and 69.8%, respectively) and were located in the South or North Central US regions (74.0% and 73.6%). On average, patients in the NIVO + IPI cohort were slightly younger at the index date compared to those in the PEM + AXI cohort (57.7 vs. 60.3 years). Most patients in both cohorts had managed care (NIVO + IPI: 75.8%, PEM + AXI: 64.2%) and, specifically, preferred provider organization (67.1% and 60.4%, respectively) health insurance. The most common metastatic sites were lung (NIVO + IPI: 48.4% and PEM + AXI: 50.0%), lymph node (31.5% and 20.8%, respectively), and bone (29.2% and 28.3%). The mean CCI scores were similar: 7.5 in the NIVO + IPI cohort and 7.4 in the PEM + AXI cohort.
Table 1 Baseline characteristicsaObserved Healthcare Costs for Patients Receiving NIVO + IPI or PEM + AXI over up to 24 MonthsTotal All-Cause and RCC-Related Healthcare CostsCompared to patients treated with PEM + AXI, patients receiving NIVO + IPI incurred higher all-cause and RCC-related healthcare costs only during the first 6 months of 1L treatment and had lower healthcare costs thereafter. Specifically, during months 1–6, patients treated with NIVO + IPI incurred average total all-cause healthcare costs of $46,348 per month while those treated with PEM + AXI incurred $38,097 per month (Fig. 3a). After month 6, the PPPM total all-cause costs for the NIVO + IPI cohort decreased to $26,840 during months 7–12, to $22,899 during months 13–18, and $22,279 during months 19–24, while the PPPM costs for the PEM + AXI cohort decreased to $27,983 and $25,137 in months 7–12 and 13–18, respectively, then increased to $27,947 in months 19–24.
Fig. 3
Temporal trends in unadjusted a all-cause and b RCC-related healthcare costs among patients receiving NIVO + IPI versus PEM + AXI. Abbreviations: NIVO + IPI (N + I) nivolumab + ipilimumab, PEM + AXI (P + A) pembrolizumab + axitinib, RCC renal cell carcinoma
The RCC-related total costs during months 1–6 were $44,059 PPPM in the NIVO + IPI cohort and $36,456 in the PEM + AXI cohort (Fig. 3b). After month 6, the PPPM total RCC-related costs for the NIVO + IPI cohort decreased to $25,144 in months 7–12, $21,645 in months 13–18, and $20,486 during months 19–24, while the costs for the PEM + AXI cohort decreased to $26,692 and $23,709 in months 7–12 and 13–18, respectively, then increased to $25,515 in months 19–24.
All-Cause and RCC-Related Drug CostsDrug costs accounted for most of the total all-cause healthcare costs and were $38,079 (82%) PPPM for the NIVO + IPI cohort and $34,512 (91%) PPPM for the PEM + AXI cohort during months 1–6 (Fig. 3a). After month 6, the PPPM drug costs for NIVO + IPI decreased to $20,730 during months 7–12, $16,534 during months 13–18, and $14,966 during months 19–24, while the costs for PEM + AXI decreased to $24,228 and $21,574 in months 7–12 and 13–18, respectively, then increased to $24,443 in months 19–24. The trends for the RCC-related drug costs were similar to those of the all-cause drug costs (Fig. 3b).
All-Cause and RCC-Related Medical Service CostsMedical service costs accounted for a relatively small portion of the total healthcare costs and were $8269 (18%) PPPM for the NIVO + IPI cohort and $3586 (9%) PPPM for the PEM + AXI cohort during months 1–6 (Fig. 3a). After month 6, the PPPM medical service costs for NIVO + IPI decreased to $6111 from months 7 to 12, then increased slightly to $6365 during months 13–18 and to $7313 during months 19–24, while the costs for PEM + AXI were generally stable at $3755, $3563, and $3504, respectively. The trends for the RCC-related medical service costs were similar to those of the all-cause medical services costs (Fig. 3b).
Cost Differences Between Patients Receiving NIVO + IPI or PEM + AXI over 24 MonthsTotal All-Cause and RCC-Related Healthcare CostsOver the 24 months following the index date, the NIVO + IPI cohort experienced larger decreases in total all-cause and RCC-related healthcare costs compared with the PEM + AXI cohort (Fig. 4). The unadjusted differences in monthly total all-cause healthcare costs between the NIVO + IPI and PEM + AXI cohorts were $8251 (95% CI $4059, $12,527) from months 1 to 6, − $1142 (− $4674, $2407) from months 7 to 12, − $2238 (− $6898, $2445) from months 13 to 18, and − $5669 (− $12,255, $770) from months 19 to 24 (Fig. 4a). After adjustment for baseline characteristics in the model, the differences in monthly total all-cause healthcare costs between the cohorts were $5324 (95% CI $959, $9739) at months 1–6, − $4129 (− $8278, $79) during months 7–12, − $4678 (− $10,418, $868) during months 13–18, and − $10,914 (− $21,436, − $1091) during months 19–24. Thus, the adjusted cost differences between cohorts became smaller from months 1 to 6, favoring PEM + AXI to a lesser degree, and subsequent interval costs differences became more favorable for NIVO + IPI. The trends in the monthly total RCC-related healthcare costs were similar to those of the all-cause costs (Fig. 4b).
Fig. 4
Temporal trends in a all-cause and b RCC-related healthcare costs difference between patients receiving NIVO + IPI versus PEM + AXI (unadjusted and adjusted). *p < 0.05. The error bars represent 95% confidence intervals of the costs difference. Abbreviations: NIVO + IPI nivolumab + ipilimumab, PEM + AXI pembrolizumab + axitinib, RCC renal cell carcinoma
Total All-Cause and RCC-Related Drug CostsSubstantial reductions in all-cause and RCC-related drug costs were also observed for the NIVO + IPI cohort compared with the PEM + AXI cohort in the 24 months after the index date (Fig. 5). The unadjusted differences in all-cause drug costs between cohorts were $3567 (95% CI − $272, $7473) during months 1–6, − $3498 (− $6776, − $213) during months 7–12, − $5041 (− $9292, − $802) during months 13–18, and − $9478 (− $15,978, − $3101) from months 19 to 24 (Fig. 5a). The adjusted differences in all-cause drug costs between the cohorts were estimated at $1137 (95% CI − $2947, $5261) during months 1–6, − $5555 (− $9527, − $1600) during months 7–12, − $7217 (− $13,005, − $1709) during months 13–18, and − $16,682 (− $29,022, − $5055) during months 19–24. Thus, the impact of adjustment reduced the differences in all-cause drug costs between the NIVO + IPI and PEM + AXI cohorts during months 1–6 but resulted in larger differences in all other time periods. A similar trend was observed for the differences in monthly RCC-related drug costs between the NIVO + IPI and PEM + AXI cohorts (Fig. 5b).
Fig. 5
Temporal trends in a all-cause and b RCC-related drug costs difference between patients receiving NIVO + IPI versus PEM + AXI (unadjusted and adjusted). *p < 0.05. The error bars represent 95% confidence intervals of the costs difference. Abbreviations: NIVO + IPI nivolumab + ipilimumab, PEM + AXI pembrolizumab + axitinib, RCC renal cell carcinoma
留言 (0)