The aim of surgical correction is to restore the penis’s normal appearance and function. An appropriately directed urine stream and an erected penis should be the outcomes of surgical urethroplasty [10]. The Snodgrass tubularized incised plate (TIP) urethroplasty has become a primary technique for the repair of distal and midpenile hypospadias. Although many techniques have been introduced for the treatment of hypospadias, urethrocutaneous fistula (UCF) and meatal stenosis, which are the most frequent complications requiring reoperation [11]. Numerous methods for the covering of the urethroplasty have been reported, such as dartos, extragenital tissues, tunica vaginalis, and local subcutaneous penile tissue. Furthermore, fibrin sealants were developed to decrease the occurance of fistulas [12].
Additionally, fibrin sealant and other homologous fibrin materials are utilized to provide a sustaining layer over urethral repair. Fibrin sealants have been utilized as a topical agent for hemostasis and adhesive in tissue approximation during numerous surgical procedures [13]. Kinahan and Johnson were the first to document the application of fibrin sealant during hypospadias surgery [14]. Then, Ambriz-Gonzales et al. propose that fibrin sealant reduces the incidence of urethrocutaneous fistula following hypospadias repair [15]. Nevertheless, Gopal et al.’s largest series demonstrated that fibrin glue could reduce the incidence of fistula formation without completely eliminating the risk of recurrence [13]. Commercial sealants are extracted from the plasma derived from multiple donors so it carries a high risk of blood-borne infections [16]. Allergic reactions are reported after using this material, so the use of an autologous edition from this fibrin material emerged as a solution for these complications.
The utilization of single-donor fibrin sealant for urethrocutaneous fistula repair was suggested by Kajbafzadeh et al. [16]. In their study, they acquired fibrin sealant from a single donor using cryoprecipitation, centrifugation, and incubation.
PRF is utilized as an additive material for TIP repair in this study. PRF is an innovative platelet concentrate that facilitates wound healing and angiogenesis. It resists and combats infection while also contributing to the immune response to damage. PRF enhances the collagen biosynthetic capacity of normal human dermal fibroblasts and promotes their proliferation [17]. Fibrin comprises an assortment of growth factors, including platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), and fibroblast growth factor-basic (FGF-b) [18]. Choukroun et al. were the first to document PRF, and since then, it has been implemented in a number of reconstructive and oral surgical procedures [18].
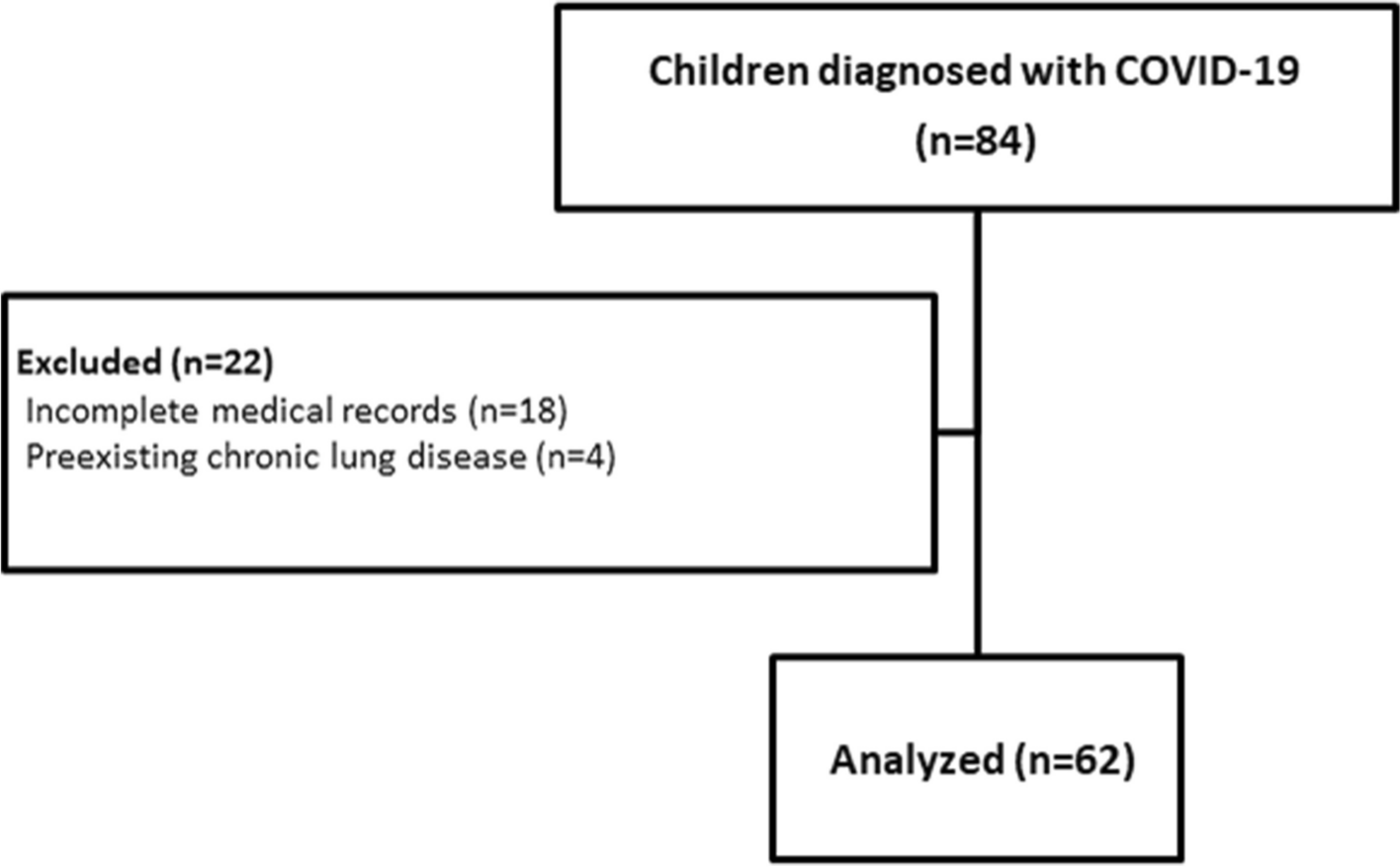
In our current study, we evaluated the usage of the autologous platelets-rich fibrin membrane as a coverage layer in cases of primary distal hypospadias surgeries to decrease the incidence of fistula formation in comparison with the dartos flap coverage layer. The study included 40 patients with primary distal type of hypospadias. Eligible patients were divided into 2 groups to receive either dartos flap (group A) or PRF (group B) as a first covering layer over repair.
In the current study, there were 7 cases of urethrocutaneous fistula (35%) in group A, while 2 patients (10%) in group B. After 6 months of follow-up the two cases of fistula in group B closed spontaneously (0%) while not in group A (35%). The 7 cases of fistula in group A required surgical repair, there was no recurrence of fistula in all cases during the follow-up.
Our findings were consistent with Fouad et al., who enrolled 30 children ages varied from 1 to 6 years, and the success rate was 93.3%, with a complication rate of 6.7%. Our complications in group B using PRF were 10% fistula and 5% meatal stenosis. Foud et al. found that utilizing a platelet-rich fibrin membrane as an intermediate layer for hypospadias surgery in Tubularized Incised Plate Urethroplasty is a feasible and safe option, additionally, the procedure is simple and swift, with few postoperative complications; however, their cases were primary not redo [19].
In another study, Mahmoud et al. reported an overall success rate of 85.6%, which is higher than the current study, and could be attributed to the small number of patients in the current work. However, regarding the urethrocutaneous fistula [UCF] our study findings were similar to 10.0% of the PRF group [20].
Guinot et al. found that the PRF appears to be an effective and safe covering technique. It is a supplementary method to coverage for hypospadias repair surgery [21].
Hassouna et al. found that using Mathieu or Snodgrass procedures to control hypopadias resulted in a 20.0% complication risk. A fistula was the most frequent consequence, with wound breakdown recorded in 5.0%, meatal stenosis in 5.0%, and fistula in 10.0% of cases. Their study included patients as old as 15 years old. Although there were age differences and the absence of the second intermediate layer compared to the current study, our results were higher. This may be due to using different techniques [22].
Our study’s limitation was the relatively small number of patients. To validate our hypothesis, additional randomized comparative studies will be required to determine whether the autologous membrane is truly superior to other tissue-covering flaps or when used in conjunction with them. Furthermore, this method may be considered for re-do cases, circumcised hypospadias, debilitated cases with insufficient covering tissues, and cases lacking a healthy covering layer.




留言 (0)