
記住我


A 5-year-old boy with severe autism spectrum disorder (ASD) presented to the outpatient neurology clinic with concerns of intermittent bilateral lower limb weakness with pain for 2 years. He was non-verbal and had behavioral concerns. He was admitted from the clinic for further investigations as he became non-ambulant, and his symptoms were progressive over the preceding 2 months causing significant concerns for possible underlying degenerative neuromuscular condition.
He had intermittent symptoms of bone pain for 2 years with occasional gait abnormalities of limping and refusal to weight-bear. During these episodes of decompensation, he was reviewed by emergency physicians and pediatricians who diagnosed him with various conditions that ranged from transient synovitis, arthritis, myositis to growing pains to attribute to his symptoms. His neurological examination was always reported to be normal during these medical reviews.
He was admitted 1 year back for further work-up when his symptoms worsened causing him to be non-ambulant. Blood investigations revealed microcytic hypochromic anemia secondary to iron deficiency but the rest of the blood tests for kidney function tests, liver function tests, thyroid function tests and muscle enzymes were normal. Magnetic resonance imaging (MRI) spine, bone scans and positron emission tomography (PET) were performed and they ruled out any underlying spinal pathology or tumors. He was then discharged with physiotherapy (PT) sessions to re-condition his muscle strength. His parents defaulted to regular follow-up with the neurology team and discontinued PT.
He re-attended neurology clinic after 1 year with additional symptoms of bilateral ankle swelling with tenderness which were concerning then of a possible rheumatological condition. In view of his multi-system presentations, he was admitted again for further detailed investigations.
On physical examination, he appeared small for his age with failure to thrive and was generally very irritable. His height was 100 cm (25% for age) and weight was 12.7 kg (3% for age) with a corresponding body mass index (BMI) of 12.7 (< 3% for age) which meant he was significantly underweight (Table 1). There was pitting edema of the ankles with tenderness over the bilateral ankle joints. He was unable to bear weight but his hip joint examination was normal.
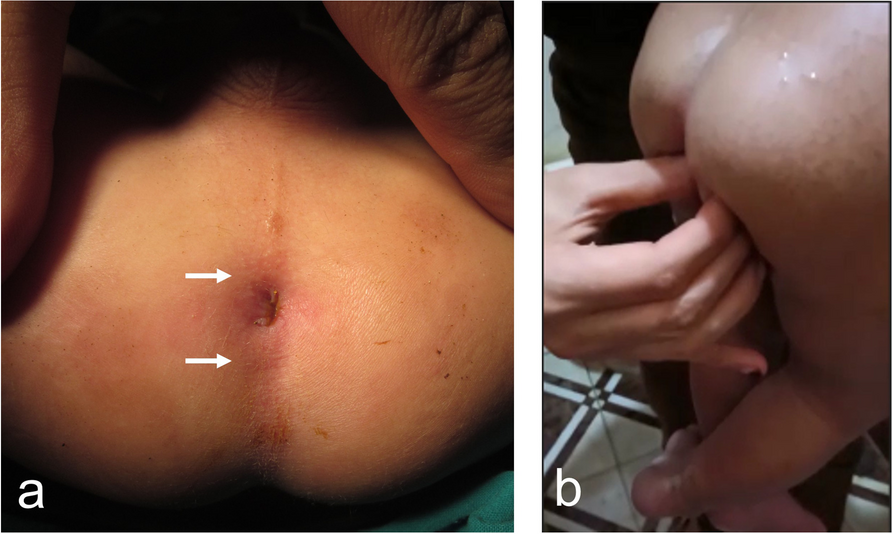
Table 1 Anthropometric measurements of our patientHe had conjunctival pallor suggestive of anemia. There was no clinical evidence of anemic heart failure as he did not have generalized edema or appear breathless. There was gum hypertrophy with contact bleeding on examination of his oral cavity. He had petechial rash over his forearms with peri-follicular hemorrhages on closer inspection of his skin. The rest of his systemic examination including the neurological examination was normal.
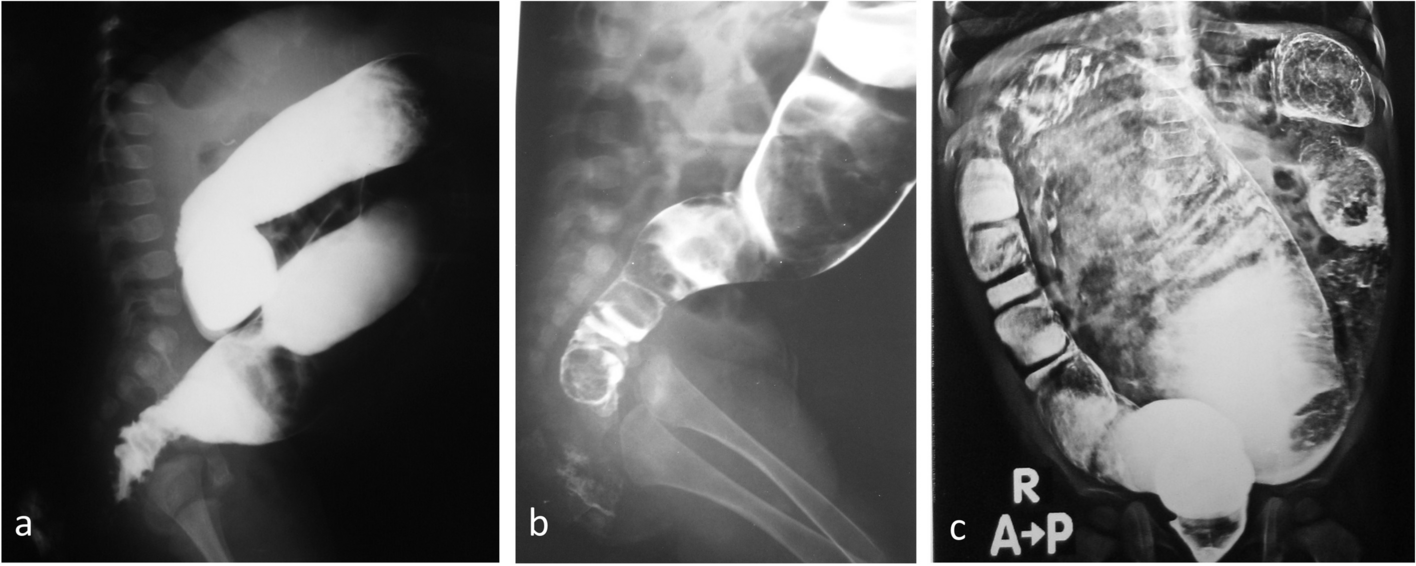
Blood investigations revealed microcytic hypochromic anemia with low iron levels (Table 2). There was no evidence of coagulopathy as his platelet and PT/INR levels were normal. More detailed blood investigations were done to investigate for the cause of persistent iron-deficiency anemia and failure to thrive. Multiple nutritional deficiencies including low folate, vitamin B12, calcium, phosphate, and vitamin D levels were detected (Table 2). Long bone radiographs revealed diffusely osteopenic bones with metaphyseal fraying and splaying, horizontal linear sclerotic bands over metaphyses (Fig. 1). MRI of the ankles and spine showed periosteal reaction over the distal tibia with edema of the surrounding muscles and subcutaneous fat. Bone marrow analysis (BMA) and bone biopsy of the ankle did not reveal any underlying osteomyelitis or malignancy.
Table 2 Blood investigations for our patientFig. 1
Anteroposterior radiograph of knee joint reveals metaphyseal dense bands in bilateral distal femoral metaphyses (white arrows). Bones appear generally osteopenic (star sign) and there is pencil-thin cortex ( blue arrows). Similar findings are also seen in bilateral proximal tibial physes. The findings are characteristic for scurvy
Further blood tests to screen for other nutritional deficiencies revealed low vitamin C levels that cemented his eventual diagnosis of scurvy. In view of his new diagnosis, his skin was examined closely again which revealed the pathognomic sign of corkscrew hair over hyperkeratotic follicles. It was missed previously as the skin was not examined at such close range.
Thereafter, he was managed by a multi-disciplinary team for nutritional rehabilitation. In view of symptomatic anemia, he required a blood transfusion. Subsequently, he was also initiated on multiple nutritional supplementations: vitamin C 400 mg/day, iron drops 80 mg/day (6 mg/kg/day), calcium 500 mg/day, vitamin D3 2000 unit/day, folic acid 5 mg/day. They were titrated with the advice of the dietician during the inpatient review. He received these supplements for 3 months with biochemical and clinical improvement in his nutritional status. Endoscopy did not reveal any underlying gastrointestinal pathology or malabsorptive conditions to account for the multiple nutritional deficiencies. He was noted to have poor dietary habits and a detailed nutritional assessment revealed a limited variety of food intake. He rarely consumed any fruits or vegetables, rejected all forms of milk feeds and predominantly consumes carbohydrates in the form of plain crackers, rice or bread. This has been his diet since he started weaning diet at 6 months of life.
His restricted dietary preferences were attributed to his underlying condition of ASD which caused him to be a picky eater. He was discharged with the dual diagnoses of scurvy and vitamin D-dependent rickets which explained his predominantly musculoskeletal symptoms. On follow-up, his anemia had resolved within 4 months of iron therapy (from 5.7 g/DL to 11.1 g/DL). His musculoskeletal symptoms completely resolved and he was ambulant after initiating nutrition supplementation within 1 month post-discharge.
留言 (0)