Recently, the incidence of CPP has increased worldwide. The diagnosis of CPP is based on clinical features, which are confirmed by hormonal and radiographic investigations [16]. However, this can be misleading, which makes it more challenging to diagnose [17]. CPP can result in various adverse effects including early menarche, premature epiphyseal closure leading to shorter target adult height, and psychological issues. Hence, it is essential to detect CPP early and develop simple screening methods to make easier decisions about starting treatment and improve the quality of life of patients [18].
The gold standard test for diagnosing CPP is intravenous GnRHST which confirms the premature activation of HPG axis [19]. A pubertal response is defined by an increase in LH concentration ≥ 5 IU/L which indicates CPP [15]. However, this test is time-consuming and expensive as it requires repeated blood sampling. Moreover, the clinical utility of the test in certain circumstances can be limited [11].
The availability of commercial intravenous synthetic GnRH is limited in some countries, including Egypt. Therefore, GnRH analogs such as triptorelin 0.1 mg injection are sometimes used [20]. The half-life of triptorelin is longer, and it has a stronger affinity for the GnRH receptor, raising uncertainties about the ideal sampling time of gonadotrophins after triptorelin stimulation [21]. There are also concerns regarding the lack of agreement on basal and stimulated LH and FSH cut-off values used to diagnose CPP [22]. Hence, a conclusive single diagnostic biomarker is needed to eliminate the need to perform GnRHST.
Previous studies have suggested basal serum LH as the most sensitive biomarker to differentiate between CPP and premature thelarche, rendering it suitable as a substitute for GnRHST [23, 24]. This is similar to our study that shows that there was a statistically significant difference in basal LH levels between CPP and control groups (p < 0.001*).
Moreover, there was a statistically significant positive correlation between basal LH and different clinical and radiological parameters such as Tanner staging (p < 0.001*), height SDS (p = 0.005*), bone age advancement (p < 0.001*), and uterine dimensions (p = 0.007*). Therefore, combining those parameters with high basal LH levels could aid in the diagnosis of CPP. Similarly, You et al. [20] developed a clinical score model for CPP among girls which consisted of four variables: age at start of puberty, basal LH level, largest ovarian volume, and uterine volume. This score may predict CPP and has been proposed to help in assessing the need for further GnRHST.
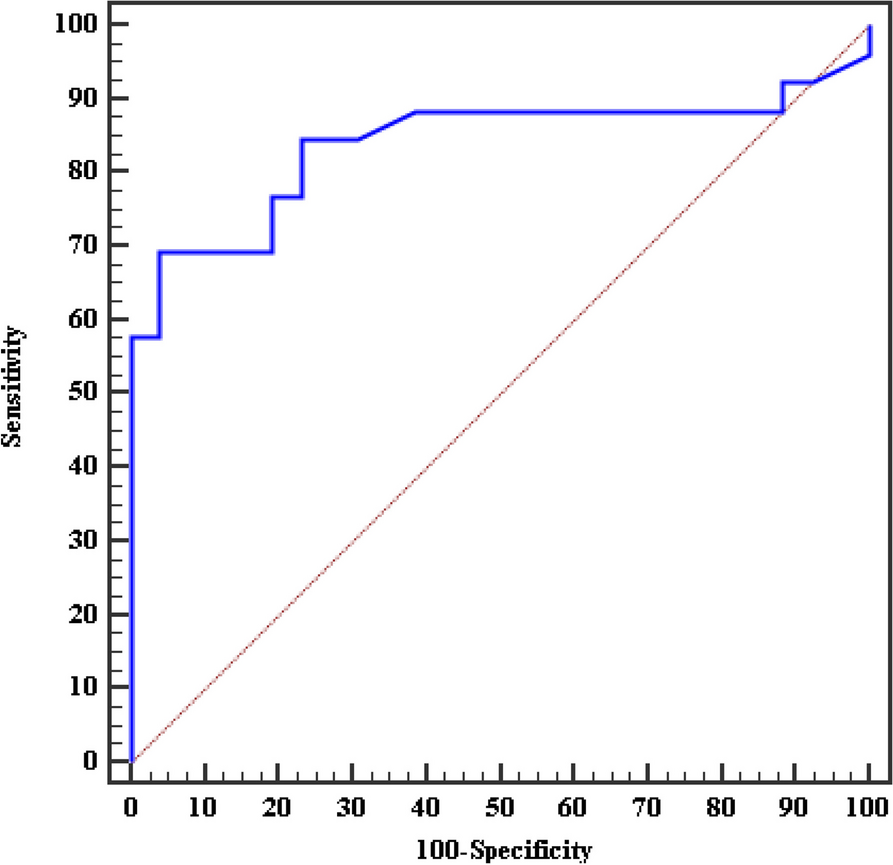
However, until now, there are no consistent cut-off values of basal LH as a diagnostic predictor of CPP. In different centers, it has varied from 0.1 to 1.5 IU/L with a sensitivity and specificity ranging between 60 and 100% [21, 23,24,25]. In the present study, the best basal LH cut-off was chosen at a value of 0.29 IU/L, with sensitivity 84.62% and specificity 76.92% (AUC 0.840). Therefore, we propose that basal LH > 0.29 IU/L could be used as a better discriminator for children with CPP.
Our results are consistent with the findings of Heo et al. [23] who studied the cut-off values in CPP and showed that levels > 0.245 IU/L had 88% sensitivity in confirming the diagnosis (p = 0.049*, AUC = 0.764). Durá-Travé et al. [26] results also showed higher sensitivity and specificity for basal LH levels (89 and 82% respectively) in 241 girls with breast enlargement between 6 and 8 years. Moreover, Lee et al. [27] studied 21 girls with CPP demonstrating a strong correlation between single basal unstimulated LH and GnRHST (r = 0.532, p < 0.001*) and proposed that basal LH levels ≥ 0.22 IU/L indicate CPP diagnosis, with a lower sensitivity compared to our results (69.4%) [28].
Additionally, Lee et al. [27] demonstrated that basal LH/FSH ratio was a significant predictor of positive response during GnRHST with significant differences between the 2 studied groups (p < 0.001*). Basal LH/FSH ratio has also been suggested to be more efficient in diagnosing children with pubertal changes with a cut-off value of 0.07 (low sensitivity and specificity of 73.2% and 89.5%) [28]. This was not observed in the present study as there was no statistically significant difference in basal LH/FSH ratio between girls with CPP and controls (p = 0.913). Perhaps, this could be attributed to the smaller sample size in our study (26 patients) in comparison to 121 CPP patients in the former study. Furthermore, combining basal LH level (cut-off 0.2) and basal LH/FSH ratio (cut-off 0.1) was proposed to be an easier method to diagnose CPP in 86 Thai girls between 6 and 8 years, with 71.4% sensitivity and 100% specificity [29].
In females, AMH is primarily produced by the ovarian granulosa cells and plays an important role in regulating sex hormone production in relation to onset of puberty. During childhood, AMH is at its lowest level. It increases gradually within 3 years before puberty, reaching its highest levels after puberty [30]. Despite demonstrating that basal LH can aid in the diagnosis of CPP in the present study, basal AMH failed to show a statistically significant difference between CPP girls and control group (median 1.3 vs 1.1 ng/ml, p = 0.07). This indicates that basal AMH could not be used as a marker in the initial screening of patients with early puberty.
Conversely, Muratoğlu Şahin et al. [30] investigated AMH in infants with premature thelarche (PT) and reported that AMH levels in PT were significantly lower than control group (1.66 vs 1.96 ng/ml, p = 0.025*), even though both were within normal range. These results implied that AMH may play an inhibitory role in breast development during infancy. Furthermore, Chen et al. [31] proposed that girls with progressive CPP had lower serum AMH in comparison to non-progressive CPP in a study enrolling 148 girls with early puberty. However, in the present study, the rate of progression of CPP was not assessed.
CPP is characterized by increased height velocity, advancement of bone age, and premature epiphyseal closure due to the effect of estradiol on bone growth. Therefore, it has been suggested that when BA is advanced, more than 2 SD in comparison to CA, premature thelarche is unlikely [26]. Similarly, BA was advanced in 17 CPP girls (65.4%) in our cohort indicating that BA could be frequently used as an additional clue, raising clinical suspicion of CPP. Nonetheless, we cannot rely on BA as a sole investigation to diagnose CPP, because only 63.2% of patients (12/19) had pubertal basal estradiol levels ≥ 10 pg/ml. These results are in accordance with the findings of Xu et al. [32].
Finally, the role of pelvic ultrasonography in CPP has been described in recent studies [33,34,35]. Normally, elevated gonadotrophin levels lead to enlargement of the ovaries and uterus in the later stages of puberty [35]. Pubertal uterine dimensions were observed in only half of the patients (13/26) in the present study. However, in the literature, there are contradictory results regarding the effectiveness of uterine dimensions in predicting CPP [33,34,35].
The present study has some limitations, including the small sample size which might have hindered finding a statistically significant difference between CPP and control groups. Lack of intravenous GnRHa due to unavailability made it difficult to compare peak LH, FSH, and LH/FSH ratio after GnRH stimulation with similar studies using intravenous route. Another limitation was the lack of a follow-up period to detect the course of CPP.



留言 (0)