
記住我



A 3-kg term male neonate was referred on the third day of life with an antenatal diagnosis at 34-week gestation of a sizable genitourinary cystic mass, approximately 10 × 10 cm in size. The prenatal ultrasound indicated that the mass might have originated from the bladder. The rest of the antenatal ultrasound, including amniotic fluid volume, was unremarkable. The neonate was delivered via caesarean section due to the identified foetal anomaly.
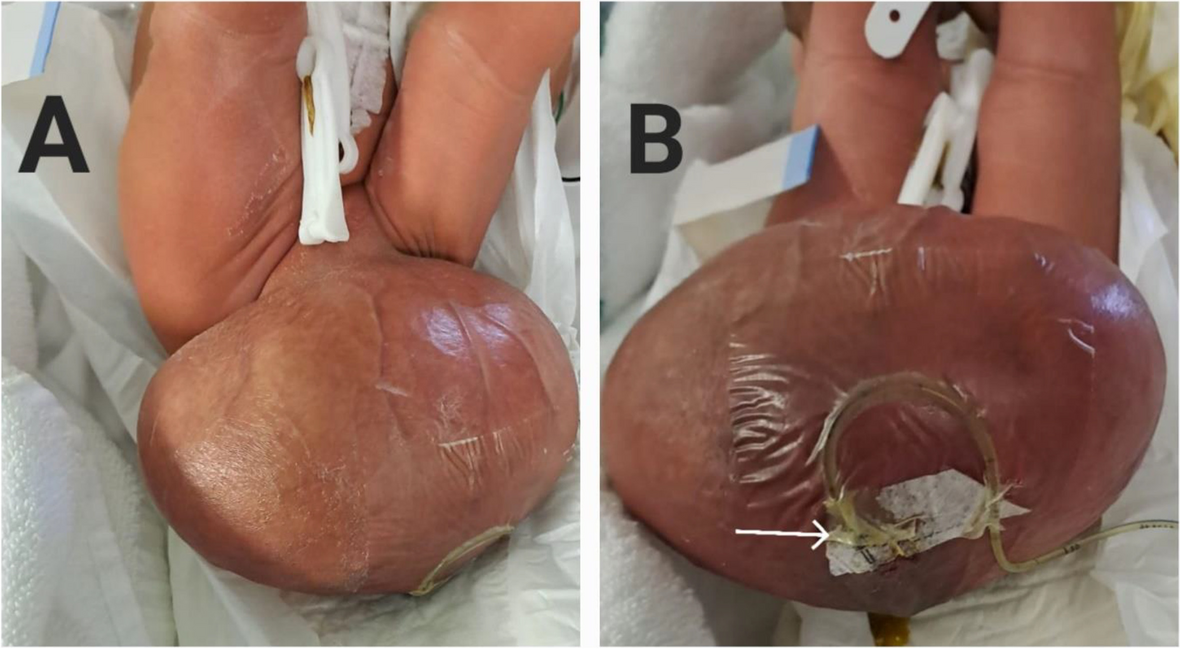
Physical examination revealed a large, non-tender cystic mass covered by the skin, located just below the pubic symphysis. The penile shaft displayed elongation and flattening on the ventral aspect of the mass, with a single urethral opening and voiding occurring through a compressed glans. A size 6-French feeding tube was inserted through the visible urethral opening in the glans to catheterize the urethra and drain the bladder (Fig. 1). Both testes were palpable in the inguinal region. No other anomalies were detected, and initial laboratory tests were normal. Ultrasonography confirmed the presence of a cystic mass measuring 12 × 8 × 9 cm, dorsal to the glans and shaft of the penis. Hydronephrosis was absent.
Fig. 1
Large cystic mass dorsal to penile shaft. A Extending from region of the pubic symphysis. B Flattened penile shaft and glans with 6-French feeding tube in ventral urethra
On day 8 of life while waiting for further imaging, the neonate developed signs of sepsis suspected to arise from the cyst as evident from observed erythema on the overlying skin. He was irritable, and laboratory results revealed elevated C-reactive protein and procalcitonin levels, 234 mg/L and 3.26 ug/L, respectively, and a decrease in the white blood count. Odorous straw-coloured fluid was aspirated from the cyst under ultrasound guidance, and a 7-French 20-cm central venous catheter was inserted into the cyst to drain the collection. Fluid analysis confirmed urinary origin and showed elevated urea and creatinine levels (fluid urea and creatinine levels of 27.7 mmol/L and 1109 µmol/L, respectively, in contrast to serum urea levels of 3.2 mmol/L and creatinine levels of 35 µmol/L). Klebsiella pneumonia was cultured from the fluid, leading to intravenous antibiotic treatment with meropenem for 7 days.
A computed tomography (CT) scan was performed due to the patient’s septic state, showing a large cystic mass, 10 × 6 cm in size, attached centrally and anteriorly to the groin. The drain was identified within the mass, and no bladder communication was observed.
A few days later, urethral communication with the cystic mass was clinically evident after displacement of both the transurethral feeding tube and drain, coinciding with cyst enlargement noted during voiding. Once antibiotics were completed, a voiding cystourethrogram (VCUG) was performed, revealing a normal-shaped bladder and a dilated posterior urethra with contrast extravasation from the anterior aspect of the posterior urethra into the cystic mass (Fig. 2).
Fig. 2
Lateral view of a voiding cystourethrogram depicting the Type IIA-2 urethral duplication in a sagittal plane (long thin arrow, dorsal hypoplastic urethra arising from posterior urethra; short thick arrow, contrast extravasation from the dorsal urethra into the cystic mass; short thin arrow, ventral urethra)
At the age of 3 weeks, the patient underwent surgical intervention. The functional ventral urethra terminated centrally in the glans, flanked by both corpora cavernosum on either side of the corpora spongiosum. Cystoscopy revealed a long, patent urethra with an unobstructive tissue fold between the prostatic and membranous urethra. During cystoscopy, the cyst is filled with fluid; while no immediate communication was evident, it later became apparent upon cyst opening and catheterization of a small-calibre ‘urethral-like’ opening resembling an underdeveloped glans on the cyst’s posterior wall using a 3-French ureteric catheter (Fig. 3A, B).
Fig. 3
Intra-operative confirmation of a Type IIA-2 urethral duplication with reconstruction of the penis. A Open dorsal penile cyst (short, thick arrow, dorsal urethra opening on posterior wall of cyst; long thin arrow, ventral urethra opening). B 3-French ureteric catheter in small calibre dorsal urethra communicating with posterior urethra. C Reconstruction of penile shaft after excision of cyst and excess skin
The dorsal hypoplastic urethra, approximately 4 cm in length, coursed along the cyst’s posterior wall and communicated with the anterior wall of the posterior urethra, indicative of a Type IIA-2 complete urethral duplication. Remnants of underdeveloped corpora cavernosa were evident on either side of the dorsal urethra.
The dorsal hypoplastic urethra was secured with a 6–0 monofilament absorbable suture and divided near its entry point into the posterior urethra. Complete excision of the cyst was performed. The ventral urethral corpora cavernosa were rotated dorsally and sutured using 4–0 polyglactin. Orchidopexies were conducted to address bilateral undescended testes located in the inguinal region. Scrotal skin was reconstructed for cosmesis, and excess dorsal skin was excised (Fig. 3C). As part of the postoperative care strategy, a 6-French feeding tube was inserted as a transurethral catheter into the ventral urethra for wound care. The ventral penis measured approximately 8 cm in length at the conclusion of the procedure.
Perioperative antibiotics consisted of three doses of cefazolin. Empiric meropenem was initiated following a post-surgery temperature spike and continued for 7 days. Multidrug-resistant (MDR) Acinetobacter, sensitive to colistin, was isolated from a peripheral blood culture. Despite the positive culture, no changes were made to the antibiotics as the patient remained clinically well. Post-operative analgesia included intravenous fentanyl and paracetamol for 24 h, followed by oral paracetamol for 6 days. Daily paraffin gauze dressings were applied. After 1 week, the transurethral catheter was removed, and the patient voided well and was discharged home (Fig. 4A).
Fig. 4
Post-operative results. A One week. B Two months
The histology of the urethral fistula showed stratified squamous epithelium and stromal fibrosis. The cystic lesion was lined by keratinizing squamous epithelium, and stromal fibrosis was noted. At the 2-month follow-up, we observed a satisfactory urinary stream and acceptable cosmetic outcomes, even though there was dorsal skin excess and a floppy penis (Fig. 4B). The guardian of the patient was pleased with the results. Further review after 6 months demonstrated a good urinary stream and cosmetic result with spontaneous erections noted by the guardian.
留言 (0)