
記住我


Data for the study were obtained from the Centers for Medicare and Medicaid Services (CMS) Chronic Conditions Warehouse (“the database”). The database includes demographic, enrollment, and claims information on all persons enrolled in Medicare FFS plans (i.e., Medicare Parts A, B, and D) in the USA. Information available for each person in the database includes age, sex, race, location, and dates of enrollment. Data available for each outpatient pharmacy claim (prescription filled) include the drug dispensed (in National Drug Code format), the dispensing date, and the quantity and number of therapy-days dispensed. Data available for each facility or professional service claim (“medical claim”) include dates of service and diagnosis, and procedure codes (in International Classification of Diseases, 9th Edition, Clinical Modification [ICD-9-CM] or 10th Edition, Clinical Modification [ICD-10-CM] format). Professional service claims also include procedure codes (typically in Current Procedural Terminology, Version 4 and Health Care Financing Common Procedural Coding System formats). All claims in the database include information on paid amounts (including copays, coinsurance, and deductibles). For each person in the database, claim-level data may be arrayed in chronological order to provide a detailed, longitudinal profile of all medical and pharmacy services received. A custom subset of the databases was provided to the investigators by CMS that consisted of all available data from the database for all patients who had one or more claims with a diagnosis of MM (ICD-9-CM code 203.0x or ICD-10-CM code C90.0x) from 2007 to 2020. Claims for these patients spanned the period from November 14, 2006, to December 31, 2020 (the “study period”), and therefore reflect treatment patterns prior to the use of BCMA- and GPRC5D-targeted immunotherapies.
Use of the data was governed by a Data Use Agreement (DUA) from CMS (DUA number: RSCH-2022-58036). The study protocol was reviewed and approved by the Advarra institutional review board (IRB Organization number [IORG]: 0000635. Protocol number: Pro00057753). This study is in compliance with the Declaration of Helsinki of 1964 and its later amendments. This study has also been reviewed and approved by an ethics committee as part of the IRB review conducted by Advarra. Given this study used deidentified, retrospectively captured clinical data, participant consent was not required. The IRB granted a Waiver of Consent for this study. No identifiable information is included in the manuscript.
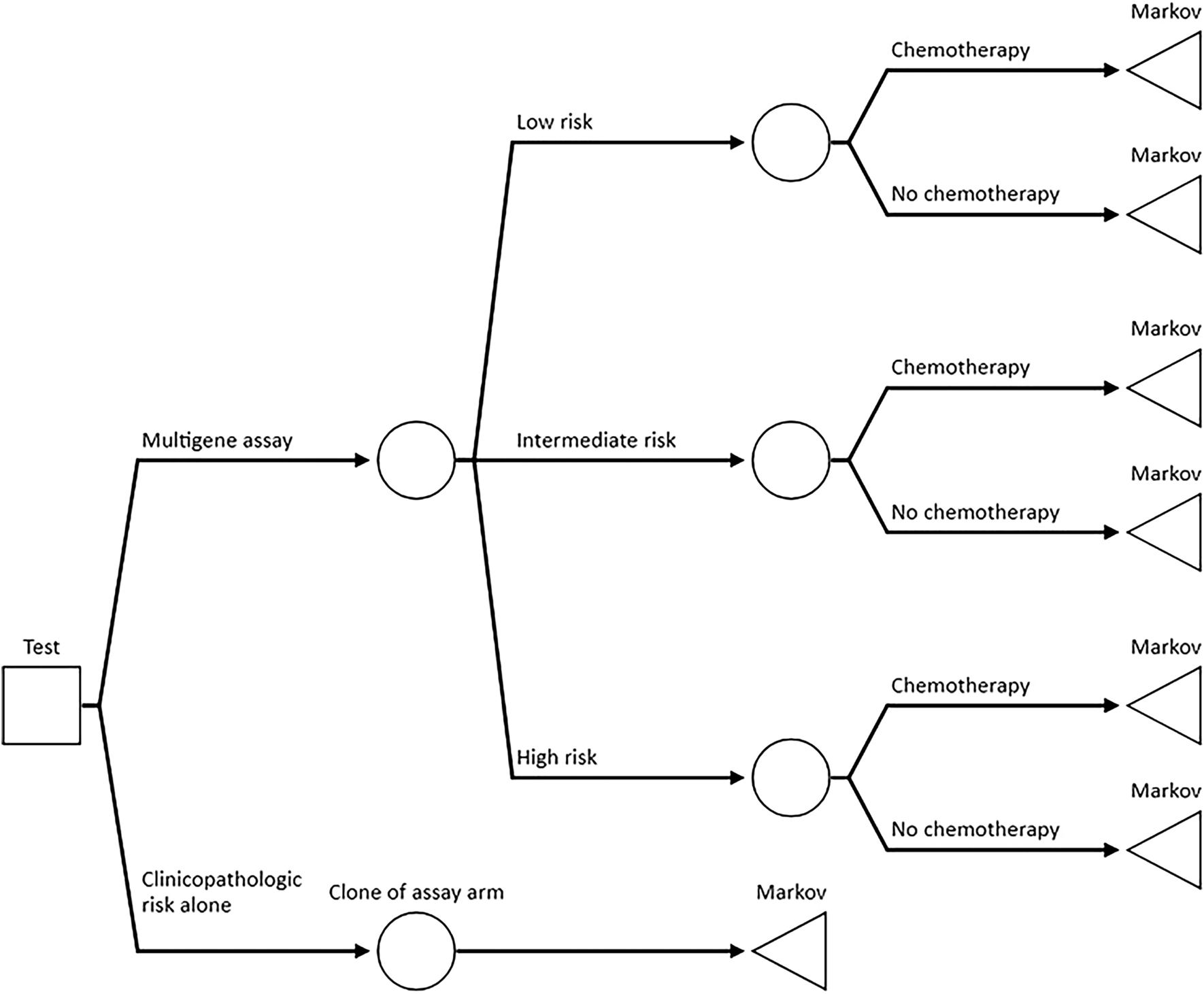
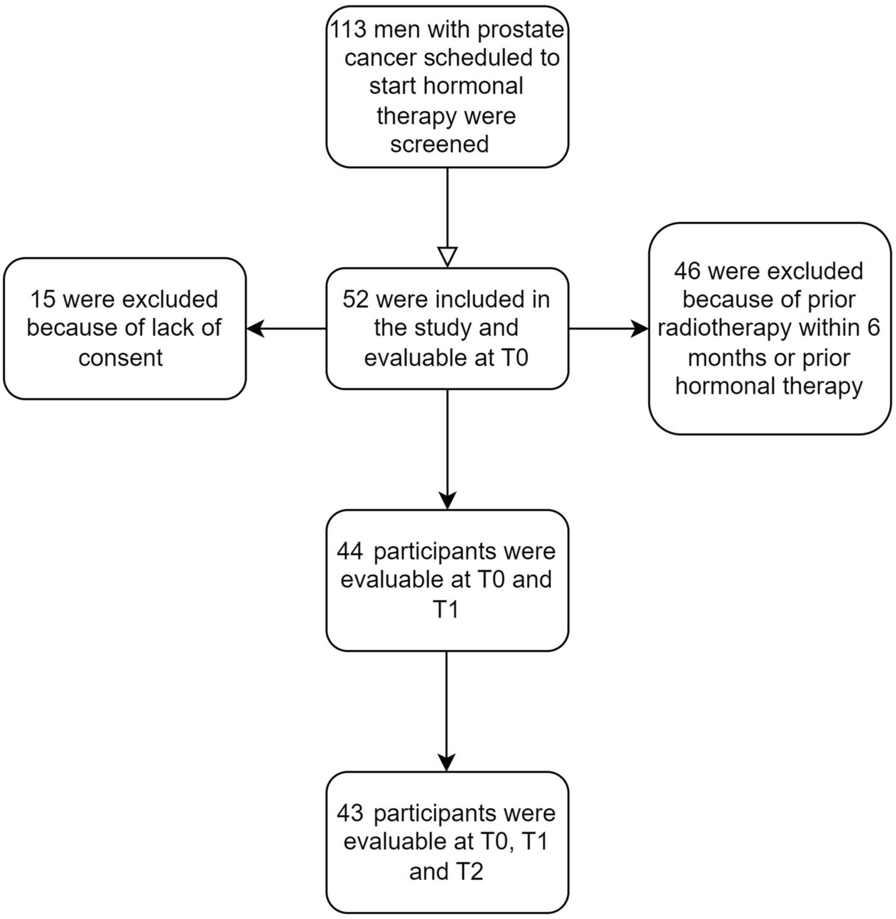
Study DesignAn incident user cohort design was used (Fig. 1) [17]. A total of four study cohorts were examined: the TCE, TCR, PE, and PE-TCR cohorts. The PE and TCR cohorts were subsets of the TCE cohort, and the PE-TCR cohort was a subset of the PE and TCR cohorts. To identify the cohorts, patients with a diagnosis of MM during the study period were first selected from the database. The date of the first diagnosis of MM was designated the “MM diagnosis date.” The period from the MM diagnosis date to the end of the study period was partitioned into lines of therapy (LOTs) based on medical and pharmacy claims for MM medications, using an adaptation of a published algorithm that had undergone extensive review and refinement by clinical experts [18, 19]. For the TCE and PE cohorts, the start date of the first LOT that qualified the patient as TCE or PE was defined as the “TCE date” or the “PE date,” respectively. For both cohorts, the first LOT after becoming TCE or PE was defined as the “index LOT,” and the start date of the index LOT was defined as the “index date.”
Fig. 1
Study design schematic. MM multiple myeloma, TCE triple-class exposed
For all patients, the “pre-index period” was defined as the 180-day period prior to the index date, and the “follow-up period” was defined as the period from the index date to the end of continuous enrollment, death, or the end of the study period, whichever occurred first. Demographic and enrollment characteristics were assessed at the index date, and comorbidities were assessed during the pre-index period. Outcomes were assessed during the follow-up period and included MM medications and treatment regimens received for the index LOT, time to discontinuation (TTD) and TTNT for the index LOT, HRU, and HCC from the index date to the end of follow-up, and OS from the index date. Diagnosis and procedure codes used in the study are listed in the Supplementary Materials (Tables S1–S25).
Study PopulationPatients meeting the following criteria were selected for inclusion in the TCE and PE cohorts:
Confirmed diagnosis of MM (ICD-9-CM code 203.0x or ICD-10-CM code C90.0x) during the study period, where a “confirmed diagnosis” was defined for the study as (a) one or more inpatient claims with the diagnosis or (b) two or more non-diagnostic outpatient claims with the MM diagnosis within 30–365 days apart; and
For the TCE (PE) cohorts, treatment with one (two) or more PI(s), one (two) or more IMiD(s), and one or more anti-CD38 mAbs on or after MM diagnosis date; and
Continuous enrollment from 6 months prior to the MM diagnosis date through TCE date; and
Aged ≥ 18 years as of the MM diagnosis date; and
One or more LOTs after becoming TCE (or PE); and
No claims for allogeneic SCT before the index date; or
Continuous enrollment from the TCE (or PE) date to 30 days post-index.
For both the TCE and PE cohorts, subgroups of patients who were also TCR at the TCE and PE date, respectively, were identified. The “TCR cohort” included all TCE patients who were TCR as of the TCE date. The “PE-TCR cohort” included all patients who were TCR as of the PE date. Patients who were TCE or PE and became TCR after the TCE or PE date, respectively, were not included in the TCR or PE-TCR cohorts. The index dates used for analyses of the TCR and PE-TCR cohorts were the same as those used for the patients in analyses of the TCE and PE cohorts, respectively. TCE and PE patients were considered TCR if they were refractory to one or more regimens including a PI, one or more regimens including an IMiD, and one or more regimens including an anti-CD38 mAb. Patients were considered refractory to any regimen if the period between the last claim or days supplied for any drug in the regimen and the start of the subsequent regimen was < 60 days, and none of the drugs in the regimen were present in the next regimen [20].
LOTsLOTs were assessed by first identifying all claims for MM therapies on or after the MM diagnosis date and sorting the claims chronologically. MM therapies included IMiDs (thalidomide, lenalidomide, pomalidomide), PIs (bortezomib, carfilzomib, ixazomib), anti-CD38 mAbs (daratumumab and isatuximab), other mAbs (elotuzumab), histone deacetylase inhibitors (panobinostat), other MM therapies, and SCTs. For simplicity, claims for corticosteroids (dexamethasone or prednisone) were not considered in the identification of LOTs. The first date with a claim for any MM therapy following the MM diagnosis date was defined as the initiation date for the first LOT (LOT1). The 60-day period beginning with the LOT1 initiation date was defined as the “treatment identification period” for LOT1. All medications received during the LOT1 treatment identification period were assumed to constitute the LOT1 regimen, except for the maintenance therapy described below. The start date for the second LOT was then identified based on the earliest (a) date of the first claim for a new MM therapy that was not among the MM medications constituting the LOT1 regimen (excluding lenalidomide maintenance therapy), or (b) date of the first claim for any MM therapy occurring > 180 days after the last claim or days supplied for any of the medications in the LOT1 regimen (i.e., a gap of 180 days in treatment was assumed to constitute the end of the LOT). Lenalidomide maintenance was identified when (a) the first claim for a new MM therapy after the LOT1 treatment identification period was lenalidomide, (b) the first such claim was ≤ 60 days after the most recent prior claim for a medication in the regimen, and (c) there were no claims for any other MM therapy in the 60-day period beginning with this lenalidomide claim. The start and end dates for subsequent LOTs were identified using the same approach as described above, except for maintenance therapy and any autologous SCT (ASCT) received after LOT1, which was considered part of the regimen.
Baseline CharacteristicsFor each patient, age (in years), sex, and race (non-Hispanic white, non-Hispanic Black, other, or unknown) were described. The year of index date was recorded. The prevalence of selected comorbidities (anemia, chronic obstructive pulmonary disease, chronic liver disease, chronic pain, chronic kidney disease [CKD], coronary heart disease, dementia, diabetes, and hypertension) were assessed based on diagnosis and procedure codes on medical claims during the 6-month pre-index period. The National Cancer Institute Modification of Charlson Comorbidity Index (NCI-CCI) was also calculated based on claims during the 6-month pre-index period [21]. Prior exposure to MM medications and ASCT, the number of prior LOTs for MM, and the number of months between the initial MM diagnosis and the index LOT were assessed for each patient.
OutcomesFor each patient, MM treatment regimens received for the index LOT were assessed. TTNT for the index LOT was defined as the number of days from the index date to the date of initiation of the next LOT. TTD for the index LOT was defined as the number of days from the index date to the last day of therapy for the LOT. The last day of therapy for the LOT was defined as (1) the day of the last claim or days supplied for a regimen medication occurring before the first day of the next LOT, or (2) the last claim or days supplied for a regimen medication preceding a gap of 180 days without a claim, or days supplied for a regimen medication. OS from the index date was assessed using date of death information in the database, based on information from the Medicare claims, the Social Security Administration, supplemented with online date of death edits submitted by family members, and other sources [22]. Over 99% of death dates are validated [22].
For each patient, measures of HRU were calculated over the follow-up period and included the number of prescriptions, the number of physicians’ office or hospital outpatient visits, the number of emergency department visits, the number of hospitalizations, and the number of inpatient days.
For each patient, MM medication costs, other MM-related costs, non-MM-related costs, and total all-cause costs were calculated over the follow-up period. Costs of administration were included in the costs of MM medications and were identified based on claims with procedure codes for chemotherapy administration for which there was a claim for an MM medication on the same date. Other MM-related costs included (a) costs of inpatient claims with a diagnosis of MM in any position or an MM-related adverse event (AE) or complication in the primary position and (b) costs of outpatient claims with an MM diagnosis in any position. MM-related AEs and complications were identified based on published studies derived from MM treatment guidelines (complications) and published prescribing information [19]. Costs were estimated based on reimbursed amounts and adjusted to 2021 US dollars [23].
AnalysisThe number and percentage of patients meeting each of the inclusion and exclusion criteria were reported in an attrition table. Descriptive statistics on patient characteristics were reported for each cohort. Binary and categorical variables were reported as numbers and percentages. Means and standard deviations (SDs) were reported for continuous measures. For each cohort, treatment regimens were alternately classified based on specific medications received (e.g., pomalidomide, carfilzomib, daratumumab) and medication classes (e.g., IMiDs, PIs, anti-CD38 mAbs). TTD and OS were analyzed using Kaplan‒Meier (KM) methods. For TTD and OS, patients with missing values were censored at the end of the follow-up period for each patient. Descriptive statistics were calculated for TTNT for patients who received an LOT after the index LOT. TTNT was also analyzed using cumulative incidence methods, with death as a competing risk. Means and SDs were reported for all measures of HRU and HCC. HRU and HCC measures were reported on a per-patient-per-month (PPPM) basis to account for variable lengths of follow-up across patients. When calculating PPPM estimates, patients were weighted by the number of months of follow-up to ensure that the average PPPM estimates would equal the sum of the units of HRU or HCC over all patients divided by the corresponding sum of the months of follow-up. The 95% confidence intervals (CIs) were calculated for time to event outcomes. Consistent with the CMS DUA, numbers and descriptive statistics for cells with N < 11 were redacted and reported as “N < 11.”
留言 (0)