Background and rationale
In recent years, the rapid increase in non-communicable diseases has posed a significant health challenge, threatening the well-being and economic progress of societies. Chronic non-communicable diseases such as cardiovascular diseases, cancer, respiratory diseases, and diabetes mellitus are the leading causes of death globally [1].
Heart failure, for example, is a progressive condition where the heart muscle is unable to adequately pump blood to meet the body’s needs [2].
The symptoms and complications of these diseases can significantly impact patients’ quality of life, increasing the risk of hospitalization and mortality [3]. The American Heart Association (AHA), 2014 reports that approximately 7.3% of all deaths from cardiovascular diseases are due to heart failure. It is predicted that by 2030, more than 23.3 million individuals will lose their lives annually due to cardiovascular diseases, and the prevalence of heart failure is expected to increase by 25% [4].
The prevalence of heart failure in Iran has been reported as 8%, which is higher than in other Asian countries, including Japan (0.8%), China (3.5%), and India (0.3%) [5]. Common symptoms of heart failure include fatigue, loss of appetite, shortness of breath, ankle swelling, and exercise intolerance [6].
In recent years, oxidative stress and inflammation have gained significant attention as key pathophysiological elements of the heart failure syndrome and potential factors in the development of heart failure. The dysfunction of cardiac mitochondria is a symptom of heart failure and a major contributor to oxidative stress, which in turn has damaging effects on cellular components, including the mitochondria themselves, leading to the creation of a defective cycle. Oxidative stress leads to damage and inflammation of the myocardial tissue, ultimately contributing to the development and progression of heart failure. Some markers of oxidative stress and inflammation are increased in chronic heart failure and have prognostic importance. Uric acid is a biomarker of oxidative stress in heart failure patients, and high uric acid levels are a risk factor for adverse outcomes, including mortality. The prevalence of hyperuricemia in patients with heart failure has been reported to range from 30 to 60% [7].
Moreover, increased oxidative stress leads to a reduction in the bioavailability of nitric oxide. In this condition, nitric oxide (NO) is deactivated by superoxide anions, and this reaction can potentially generate peroxynitrite, which is a toxic substance. Numerous studies have indicated that patients with heart failure experience a decrease in the body’s nitric oxide levels, potentially leading to elevated blood pressure and inflammation in the heart vessel walls [8, 9].
Monocyte chemotactic protein 1 (MCP-1) is a cytokine with pro-inflammatory properties, which is generated in reaction to injury or exposure to other cytokines. Its concentration rises in individuals with heart failure, potentially leading to a significant inflammatory response and the development of atherosclerosis [10, 11].
Blood lipid levels play a crucial role as risk factors for heart failure. Atherogenic index of plasma (AIP) is a strong predictor for assessing the risk of atherosclerosis and coronary heart disease, calculated using the formula (log) TG/HDL-C [12, 13]. The amount of AIP is notably higher in patients with heart failure compared to healthy individuals and is inversely related to left ventricular ejection fraction (LVEF) [14, 15].
Due to these reasons, antioxidants or anti-inflammatory medications may yield beneficial results in managing patients with heart failure [16,17,18].
Astaxanthin, a carotenoid similar to carotene and lycopene, is commonly found in nature, particularly in naturally occurring deep red seafood such as salmon, shrimp, and crab [19]. As humans are unable to produce carotenoids, astaxanthin must be acquired through dietary sources [20]. As per reports, astaxanthin exhibits a potent antioxidant effect that is more than 100 times stronger than alpha-tocopherol [21]. Astaxanthin also possesses various properties including anti-inflammatory, anti-oxidative stress, anti-cancer, immune system modulation, and blood pressure reduction [22,23,24]. In 1999, the US Food and Drug Administration approved astaxanthin for use as a dietary supplement [25]. Astaxanthin, derived from microalgae such as Haematococcus pluvialis, is commercially available as a food supplement in many countries [26]. Previous studies have demonstrated the effectiveness of astaxanthin in reducing inflammatory biomarkers and cytokines, as well as improving lipid profile levels [27, 28].
In a meta-analysis study conducted in 2015, Ersonia et al. investigated the impact of astaxanthin supplementation on lipid profile and glycemic markers. Seven studies involving 280 adult participants were evaluated, using a dosage of 4 to 20 mg over a study period of 4 weeks to 3 months. The results indicated that the supplementation did not affect the lipid profile, but did lead to a slight decrease in blood glucose levels [29].
In a meta-analysis conducted in 2020 by Xia et al., the impact of astaxanthin supplementation on obesity, blood pressure, lipid profile, and glycemic biomarkers was investigated. The study revealed that astaxanthin consumption led to an increase in HDL-C and a decrease in CRP (at doses higher than 12 mg), with no significant effect on other factors [30].
In a 2021 systematic review and meta-analysis conducted by Mokhtari et al., the impact of astaxanthin supplementation on blood pressure was investigated. The study evaluated 10 clinical trials with a total of 493 adult participants. The findings indicated that astaxanthin supplementation may lead to a reduction in diastolic blood pressure, particularly when administered at a dosage exceeding 12 mg per day in Asian individuals [22].
Another meta-analysis conducted in 2022 investigated the impact of astaxanthin supplementation on the health outcomes of adults at risk of metabolic syndrome. Seven studies involving 321 participants were assessed, and the results indicated that astaxanthin supplementation had marginal effects on reducing total cholesterol and systolic blood pressure, as well as significant effects on reducing LDL levels [31].
Based on a study conducted by Qarai et al. in 2022 involving 60 women with polycystic ovary syndrome, it was found that the administration of 8 mg of astaxanthin per day for 40 days resulted in an increase in the total antioxidant capacity compared to the placebo group. However, it did not have a significant effect on the levels of malondialdehyde and superoxide dismutase [32].
In a study by Rostami et al. in 2023, 50 infertile women with endometriosis were administered a daily dose of 6 mg of astaxanthin for a period of 12 weeks. The study’s findings revealed a significant increase in the total antioxidant capacity and superoxide dismutase, along with a significant decrease in malondialdehyde, interleukin-6, and TNF-α levels as a result of the supplement intake [33].
Hence, taking into account the positive impact of astaxanthin in decreasing oxidative stress and inflammation, and the limited research on the impact of astaxanthin supplementation on individuals with heart failure, we aim to examine the effects of astaxanthin supplementation on inflammatory markers, oxidative stress levels, lipid profile, uric acid levels, blood pressure, and endothelial function, as well as the quality of life and symptoms of heart failure in a double-blind randomized controlled clinical trial.
Objectives
Main aim: To assess the impact of astaxanthin supplementation on inflammatory markers, oxidative stress indices, lipid profile, uric acid level, blood pressure, endothelial function, quality of life, and disease symptoms in individuals with heart failure.
Primary objective: To evaluate the effect of 8-week astaxanthin consumption on levels of total antioxidant capacity (TAC) in individuals with heart failure.
Secondary objective: To evaluate the effect of 8-week astaxanthin consumption on variation in lipid profile (cholesterol, LDL-C, HDL-C, TG, AIP), oxidative stress levels (SOD, MDA, TAC), inflammatory markers (CRP, MCP-1, TNFα), uric acid levels, endothelial function (nitric oxide), quality of life and symptoms of heart failure (fatigue, loss of appetite, shortness of breath). Also to determine the impact of astaxanthin supplementation on the average alterations in anthropometric measurements (such as weight, BMI, and waist circumference) in individuals with heart failure pre- and post-intervention.
Trial design
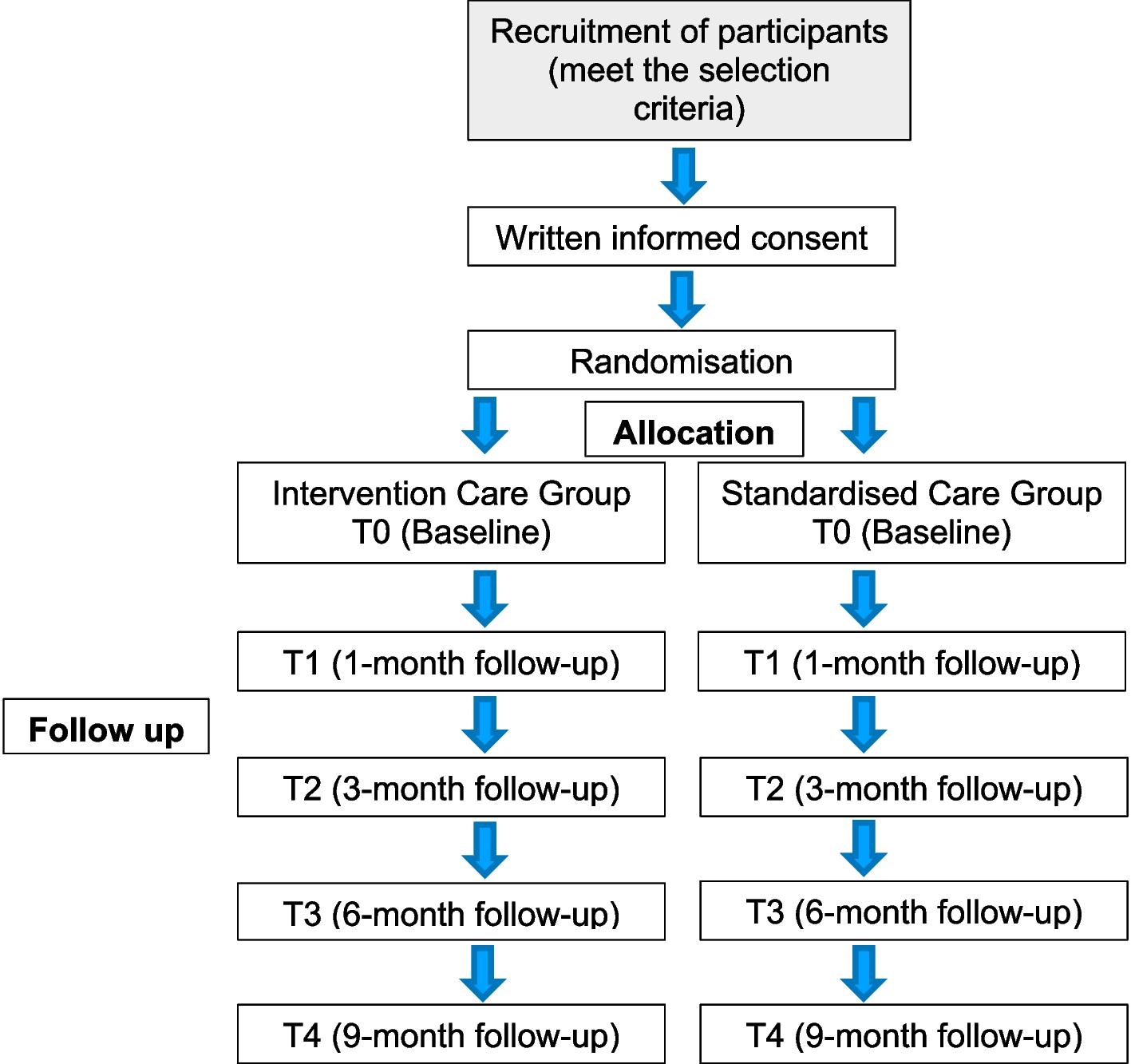
This is an 8-week, prospective, double-blinded, parallel assigned, randomized controlled clinical trial (RCT) in which subjects with heart failure will be randomized to an interventional (astaxanthin) or placebo group.



留言 (0)