
記住我




A clinical trial is designed to see the effect of the aerobic exercise protocol on neuropathic pain and QoL in persons with paraplegia.
Patient and study designA double-blind, parallel, two-group, and randomized controlled trial with equal subject allocation (1:1) will be undertaken. A convenient sample of 30 participants with paraplegia will be recruited from the inpatient and outpatient rehabilitation departments of the Indian Spinal Injuries Centre Hospital, New Delhi, India. All participants will be provided with information sheets, and written consent will be obtained by the principal investigator before recruitment. The demographic details will be obtained, and the participants will be selected based on the eligibility criteria after the neurological examination (Table 1).
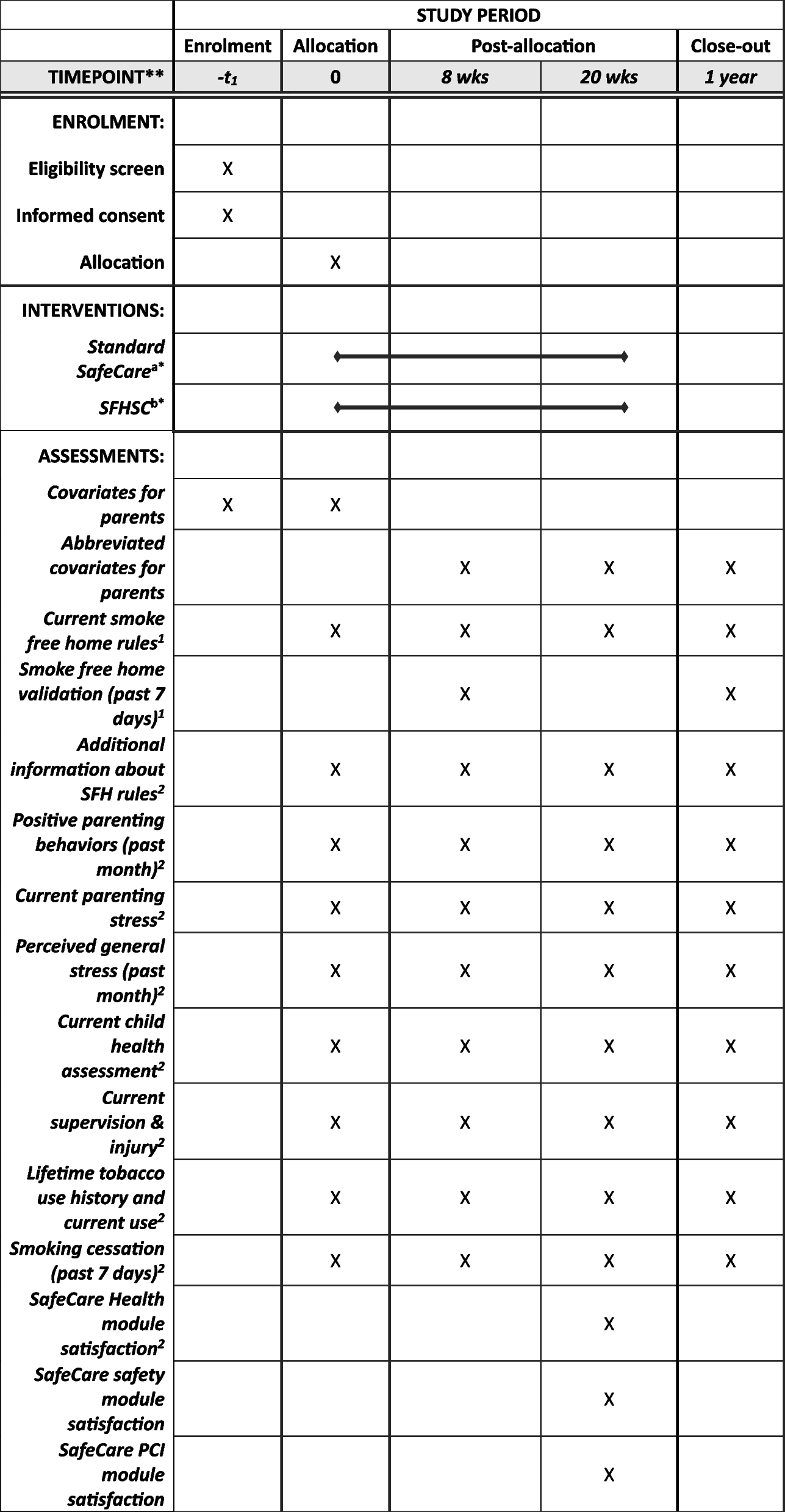
Table 1 Eligibility criteriaDRRC and RRC of the research department of the Indian Spinal Injuries Centre hold the legal liability and keep the check and record of all potential recruits and monitor the data collection throughout the intervention. The members of DRRC along with the consultants and physiotherapists in the hospital provide day-to-day support to all aspects of the local organization of the trial. The trial is supervised by the guides and co-guides twice a week. This research protocol is consistent with the current Consolidated Standards of Reporting Trials (CONSORT) guidelines (Fig. 1) and follows the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT schedule) (Table 2) [17] and is developed based on the SPIRIT checklist (Additional file 1). A visual description of the study regarding enrolment, assessments, and interventions is shown in Table 2. Baseline assessments (T0) will be done before group allocation. Mid-intervention assessments of both groups (T1) will be taken after the third week which will serve to compare the short-term effects of respective interventions delivered to the subjects. Post-intervention assessments of both groups (T2) will be done after 6 weeks of intervention to detect potential long-term effects.
Fig. 1
CONSORT (Consolidated Standards of Reporting Trials). HIIT + CT, high-intensity interval training along with conventional training; FHAA + CT, free hand arm aerobics along with conventional training
Table 2 Schedule of enrollment, interventions, and assessments according to the Standard Protocol Items: Recommendations for Interventional Trials guidelineEthical considerationsThe enrolled participants will be informed orally and in writing about the purpose of this trial, its potential risks, benefits of participation, and the right to withdraw from the trial at any point during the study. A written informed consent signed by the participants will be taken from those who are willing to participate in the study.
The data of the participants will be collected, documented, and managed confidentially using the paper-based entry data sets. Only all the authors related to the trial will have access to the final trial dataset. The masked datasets analyzed during the current study and statistical code will be available from the corresponding author upon reasonable request. The study protocol has been approved by the Institutional Ethical Committee and the trial is registered with Clinical Trials Registry.
RandomizationEligible individuals will be assigned randomly to either the Intervention or Control group. Randomization will be performed using a computer-generated randomization sequence generated by the Random Allocation Software, using a 1:1 allocation ratio.
To ensure concealment, the allocation sequence will be marked sequentially and sealed in opaque envelopes. An individual not associated with the study will sequentially open the numbered envelopes to reveal the participant’s group allocation. Based upon this, participants will be allocated to group A; intervention, or group B; the control group.
BlindingThe trial is a double-blinded study where the outcome assessor who will be a physiotherapist and participants will be blinded to group allocation. The principal investigator will be informed of the group allocation given the nature of the interventions. Also, the statistician who will perform data analysis would be unaware of the existence of treatment groups.
Exercise interventionThe planned protocol is reported in accordance with the Consensus on Exercise Reporting Template (CERT) checklist. In both groups, the intervention will be carried out individually along with conventional physiotherapy treatment, under the supervision and guidance of the physiotherapist for 30 min each day, 4 days a week for a total of 6 weeks. Special considerations of the American College of Sports Medicine (ACSM) for exercise prescription in spinal cord injury will be followed such as; participants will be asked to empty their urinary bladder before beginning of the exercise session [18]. To compensate for blood pooling, the participants will be required to wear stockings on the legs and abdominal binder during the intervention. Considering the enhanced thermoregulatory drive and lower sweat rates in persons with SCI the use of light clothing and maintaining proper hydration during the intervention will be ensured [19, 20].
The intervention will be divided into three phases for both groups (Table 3). Phase 1 will consist of a warm-up period. Participants will be asked to perform gentle upper extremity stretching exercises and low-intensity arm ergometer exercises at a rate of perceived exertion (RPE) between 2 (light) and 3 (moderate) for 5 to 10 min [11]. This will be followed by phase 2 of the aerobic training, i.e., in the intervention group HIIT will be performed which consists of 20 min of cycling with the arms using an arm ergometer (Thera Trainer) at high and low intensities during 60- and 60-s intervals, respectively, and to repeat this sequence 10 times over a period of 20 min. During the 60-s high-intensity interval, participants will be required to reach their 80- 90% HRpeak which will be achieved during aerobic exercise testing [21, 22]. Each high-intensity interval will be followed by a 60-s active recovery period at low intensity at an RPE between 1 (very light) and 2 (light) on the Borg CR10 scale.
Table 3 Description of exercise protocol with interventionThe active control group was designed to perform free hand-arm aerobic exercise consisting of five dynamic arm movements such as marching with arms, arm-swing side-to-side and front-to-back, and figure-of-eights mimicking kayak paddling [23]. Each movement will be performed for 1 min in a sequence and the whole sequence of these five movements will be repeated 4 times over a period of 20 min. These movements will be performed at low intensity guided by the metronome at 60 beats per minute [24].
In phase 3 of the training, there will be a 5–10-min cool-down period in the form of low-intensity arm ergometry at an RPE between 2 and 3 and gentle UE stretching resulting in a total exercise time of 30 min [11]. No rest will be provided during the session. Participants will be asked to wear an HR monitoring device (Samsung Galaxy Watch 4 Classic) on their wrist during the training to monitor their HR response in real-time. Adverse events will be monitored throughout.
Progression and feedbackTo account for changes in fitness and ensure progression, in the intervention group the intensity will be increased by 5% every 2 weeks (i.e., 80% HRpeak for weeks 1 and 2, 85% HRpeak for weeks 3 and 4, and 90% HRpeak for weeks 5 and 6) [22]. In the control group, the intensity will remain the same throughout without any progression. In the intervention group feedback on the heart rate and the time to change the intensity during the intervention will be given by the stopwatch placed in front of the patient and HR monitoring device. Whereas, in the control group the intensity will remain the same throughout the 6 weeks of the program. The participants will receive concomitant auditory feedback of intensity via metronome beats. Motivation will be provided by the therapist to achieve and maintain the targeted intensity.
Termination criteriaThe exercise will be terminated if any signs or symptoms of autonomic dysreflexia appear or if any kind of unusual uneasiness is reported by the participants. Protocol modification, if required will be done only after proposing the changes to the Research Review Committee and Internal Ethical Committee and after approval, the same will be notified to CTRI and the Journal. Any deviations from the protocol will be fully documented using a breach report form.
AdherenceThe adherence of the participants recruited in the study will be monitored by documenting the details of sessions attended, and the targeted intensity of the training protocol in different phases of intervention. As interval training elicits higher enjoyment, it keeps the person more engaged in the active intervention. Whereas, in the control group, matching the pace of the metronome to achieve the intensity and random order of the dynamic movements may positively influence the adherence and reduce attrition rates.
The participants will be permitted to increase the training duration by 1 week keeping in mind the “intention-to-treat” analysis principle if the participants are unable to complete the total number of sessions within the stipulated 6 weeks. Also, the type, extent, and pattern of missing data throughout the study will be fully reported by the authors.
Outcome variables 1.International Spinal Cord Injury Pain Basic Data Set Version 3.0: The International SCI Pain Basic Data Set (ISCIPBDS) standardizes the characterization and reporting of pain (primary outcome measure) and pain interference with day-to-day activities, overall mood, and sleep in persons with SCI by interviewing the participants [25]. It is based on the International SCI Pain Classification (ISCIP) which classifies pain based on its type (nociceptive, neuropathic, other, or unknown), subtype (nociceptive: musculoskeletal, visceral, or other), pain locations, intensity of pain on a numerical pain rating scale, frequency, and duration [26]. The ISCIPBDS has good validity and reliability as a self-reported measure of pain in individuals with SCI [27].
2.International SCI Quality of Life Data Set-Version 2.0: It is a tool to measure QoL in persons with SCI. It reflects subjective QoL based on each person utilizing his or her own personal perspective, internal standards, and assessment to assess his or her own QoL. It considers all factors that they feel contribute to or detract from their QoL, whether these are related to health, pain, family, finances, or any other domains of life. It has four questions in which participants provide a subjective rating of the past 4 weeks in four different domains related to QoL, i.e., general QoL (overall well-being), satisfaction with physical health, psychological health, and social life [21]. Each domain is ranked on a 0–10 scale, where 0 indicates complete dissatisfaction and 10 indicates complete satisfaction. Data will be collected by interviewing the participants. It has good internal construct validity [28].
3.6- Minute Push Test: Aerobic capacity will be evaluated using a 6-min push test (6-MPT). It is a reliable and valid measure for cardiorespiratory fitness testing in the SCI population (ICC > 0.90) [29]. The guidelines for conducting 6-MPT will follow the standardized American Thoracic Society guidelines and instructions for the administration of 6-MPT [30]. The test will be conducted along a flat corridor with clear space using a personal wheelchair at a 30-m loop course, marked 15 m apart by two cones with 2.8 m on either end to allow space for turning. The distance traveled in 6 min will be used to estimate the aerobic capacity of the individual. This is a valid and reliable measure of aerobic capacity in persons with SCI [29].
Sample sizeA priori sample size estimation was done using the statistical formula by considering pain intensity as the primary outcome measure. It is based on an expected drop-out of ∼15%. The total sample size was calculated at 28 by using an α level of 0.05, a power of 80%, and a calculated medium effect size of 0.67 at 95% CI. It was increased to 30 on a suggestion from the ethical committee.
Statistical analysisTo check for selection bias, we will apply Pearson’s chi-square test for categorical variables and Student’s t-test for numerical variables. This will be performed to know if the randomization process generated between each group of participants has homogenous clinical and demographic characteristics before the intervention.
Continuous variables will be summarized as mean ± standard deviation for normal distribution and median ± interquartile range for non-normal distribution. The Shapiro–Wilk test will be used to know the normality of data. In the case of normal distribution of data, we will analyze the intergroup comparison by applying a two-sample t-test. In case of skewed data, we will use the Mann–Whitney U test for the intergroup comparison. The intragroup comparison will be analyzed by Repeated measure ANOVA or Friedman’s test (if data is not normally distributed). The final statistical analysis will be performed using IBM SPSS ver. 21.0 (IBM Corp., Armonk, NY, USA). This will be done based on the modified intention-to-treat principle, whereby each participant must complete > 75% (18 of 24 sessions) of planned exercise sessions. The principle of the “last observation carried forward” shall be applied in case of missing data of dropped-out individuals. This means that the missing final values of the outcome variable will be replaced by the last known value. The level of statistical significance is assumed at p-value < 0.05.
留言 (0)