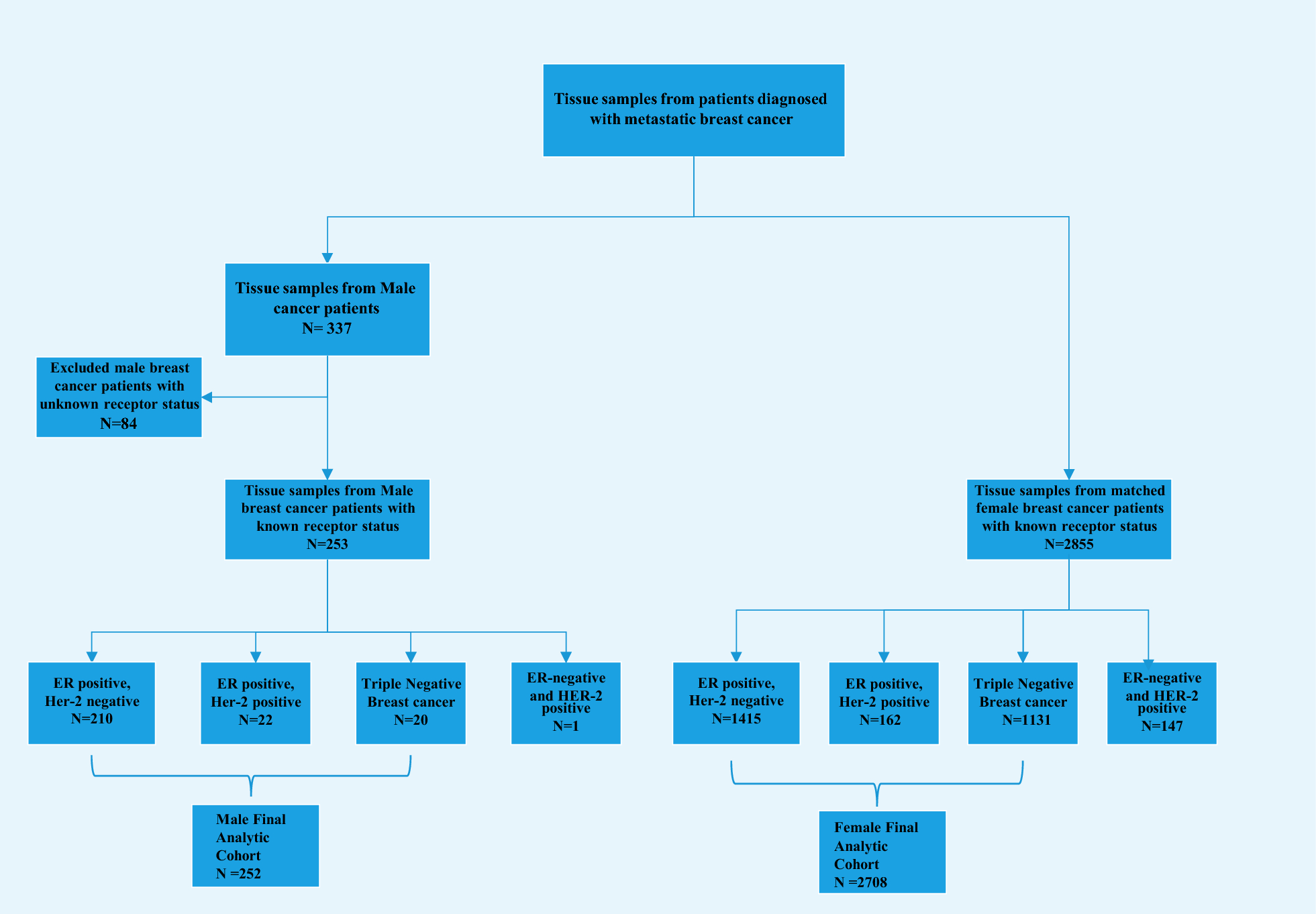
In this study, we evaluated a series of 252 MaBC samples that underwent next-generation sequencing using Foundation Medicine and compared the genomic profiling with a FBC cohort of 2708 cases from the same source, stratified by molecular subtype. While there were genomic similarities between male and female breast cancers, our study showed important genomic differences between the two sexes.
Men with ER-positive/HER2-negative breast cancer had more frequent alterations in GATA3, MDM2, CDK4, BRCA2 genes as compared with FBC patients of the same subtype. GATA3 is a defining marker for luminal cancers and an important regulator of luminal differentiation [14, 15]. Mutations in GATA3 have been associated with changes in luminal biology endocrine resistance, and worse prognosis [16].
The presence of alterations in BRCA2 in MaBC provides opportunity for targeted therapy with PARP inhibitors. As compared with women, men in our study with ER-positive/HER2-negative breast cancer were also found to have fewer alterations in TP53 and ESR1 genes. While intriguing, the lower frequency of TP53 in men compared with women and the higher frequency of MDM2 in men compared with women may represent true biologic differences between male and female breast cancer tumor biology. In fact, alterations in TP53 and MDM2 are nearly mutually exclusive events and suggest different biological pathways to p53 inactivation. The lower incidence of ESR1 mutations in men is suggestive of lower rates in use of aromatase inhibitors as compared with women.
When comparing patients with ER-positive/HER2-positive breast cancer, male patients had higher alterations in ERBB2, PIK3CA, GATA3, and MDM2 genes while female patients had higher alterations in TP53 genes. Mutations in ERBB2 and PIK3CA are associated with resistance to anti-HER2 therapies [17,18,19,20,21].
Two prior studies have shown that, as compared with women, men with HER2-positive breast cancer have worse survival [5, 22]. A recent analysis of National Cancer Database showed that men with HER2-positive breast cancer have 60% lower odds of achieving pathologic complete response to neoadjuvant chemotherapy compared with women of the same subtype [23, 24]. Taken together, the data from the aforementioned manuscripts show that HER2-positive breast cancer in men appears to have worse prognosis than in women. Our current study suggests that the differences in prognosis may be related to genomic alterations that confer resistance to anti-HER2 therapy, such as ERBB2 short variants and PIK3CA alterations, both of which are associated with therapy resistance and poor prognosis. Interestingly, our study showed that the median ERBB2 copy number in MaBC is significantly lower than in FBC, highlighting additional molecular differences in HER2-positive breast cancer between males and females which may impact sensitivity to anti-HER2 therapy. It is possible that HER2-positive MaBC may be less HER2 addicted than HER2-positive FBC.
Among patients with TNBC, a higher frequency of alterations in the BRCA2 gene was observed in male patients. We also observed a significantly higher frequency of alterations in TP53 in female patients when compared to male patients. BRCA2 has a critical role in DNA repair, and mutations in BRCA2 are a known risk factor for the development of breast cancer in men.3 Two pivotal trials demonstrated the role of PARP inhibitors in the treatment of BRCA-mutated metastatic breast cancer [25, 26]. Our results suggest that alterations in BRCA2 are very prevalent in MaBC and raise the possibility of using PARP inhibitors in this population.
As observed in our study, there are important genomic differences between MaBC and FBC. One possible explanation for the different genomic alteration frequencies may be differences in intrinsic subtypes between sexes. In fact, analysis of genomic intrinsic subtypes in male breast cancer has shown a predominant luminal disease, with higher frequency of luminal B tumors and lower frequency of HER2 enriched and basal-like tumors [27].
Our study revealed a considerable number of men with breast CSG alterations (22.6%), which was significantly higher than in women (14.6%). Similarly, BRCA mutations were more frequent in men than in women. This represents a significant opportunity for targeted therapy with PARP inhibitors. The phase III EMBRACA trial (25) and Olympiad trial (26) showed improvements in progression-free survival in BRCA 1/2-mutated HER2-negative population. Notably, there were only 5 men in the treatment arm of the Olympiad trial, and 2 in the trial’s standard therapy group. Similarly, men in the EMBRACA trial represented less than 2% of the study population. As expected, we observed that BRCA2 was the predominant alteration in men, consistent with prior studies [28,29,30,31]. To our knowledge, our study represents the largest analysis of breast cancer susceptibility genes in MaBC to date.
Our study had some important limitations. The first is that the study is retrospective. Secondly, we do not have patients’ clinical information including some demographics, treatment, and clinical outcomes. Some alteration frequencies reported may be impacted by the sample used for sequencing, as the mutational spectrum can change over time; in this regard, while the tissue sources are described in Additional file 1: Figure S1, the lines of therapy that patients received before sample acquisition are unknown. This is an important limitation considering that prior treatment may alter alteration frequencies. Given the lack of information on some patient characteristics and prior treatments, there may be unmeasured differences between the male and female cohorts. The sample size of HER2-positive and triple-negative MaBC was small, and we had to exclude the one case that was ER-negative/HER2-positive. This underrepresentation is expected owing to the rarity of these subtypes in men [32]; nonetheless, caution should be taken when interpreting the results from these smaller subgroups. Unfortunately, data on HER2-low classification was not available for the FBC cohort and thus prevents comparisons with the findings of the MaBC cohort. Additionally, our study lacked matched normal tissue to help determine whether aberrations are germline or somatic, and lacked information on variant allele frequencies. Finally, given that we are reporting on cases that were specifically submitted for genomic analysis, our study has a selection bias and the study population may not be representative of the overall population of men with breast cancer. To address this issue, we used a female cohort with the same inclusion criteria and from the same source, likely sharing the same degree of selection bias in the control group.
Despite these limitations, there are several important strengths to our study. To our knowledge, this is the largest reported cohort of MaBC undergoing genomic analysis. In addition, we have included a comprehensive approach consisting of extensive genomic characterization with a high number of genes, including breast CSGs, which if confirmed as germline can have additional impact on these patients and their families. We compared genomic alterations between male and female by molecular subtype, which provides subtype-specific information that is clinically more relevant. Our study results provide important information about clinically actionable alterations in MaBC with regards to somatic mutations, as well as breast CSGs.




留言 (0)