
記住我


Data retained by the author for patients with idiopathic constipation who were referred to our pediatric surgical facility during the period from 2013 to 2023 were retrospectively analyzed. The study included patients with significant symptoms of constipation and in whom we suspected a minor degree of unrecognized anterior anal misplacement. The criteria (inclusion and exclusion criteria) to select such cases with debatable diagnoses can be summarized in the following points:
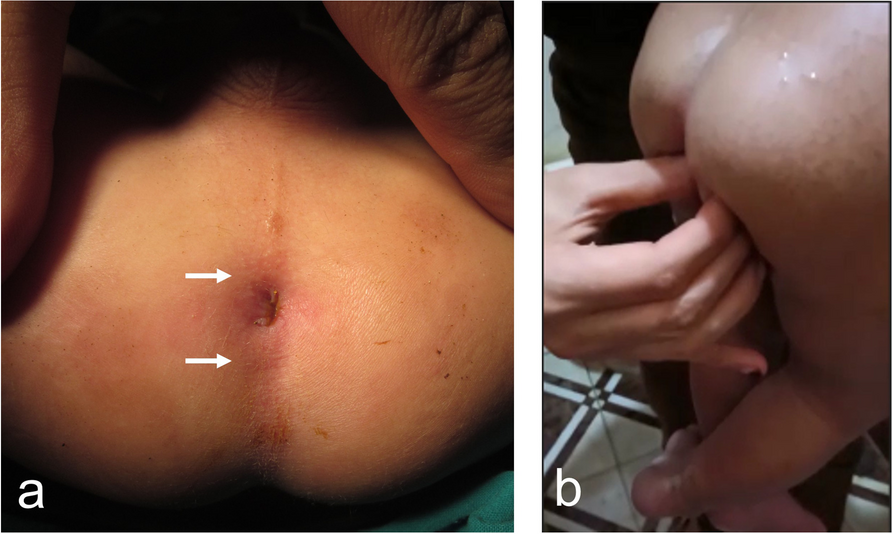
First, the history of constipation in these children was usually dated since early infancy being more pronounced after the start of weaning. Remarkably, almost all cases passed stools with severe straining whatever the frequency of defecation (sometimes up to every 5–10 days); otherwise, they were healthy children. Some parents reported that they used to press on the perineum of their children behind or at both sides of the anus to facilitate the extrusion of feces through the anus (Fig. 1).
Fig. 1
Fifteen-month-old boy presenting with constipation characterized by severe straining at defecation not responding to medical treatment. a Photograph of the perineum in the supine lithotomy position: the anus was not perfectly in the middle, but slightly anteriorly displaced with no evidence of stenosis. White arrows mark the anterior and posterior boundaries of the perianal pigmented skin. b Photograph sent by the mother to demonstrate how she facilitates the extrusion of stools by squeezing on the perineum at both sides of the anus
Second, on examination, the anus looked ‘more or less’ normal with no evidence of stenosis. However, in females (majority of cases), the perineum looked shorter than usual (Fig. 2). With more careful examination, one can notice the peri-anal pigmented skin is not evenly distributed around the anus. In other words, the anus was not perfectly in the middle but slightly anteriorly displaced (eccentric), which may still be considered normal by many of the attending pediatric surgical colleagues due to the absence of stenosis. Occasionally, an anterior anal fissure was noticed at the 12 o’clock position (Fig. 2).
Fig. 2
Eight-month-old girl presenting with constipation characterized by severe straining at defecation. Photograph of the perineum in the supine lithotomy position: notice the peri-anal pigmented skin is not evenly distributed around the anus (dotted yellow circle); the anus is not perfectly in the middle but slightly anteriorly displaced with no evidence of stenosis. Note the presence of an anal fissure at the 12 o’clock position
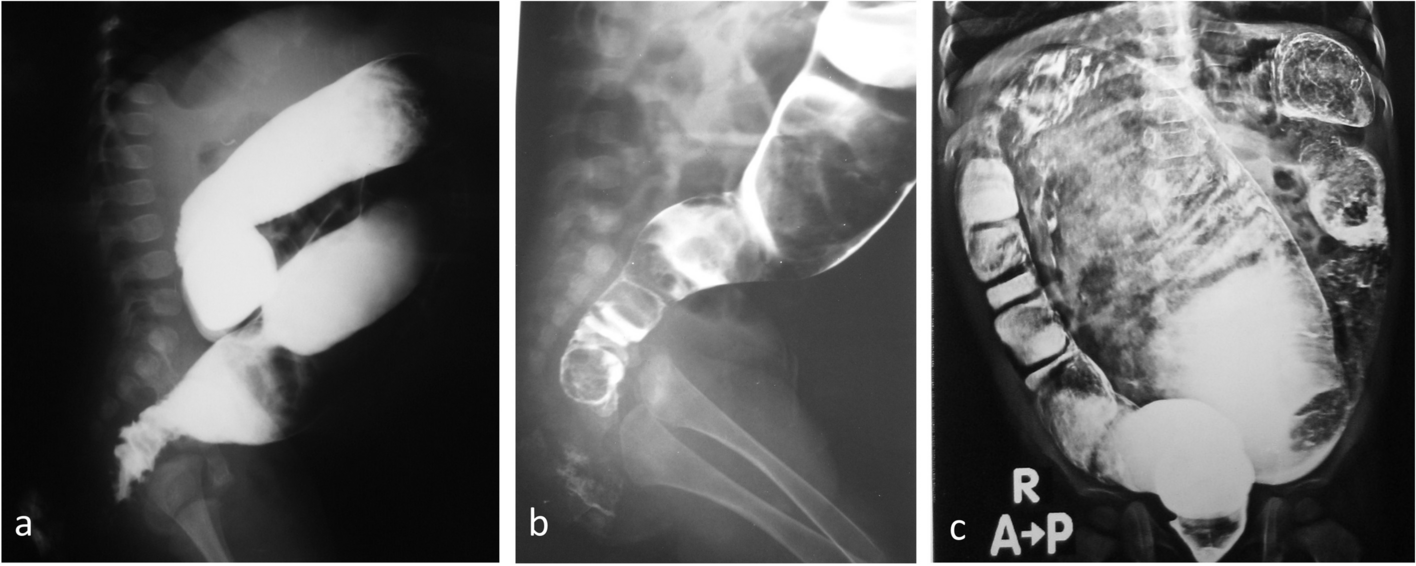
Third, it was important to exclude the possibility of Hirschsprung disease in these patients. The typical history of Hirschsprung disease includes delayed passage of meconium in addition to significant abdominal distension which is considered the red flag for diagnosing Hirschsprung disease. Failure to thrive and enterocolitis are another two important associations with Hirschsprung disease. Cases included in the study lacked this typical history and associations. In addition, their contrast enema demonstrated a normal/dilated rectum down to the anal canal usually with prominent posterior shelving (Fig. 3). In doubtful situations, a rectal biopsy was performed that confirmed the presence of ganglion cells. In some cases, rectal biopsies were already taken before referral, which excluded Hirschsprung disease.
Fig. 3
Contrast enema demonstrating normal rectum down to the anal canal with prominent posterior shelving (arrow)
Fourth, to support the subtle external deviations, pelvic MRI studies were ordered in most cases searching for possible deviations from the norm at a deeper level. Findings were related to our previous experience comparing pelvic MRI anatomy in cases of anorectal anomalies and controls [6, 7]. Interestingly, we could detect deviations similar to those found in mild forms of anorectal anomalies (rectoperineal fistula) [8]. These mild deviations from the norm were more pronounced at the level of the mid-anal canal rather than distally. The mid-anal canal appeared elongated (Fig. 4), hanging forwards, and anteriorly displaced in relation to bony and soft tissue landmarks: ischial tuberosities (Fig. 5), and transverse perineal muscles (Fig. 6).
Fig. 4
Deep pelvic anatomical deviations in cases with mild anterior anal misplacement as demonstrated in their pelvic MRI studies compared to normal control (a). a Mid sagittal pelvic MRI (T2WI) in 5-year-old girl (normal control). b, c Eight-month-old and 2-year-old girls with mild anterior anal misplacement presenting with severe constipation. d, e Mid sagittal pelvic MRI (T2WI) of the above two cases (b and c, respectively). P: pubic symphysis; UB: urinary bladder; R: rectum; thick black arrow points to the site of the anus. Note the elongated anal canal in d and e compared to control (a); a double arrowhead dotted line is used to mark the distance from a fixed bony landmark, the pubic symphysis (P)
Fig. 5
One-year-old girl with mild anterior anal misplacement presenting with severe constipation. a Photograph of the perineum in the supine lithotomy position: the anus was not perfectly in the middle, but slightly anteriorly displaced with no evidence of stenosis. Arrows are marking for the anterior and posterior boundaries of the perianal pigmented skin. b, c Pelvic MRI study mid-sagittal, and axial (at the level of ischial tuberosities), respectively, demonstrating deep pelvic anatomical deviations. P: pubic symphysis; UB: urinary bladder; R: rectum; An: anus; Vs: vestibule; Cl: clitoris; i: ischial tuberosity. Note the distended rectum (R) and elongated mid portion of the anal canal in b. Also, note the anterior displacement of the anal canal (An) in c, which should be normally located at the level of an imaginary line joining both ischial tuberosities (i)
Fig. 6
Seven-month-old girl with mild anterior anal misplacement. a Axial pelvic MRI (T2WI) at the level of the distal anal canal with color-overlay in b. Note the anal canal (yellow circle) is displaced anteriorly separating the transverse perineal muscles (red arrows) on both sides
By collecting the above pieces of evidence, and most importantly, in the presence of the characteristic complaint of severe straining during defecation (indicating some sort of mechanical obstruction), we offered these cases surgery in the form of posterior anoplasty [3].
Surgical technique (posterior anoplasty)The patient is placed in the supine lithotomy position (Fig. 7a). A posterior circum-anal incision is made from the 3 o’clock to the 9 o’clock position. The incision is deepened by dissection on the posterior and lateral aspects of the anal canal; this step is facilitated by outward retraction of the anus (Fig. 7b). The posterior traversing subcutaneous sphincteric muscle fibers are identified deep in the wound, which are incised in the midline (posterior myotomy). The skin incision is then closed (Fig. 7c). More recently, we modified the procedure to be performed in a simpler yet similar way (Fig. 8). A vertical midline “cutback” incision (about 1 cm) is made in the posterior wall of the anal canal and nearby skin (at the 6 o’clock ‘position) (Fig. 8a). The posterior extension of this vertical ‘cutback’ incision is limited by the boundaries of the modified (pigmented) perianal skin. Deep in the wound, the posterior traversing muscle fibers are identified and incised in the midline (posterior myotomy) (Fig. 8e). The vertical mucocutaneous incision is then closed in a horizontal fashion. Puckering of the skin/mucous membrane at the edges of the wound may need to be trimmed (Fig. 8).
Fig. 7
Surgical technique of the posterior anoplasty. a The patient is placed in the supine lithotomy position. b A posterior circum-anal incision is made from the 3 o’clock to the 9 o’clock position. c After performing the posterior myotomy, the skin incision is then closed
Fig. 8
Surgical technique of the cutback anoplasty. a The patient is placed in the supine lithotomy position. b Traction sutures at the 5 and 7 o’clock positions. c, and d A vertical midline “cutback” incision (about 1 cm) is made in the posterior wall of the anal canal and nearby skin (at the 6 o’clock ‘position). e Deep in the wound, the posterior traversing muscle fibers are identified and incised in the midline (posterior myotomy). f The vertical mucocutaneous incision is then closed in a horizontal fashion
Postoperative careEnteral feeding is resumed on the same day upon full recovery, and the patient is discharged home the next day on analgesics. No need for prophylactic antibiotics apart from a single dose given at induction of anesthesia. Laxatives are usually prescribed on the third postoperative day and continued for 2–3 weeks as needed.
Follow-upThe first follow-up visit was scheduled 7 days postoperatively to inspect for possible wound complications. As the incision was not involving the whole anal circumference, postoperative anal dilatation was not required. The second visit was 4 weeks later to ask about symptoms of constipation (straining), frequency of defecation, and whether there was a need to continue on laxatives. Messages were sent to parents of operated cases through their registered phone numbers to ask about longer-term follow-up.
留言 (0)