Monitoring the incidence, prognosis, and development of NS requires robust methods while considering the evolving clinical definitions of sepsis [6]. There is currently no international consensus for defining NS. In 2016, the Journal of the American Medical Association named this disease ‘SEPSIS-3’, which is a life-threatening disease characterized by the host’s dysregulated response to infection and consequent organ dysfunction [7]. NS diagnosis is divided into three categories: suspected diagnosis, clinical diagnosis, and definite diagnosis [4]. Given that newborns are the most susceptible to sepsis, it is necessary to understand the associated risk and etiological factors for better NS management.
The neonatal immune system is vulnerable due to characteristics including decreased cellular activity, underdeveloped complement systems, preferential anti-inflammatory responses, and insufficient pathogenic memory [8]. Neonatal susceptibility is caused by an immature immune system, maternal infection, adverse environment, and other risk factors. Additionally, studies have shown that the IL-1β rs1143643 G > A gene polymorphism is related to the incidence of NS [9]. Researchers have suggested that NS increases the risk of neurodevelopmental disorders in premature infants [10]. Given that an early diagnosis of NS can improve prognosis, it is critical to identify novel biomarkers for NS. As biomarkers of neonatal sepsis, the most commonly used laboratory parameters include whole blood cell count, C-reactive protein, and procalcitonin, all of which have significant limitations in sensitivity and specificity. Other serum biomarkers, including interleukin-6, presepsin, cluster of differentiation (CD) 64, CD11b, serum amyloid A, S100 protein A12, lipopolysaccharide-binding protein, volatile organic compounds, and soluble triggering receptor expressed on myeloid cell-1, have also been used for the identification of neonatal sepsis [11]. Expert studies have found that CRP levels are associated with bacteremia, fungemia, and viremia detected by blood mNGS [12]. In this study, we found that the total number of WBCs or CRP in the vast majority of NGS-positive newborns with NS were elevated. Progranulin is a promising biomarker for the diagnosis of EOS, as its use combined with the detection of procalcitonin can improve the diagnosis of sepsis [13]. Studies have shown that although blood culture results are similar to PCR results in EOS, the positivity rate of PCR is significantly higher than that of blood culture, with 16S rRNA PCR showing higher sensitivity and allowing for a rapid and accurate diagnosis [14].
Blood culture is the most suitable method for antimicrobial susceptibility testing [14]. İstanbullu et al. point out that the 16S rRNA genes of all suspected microorganisms should be subjected to real-time PCR detection to improve the diagnostic sensitivity of NS [15]. In the current study, we amplified the 16S rRNA gene and ITS sequence in patient samples to construct gene libraries and performed high-throughput NGS analysis, covering the genes of prokaryotic and eukaryotic microorganisms, and neither viruses nor fungi were detected. Akbarian-Rad et al. found that NS is highly prevalent in patients suspected of having NS, indicating the importance of taking preventive measures, conducting routine evaluation, and closely monitoring newborns [16]. Zhou et al. found through a retrospective study that the detection rate of pathogenic microorganisms in blood mNGS was significantly higher than that of pathogens in blood culture. Among all the positive bacterial and fungal detection results, only 12.00% of blood mNGS were consistent with blood culture, suggesting that mNGS could not completely replace blood culture in patients with suspected blood infection [12]. Herein, among the patients clinically diagnosed with NS, 44% were definitively diagnosed using high-throughput NGS. The discrepancy between the clinical diagnosis and final diagnosis in traditional bacterial culture methods indicates that this method alone cannot be used to confirm a suspected diagnosis or clinical diagnosis of NS; thus, other effective and practical diagnostic techniques must be used.
The pathogens responsible for NS vary worldwide; the most common pathogens in developing countries are gram-negative bacteria, including Acinetobacter spp., Klebsiella spp., and Escherichia coli. Bacterial culture-based studies have confirmed that Streptococcus pneumoniae is the most common pathogen responsible for NS in South China [17]. S. pneumoniae is primarily associated with LOS in premature infants, whereas group B Streptococcus is the main EOS pathogen. E. coli is common in both LOS and EOS and leads to the highest mortality rate [18]. El-Amir et al. reported that EOS is primarily caused by E. coli, whereas LOS is caused by Staphylococcus aureus [14]. Margaret et al. found that group B streptococci and E. coli were the most common in EOS, while coagulase-negative Staphylococcus was the main cause of LOS [8]. The herpes simplex virus may also cause potentially devastating infections in newborns [19]. Gao et al. found that the positivity rate of gram-negative bacteria in NS exceeds that of gram-positive bacteria and fungi, and that the four most dominant bacterial pathogens in NS are E. coli (21.9%), Klebsiella pneumoniae (21.9%), group B Streptococcus (13.2%), and S. aureus (6.8%). Enterobacter spp. and K. pneumoniae are considered the main bacterial pathogens responsible for NS in Iran. Moreover, 22.9% of Enterobacter spp. responsible for NS are extended-spectrum beta-lactamase-producing bacteria [20]. Extended-spectrum beta-lactamase-producing multidrug-resistant E. coli have emerged as the main pathogens responsible for early NS, particularly in premature infants [21]. Common bacterial pathogens responsible for sepsis in surgery are Enterococcus faecalis, S. aureus, K. pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter spp., which are similar to the common bacterial pathogens in NS [22].
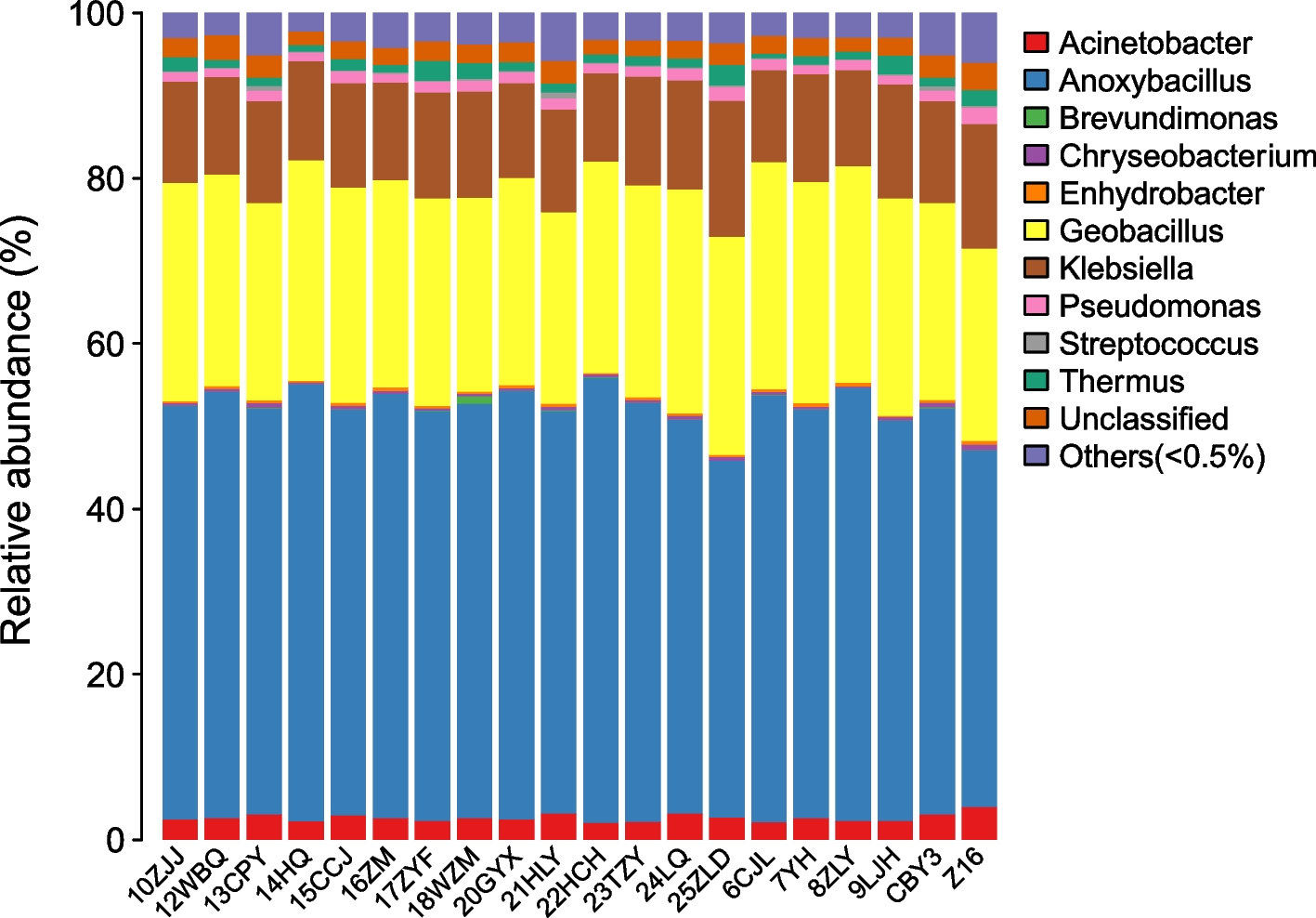
The bacterial species detected in this study included Streptococcus spp. and Pseudomonas spp. However, the number of OTUs belonging to these two genera was relatively small, thus excluding them as the main candidate bacterial pathogens. In samples from subjects clinically diagnosed with NS and who later received a definite diagnosis, after excluding contaminating bacteria associated with a small number of OTUs, A. kestanbolensis, G. vulcani, K. oxytoca, and A. guillouiae were found to co-exist, suggesting coinfections maybe with multiple bacterial species in NS. We observed that Anoxybacillus kestanbolensis was associated with the largest number of OTUs in the 20 clinically confirmed NS samples, followed by G. vulcani; both species are gram-positive bacilli. Klebsiella oxytoca and A. guillouiae, associated with a slightly smaller number of OTUs, are gram-negative bacilli. These bacteria could not be cultivated using traditional bacterial culture methods; therefore, to verify the NGS results, we performed PCR amplification using specific primers followed by Sanger sequencing. These results of NGS were consistent with these findings.
The primary drugs used to treat patients with NGS-positive NS in the present study were latamoxef, ceftazidime, ceftriaxone, and penicillin (see Additional file 2), and subjects were hospitalized for an average of 5 days prior to discharge following symptom improvement, which was shorter than the 12.3 day treatment time reported by Wagstaff et al. for EOS patients [23], and the patient’s prognosis was good, indicating a high cure rate for NS caused by these four bacteria. In contrast, 25 unconfirmed cases of NS were empirically treated with third-generation cephalosporin antibiotics and discharged after 3–7 days with symptom improvement. Latamoxef is a member of the oxacephem family and has an antibacterial spectrum similar to third-generation cephalosporin antibiotics (ceftazidime and ceftriaxone). These drugs can treat single or multiple pathogenic infections, with antibacterial activity against both gram-positive and gram-negative pathogens. Penicillin is efficacious in the treatment of infection-induced bacteraemia and sepsis.
The underlying diseases for NS in this study were primarily neonatal infectious pneumonia, neonatal hyperbilirubinemia, and neonatal meconium aspiration syndrome, all of which are common in newborns. Some patients with NS presented with double infections or multiple cross-infections. Although patients presented with different types of underlying diseases, four main bacteria, namely, A. kestanbolensis, G. vulcani, K. oxytoca, and A. guillouiae, were commonly identified. These bacteria were also identified in our previous study on male and female urogenital diseases and are commonly present in the genitourinary tracts of men and women [5]. Thus, these bacteria can enter the foetal blood circulation through the foetal skin, oral cavity, or respiratory mucosa during intrauterine infection or delivery owing to the compression of the birth canal or other reasons. These four kinds of bacteria may temporarily enter the blood; however, with no way to isolate and grow these bacteria, further study is required to determine whether they cause NS.
Radchenkova et al. [24] isolated A. kestanbolensis from Bulgarian hot springs. Dulger et al. [25] isolated A. kestanbolensis sp. nov. from the mud and water samples of Turkish hot springs, but this bacterium has not been isolated in humans, nor has it been reported as related to human diseases. Sürmeli et al. [26] reported that α-L-arabinofuranosidase subjected to directed evolution and cultivation using G. vulcani GS90 exhibits improved activity, such as higher thermal stability but lower alkaline stability. Reportedly, the above-mentioned two gram-positive bacilli show high-temperature resistance, are difficult to isolate and culture at 37 °C, and have high nutritional requirements. Few reports are available on G. vulcani. Nazina et al. [27] isolated a new type of thermophilic spore-forming strain, GaT, from hot springs in northern Russia and found that this strain is genetically and phenotypically different from the known Geobacillus strain. Although K. oxytoca and A. guillouiae in the present China-based study belong to the same genera as K. pneumoniae and A. baumannii reported in other countries, some interspecies differences do exist.



留言 (0)