Data Source
This study was conducted using data from the Flatiron Health US-based nationwide database of deidentified electronic health record (EHR)-derived data from approximately 280 cancer clinics representing an estimated 800 sites of care [11, 12]. The database contains patient-level structured and unstructured data, curated via technology-enabled abstraction from physician notes and other unstructured documents. For this study, data were custom curated to capture all patients treated with niraparib from the overall OC population available in the database, using the data cutoff of 30 November 2022. The deidentified data were subject to obligations to prevent reidentification and protect patient confidentiality.
Study Population
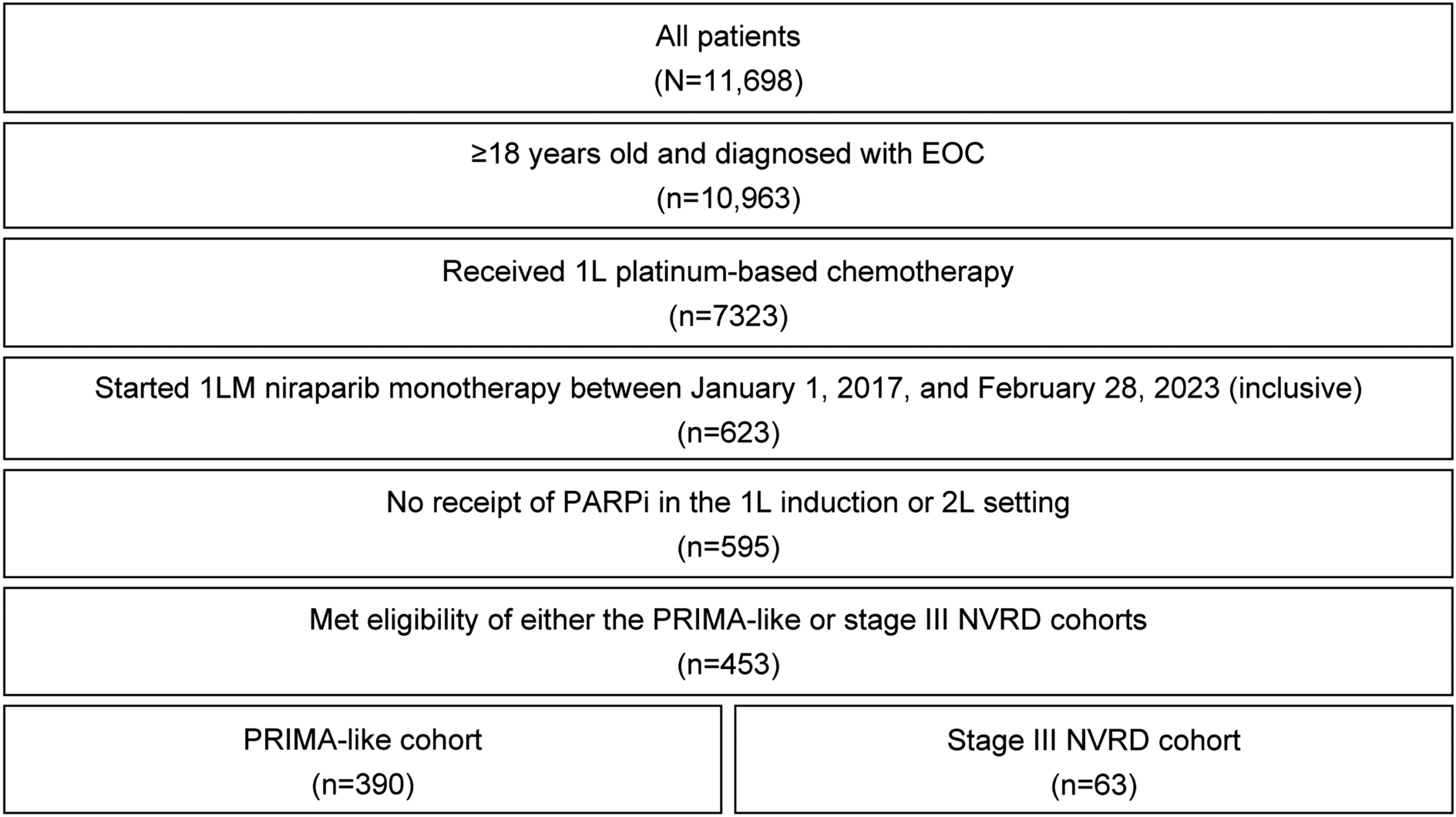
Patients diagnosed with OC during the study period (1 January 2011 to 30 November 2022) were eligible if they received 1L combination chemotherapy plus bevacizumab followed by 1LM niraparib monotherapy. Initiation of 1LM niraparib monotherapy must have occurred between 1 January 2017 and 2 September 2022. Patients were required to be at least 18 years of age at initial OC diagnosis, have evidence of epithelial histology (serous, clear cell, mucinous, endometrioid, transitional cell, epithelial not otherwise specified, or unknown), and have at least 1 day of follow-up after the index date (defined as the date of initiation of 1LM niraparib monotherapy). Patients were excluded if they were likely to have a misclassified line of therapy, defined as having a record of receiving 1L or second-line (2L) PARP inhibitor monotherapy. Lines of therapy were defined with a prespecified database-specific, rules-based, oncologist-defined line-of-therapy algorithm. Patients were followed from index date until the first occurrence of death, end of follow-up, or end of study (30 November 2022).
Study Outcomes
Patient demographics and clinical characteristics were collected from the index date or within the baseline period, defined as the time between initial OC diagnosis and index date. Specifically, age, geographic region, race, ethnicity, and practice type were collected. Clinical characteristics included year of initial OC diagnosis, year of end of 1L therapy, duration of 1L therapy, prior primary or interval cytoreductive surgery, residual disease status, height, weight, blood pressure, hypertension, platelet count, biomarker status, Eastern Cooperative Oncology Group performance status score, histology at OC diagnosis, and stage at initial diagnosis. Dosing characteristics for 1LM niraparib monotherapy included starting daily dose, occurrence and type of dose modifications, occurrence of dose discontinuation, and reason(s) for discontinuation.
Individualized starting dose (ISD) was determined based on the patient’s weight and platelet count (closest to index date, from 28 days prior to the last date of 1L induction treatment up to index date). Patients weighing < 77 kg or with a platelet count of < 150,000/µL were indicated for a 200-mg starting dose. Patients weighing ≥ 77 kg and with platelet count ≥ 150,000/µL were indicated for a 300-mg starting dose. Starting dose status was a categorical variable defined as ISD (a patient started at the dose indicated by ISD calculation), received a dose lower than ISD (e.g., indicated for 300 mg but had a starting dose of 200 mg or 100 mg), or received a dose higher than ISD (e.g., indicated for 200 mg but had a starting dose of 300 mg); patients with missing data for any of these variables had their starting dose status classified as “other or unknown.”
Real-world clinical outcomes of interest included time to treatment discontinuation (TTD) of niraparib and TTNT. TTD was measured as the time from start of 1LM niraparib monotherapy to the date of 1LM niraparib monotherapy discontinuation; patients who did not discontinue their maintenance therapy were censored at the last drug episode. TTNT, a proxy for real-world PFS, was measured from the end date of 1L therapy until the earliest of 2L initiation or death; patients who did not initiate subsequent treatment or die were censored at the last clinical activity or end of the study period.
Statistical Methods
Patient baseline characteristics were summarized descriptively for the overall study population. Kaplan–Meier curves were used to describe median TTD and TTNT (in months) and associated 95% CIs.
Ethical Approval
This study complied with all applicable patient privacy laws. The deidentified data were subject to obligations to prevent reidentification and protect patient confidentiality. There was no direct patient contact or primary collection of individual human participant data. Study results and analyses omit patient identification. Therefore, informed consent and ethics committee or institutional review board approval were not required. The data that support the findings of this study have been originated by Flatiron Health, Inc, and we have permission to use the data.






留言 (0)