
記住我

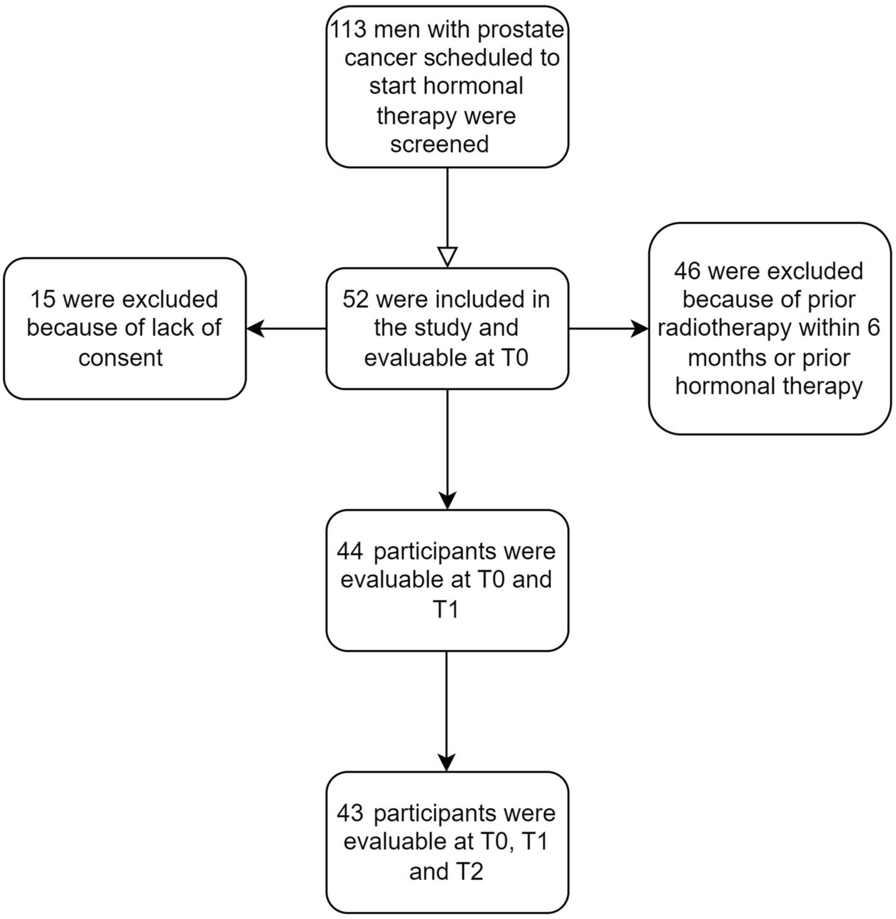

These analyses are based on responses to the “International Survey to Elicit the Burden of Illness of Idiopathic Multicentric Castleman Disease—Patient Survey” [3], and permission for use of this data has been granted by the funder and the researchers. The online survey conducted between 14 April 2021 and 8 November 2021 was administered to patients with iMCD registered with the Castleman Disease Collaborative Network (CDCN), a USA-based organization which, among other objectives, aims to support patients with Castleman Disease (CD) worldwide. This survey included patients registered with the CDCN and residing in Australia, Canada, UK, and USA (see Fig. 1). Patients were recruited via the CDCN using a variety of methods including postings on the CDCN website, communication via the CDCN social media (Facebook), and direct mailing to CDCN patient-members. There were no specific recruiting sites or investigators involved in direct recruitment in any of the countries. This was a non-targeted dissemination of the survey through CDCN and recruitment was primarily based on voluntary participation of the patients and caregivers provided they met the eligibility criteria and signed the consent form. In preparing to conduct the Symptom Burden Study, a non-therapeutic, non-interventional online survey, the researchers followed advice and guidance on ethics approval from each country where it was anticipated that the participants would reside. We undertook this research following the WMA Declaration of Helsinki. All patients were recruited from the Castleman Disease Collborative Network (CDCN, based in the USA) via communication to their members, who reside all over the world. The advertisement of this survey was limited to CDCN members only, irrespective of their resident country, but the participation was limited to four English-speaking countries. These countries were Australia, Canada, the UK, and the USA given similarities in the consent and approval process, proportional representation of patients with iMCD from these countries in the CDCN, and the likelihood of recruiting an adequate number of respondents. Approval was granted by the following Ethics Committees: Advarra for Canada: Pro00049277 granted 4/04/2021; Australia: Bellberry 2021–05-507, 26/07/2021. Guided by Advarra it was concluded (and communicated to BresMed) that the study met the US criteria (at the time of submission) for exemption from ethics approval/IRB oversight. To assess the need for ethics approvial in the UK, the online NHS portal assessment questions were complemented and it was determined that ethics approval was not required. Therefore waivers were obtained for England, Wales, Scotland, and Northern Ireland. Of note, there were no designated clinical sites, centres, nor investigators in any of the four countries for direct recruitment of the study patients as it was an international online survey and recruitment of all patients was done via the CDCN. Informed consent was obtained from all individual participants included in the study before they could participate in the online survey. Study participants were able to withdraw from the study at any point. Consent to publish was obtained from all individual participants included in the study
Fig. 1
Hypothesis generation process. CDCN Castleman Disease Collaborative Network, iMCD idiopathic multicentric Castleman’s disease
Eligibility criteria included English-speaking patients aged ≥ 18 years with a self-reported healthcare practitioner-confirmed iMCD diagnosis. Patients enrolled in a clinical trial 6 months prior to the survey were excluded. Written consent was obtained from all respondents before they were permitted to participate in the survey.
The survey methodology including the development of the questionnaire, its validation, and administration have been extensively elucidated elsewhere [3]. Patients were asked what symptoms they had experienced over the past week and the severity impact of symptoms was explored on several domains of daily life which included pain/discomfort, mobility, diet, sexual functioning, emotional and psychological well-being, work/education, social life, general routine, personal relationships, financial well-being, and ability to travel. Questions related to patient-reported effects on daily life (e.g., due to symptoms or treatment) were assigned a Likert, ordinal scale numerical value from 0 to 4 for the following severity categories: 0, does not affect my daily life; 1, slightly affects my daily life; 2, moderately affects my daily life; 3, severely affects my daily life; 4, very severely affects my daily life. A higher number on the ordinal scale suggested worse severity in terms of patient-reported effect on daily life. An overview of the survey’s sections and specific questions and associated responses used for the psychometric analyses are provided in the Supplementary Appendix (SA)-S1.
HypothesesThese exploratory analyses are used to investigate the strength of the relationships between patient-reported symptoms and their perceived impact on daily life. A priori hypotheses were generated on the basis of an IMCD clinician’s expert opinion, one patient with iMCD, and one informal caregiver representative via in-depth interviews conducted between 10 and 12 November 2021 (Fig. 1). The interviews explored whether specific questions and response options could be grouped together as potentially related, e.g., if responses to one item would be related to responses on another item. For the interviews, a hypothesis inferring a positive relationship with a strong strength of relationship was posed, e.g., “if tiredness has a big impact on daily life for patients with iMCD, then so would physical weakness”, alongside which the responder would suggest if they thought this positive relationship would be of strong, weak, or no strength; this example relationship between tiredness and physical weakness was suggested to be strong. Hypothesized relationships were prioritized on the basis of the most common experiences and those that were perceived as most likely and important to patients and their caregiver, as well as those noted to be the strongest by the clinical expert; these hypotheses were subsequently grouped into three hypotheses sets.
Hypotheses Set 1 (HS-1): Specific Paired Symptoms’ Related Patient-Reported Effect on Daily LifeIt was hypothesized that specific paired symptoms would have either convergent (e.g., strength of relationship moderate to strong) or discriminant (strength of relationship none to weak) relationship with patient-reported effects on aspects of daily life (see Symptoms Q13 in SA-S1).
Three positive convergent relationships were hypothesized to exist, i.e., one symptom’s negative patient-reported effect on daily life would be related to the other symptoms’ negative patient-reported effect on daily life (SA-Fig. S1):
C1. Tiredness and weakness (physical).
C2. Tiredness and impaired cognitive function.
C3. Loss of appetite and weight loss.
Six discriminant relationships were hypothesized to exist (SA-Fig. S2):
D1. Dizziness and impaired cognitive function.
D2. Dizziness and loss of appetite.
D3. Dizziness and tiredness.
D4. Depression and tiredness.
D5. Loss of appetite and anxiety.
D6 Loss of appetite and weight loss.
Hypotheses Set 2 (HS-2): Number of Symptoms and Patient-Reported Effect of Symptoms on Aspects of Daily LifeIt was hypothesized that having a greater number of symptoms (Symptoms Q12, SA-S1) would have a positive convergent relationship with worse severity in terms of patient-reported impact of overall symptoms on specific aspects of daily life (i.e., Symptoms Q15, SA-Fig. S3).
Hypotheses Set 3 (HS-3): Receiving iMCD Treatment or Not and Patient-Reported Effect of Treatment on Aspects of Daily LifeIt was hypothesized that receiving treatment for iMCD [intravenous, oral, both oral and intravenous, or just for symptom management] (Treatment Q19, SA-S1) would be associated with less of a patient-reported effect of iMCD on aspects of daily living compared to those not on treatment (Impact of iMCD on your daily life Q33; SA-Fig. S4).
Statistical AnalysesThe analyses include all observed cases from the cohort (N = 51); whilst, the analytical sample size (n) varies dependent on the analysis being performed with relevant n values presented in the result tables. Construct validity assesses how well a measure represents the construct it was designed to represent whereby our construct of interest is iMCD burden, particularly in relation to patient-reported effect on aspects of daily life. We assessed internal construct validity (i.e., utilizing responses to different questions within the same questionnaire) in relation to internal convergent, discriminant, and known-group validity. All analyses were conducted in Stata 17.
Convergent and discriminant validity assesses the strength and direction of relationship between questions, based here on correlation analyses. Convergent validity here refers to the extent to which responses on a test or instrument exhibit a moderate to strong relationship with responses on conceptually similar tests or instruments. In contrast, discriminant validity here refers to the degree to which a test or measure has a weak to no correlation with another measure, whose underlying construct is conceptually unrelated. Given that the severity rating options common across hypotheses are considered categorical and ordinal, Spearman’s rank absolute correlation strength (ACS) and associated p value are used to indicate the degree to which questions are measuring related (i.e., convergent as for HS-1 and HS-2) or unrelated (i.e., discriminant for HS-1) factors. Correlation strength is described on the basis of Cohen’s ACS cutoffs: weak, < 0.3; moderate, 0.3 < 0.5; strong, ≥ 0.5. On the basis of these ACS values:
Convergent validity is suggested to be supported when there is an estimated moderate to strong and statistically significant relationship: ACS ≥ 0.3 and p value < 0.05.
Discriminant validity is suggested to be supported when there is an estimated weak to no relationship which need not be statistically significant: ACS < 0.3.
Known-group validity assesses the extent to which question scores differ between groups that are expected to differ, i.e., between treatment and no treatment groups for HS-3. Known-group differences are quantified using Cohen’s d standardized absolute effect sizes (AES; i.e., the difference in mean scores between the two subgroups divided by the standard deviation of the score for the no treatment group), where AES are defined as trivial, < 0.2; small, 0.2 < 0.5; medium, 0.5 < 0.8; large, ≥ 0.8. A positive effect size suggests the mean value of the no treatment group is higher than the treatment group (i.e., a more severe score); a negative effect size suggests the mean value of the treatment group is higher than the no treatment group. The p value is based on the Wilcoxon–Mann–Whitney test as a non-parametric test for statistical significance between independent sample distributions when assuming the data is at least ordinal. On the basis of these AES values, the known-group validity is suggested to be supported when there is an estimated medium to large effect size with a statistically significant difference between groups’ score distributions: AES ≥ 0.5 and p value < 0.05.
留言 (0)