
記住我

We will recruit 30 facilitators from NGOs, refugee shelters, FBOs, and churches who participated in the initial Hope Groups pre-post study [21], who are living in Ukraine, Poland, Spain, and the UK. Participants will be primarily located in these four countries—with the vast majority in Ukraine and Poland—while participants joining virtually may be displaced throughout Europe and beyond. In-person Hope Groups will be held at shelters, community centers, churches, and homes. We recognize that participants may move to different countries throughout the study, and there may also be weeks when it is unsafe to meet in person (e.g., during ongoing air strikes). We have prioritized a pragmatic and flexible delivery system which can transition between meeting virtually and in person as needed.
Eligibility criteriaParticipant inclusion criteria are as follows: participant (1) is Ukrainian, or another nationality and affected by the war in Ukraine; (2) understands the Ukrainian language; (3) is aged 18 or older; and (4) is a parent or caregiver for one or more children ages 0–17 years old. Participant exclusion criteria are as follows: (1) participants are not eligible if they have already participated in a Hope Group.
Facilitator inclusion criteria are as follows: facilitator (1) is Ukrainian, or another nationality and affected by the war in Ukraine; (2) speaks and understands Ukrainian; (3) is 18 or older; (4) is connected to an NGO, refugee shelter, FBO, church, or other networks of Ukrainians; (5) has had previous experience leading small group discussions; (6) self-defines as emotionally stable with the capacity to support others; (7) is willing to participate in Hope Groups trainings; and (8) is willing to recruit and facilitate two or four Hope Groups through their network, with the understanding that their groups will be randomized to intervention or control with a 1:1 allocation ratio. There are no inclusion or exclusion criteria for facilitators’ backgrounds; some facilitators are mental health professionals, while others have no previous mental health training.
Who will take informed consent?Facilitators and participants will consent to participation in the study. Facilitators and participants will both complete self-administered informed consent using their phones via a link to an Open Data Kit (ODK) form.
Additional consent provisions for collection and use of participant data and biological specimensIn informed consent, participants consent to making publicly available anonymized data and results to contribute to research identifying ways to strengthen caregivers amidst war. No biological specimens will be collected.
InterventionsExplanation for the choice of comparatorsThis study compares intervention clusters to waitlist control clusters. Facilitators recruit two or more Hope Groups. Logistically, facilitators could not implement all sessions simultaneously; thus, we relied on a random lottery system to select which clusters receive the intervention now and which are assigned to a waitlist to receive the intervention after the RCT concludes. Through utilizing a waitlist design, we expect that placebo effects will be effectively balanced between groups, as the control group’s knowledge of soon receiving a supportive intervention may yield improvements in their outcomes [24].
Intervention descriptionIntervention clusters receive the 12-session psychosocial, mental health, and parenting intervention called Hope Groups through trained facilitators (Table 1). All content is based on evidence-based principles and adapted by Ukrainians for the Ukrainian context. Mental health content utilizes key principles for psychosocial support in armed conflict to build participants’ skills in healthy grieving and coping, de-escalation and stress reduction, and self-care to address war-time challenges. Parenting and violence prevention content was based on content developed by Parenting for Lifelong Health (PLH) and endorsed by the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF). Additionally, content was informed by the “Ukraine Parenting” resources developed by the Global Initiative to Support Parents, WHO, PLH, UNICEF, United Nations High Commissioner for Refugees (UNHCR), United Nations Office on Drugs and Crime, Global Partnership to End Violence Against Children, and Early Childhood Development Action Network.
Table 1 Description of 12-session Hope Groups interventionFacilitators receive training on all 12 sessions, as well as overall training in supporting individuals in crisis, group facilitation, mental health referrals, mandatory child abuse reporting protocols, gender-based violence, violence against children, and research principles such as reducing spillover and loss-to-follow-up. Total facilitator training time is 14 h, with training sessions delivered in increments of 2 to 3 h at a time.
Hope Groups are generally implemented two times per week for 6 weeks; however, given the war crisis and based on the needs of participants, facilitators can elect to implement the Hope Groups three times per week for 4 weeks (e.g., particularly in shelter settings where participants are available for frequent meeting and may only remain in this setting for 4 weeks) or one time per week for 12 weeks (e.g., in settings where participants’ schedules do not allow more frequent meeting). This pragmatic delivery, which flexibly caters to the needs of a population living amidst a war, was consideredessential [25].
Criteria for discontinuing or modifying allocated interventionsAll participants are informed that they may stop participating in Hope Groups at any time, and all facilitators are trained to be flexible and adaptive based on the needs of the participants (e.g., pausing content within sessions to let participants share their personal struggles as needed, guiding the conversation to protect all participants from secondary trauma, and making appropriate mental health referrals as needed).
Strategies to improve adherence to interventionsWe created a facilitator manual to guide all 12 sessions, including content delivery, skills-building, and discussions. After sessions, we collect monitoring data from facilitators to explore whether all session content from the Hope Groups guide was completed. This study relies on a pragmatic design; facilitators are trained to deliver all session content, but we do not additionally intervene to ensure the Hope Groups guide is closely followed.
Relevant concomitant care permitted or prohibited during the trialWe have no restrictions on participants receiving other mental health, psychosocial, and parenting support during our study. We collect data on participation in other similar programs and will include this as a covariate in our models if prevalence is high in our sample.
Provisions for post-trial careCurrently, we have no structured plans for continued care after the completion of Hope Groups; however, in the pre-post study, we observed some facilitators and participants self-elected to maintain contact after the completion of Hope Groups. After the follow-up survey, we will assess the frequency of self-elected continued contact and change in participant outcomes from endline to follow-up, which may inform future adaptations for structured follow-up contact between facilitators and participants.
OutcomesFollowing guidance for research in war settings, researchers made every effort to create a highly sensitive, non-triggering, and brief survey for participants [25]. To achieve this, we adapted validated scales to be relevant to our context, often including relevant subscale items rather than full survey scales. Primary and secondary outcomes are detailed in Table 2; all outcomes are based on participant self-report. Other than Caregiver Mental Health (which uses the standard Patient Health Questionnaire-4 scoring), outcomes are adapted to ask for frequency of occurrence in the past 7 days. All outcomes are collected at baseline, endline, and follow-up, except for Violence Against Women outcomes, which will only be asked at endline and follow-up due to their highly sensitive nature. We also collect data on standard covariates such as age, sex, education, income, and other exploratory outcomes including oblast location at the onset of full-scale invasion, displacement status, military service, facilitator background (lay-trained or mental health professional), and mode of intervention delivery (in-person, virtual, hybrid).
Table 2 Outcome measuresParticipant timelineTrial endline will be reached approximately 31 weeks after the RCT’s launch (Figs. 1 and 2). Trial endline is 1 week post-intervention. We originally planned to continue the trial through a 6-week follow-up period; however, as missiles and bombings in Ukraine have intensified, Ukrainian partners expressed urgency to deliver the Hope Groups to control clusters immediately after trial endline, rather than delaying control clusters throughout a follow-up period, based on (1) the war context having detrimental impacts on caregiver mental health and violence against children, which results in an urgent need for psychosocial, parenting support; (2) strong results from our pre-post study [21]; and (3) concern that high mobility during the war crisis may result in control participants’ inability to participate if delayed through a follow-up period. This was recognized and adopted by all study investigators, who designed a plan to conduct an interim analysis after the first 20 clusters (~100 participants) reached endline to provide real-time data-based information to inform Hope Groups delivery to control clusters, with the following guidelines:
1.If we find evidence of a harmful effect across primary outcomes, we will pause all activity to investigate and make adaptations.
2.If we find evidence of a protective effect of Hope Groups across primary outcomes, even after incorporation of skeptical priors [34,35,36], this will be used to support the decision to end the trial after 1-week post-intervention and immediately deliver Hope Groups to control clusters (without delaying them through a follow-up period).
3.If we find evidence of a null effect, the trial will continue as planned through endline to enable the sample size to reach the target number. Additionally, we will incorporate enthusiastic priors [34, 35] based on information from the pre-post study [19]; if results remain null, we will still continue the trial until endline, but we will also collaborate with Ukrainian partners to make adaptations to Hope Groups prior to delivery to control clusters with the aim of strengthening the intervention. Adapted Hope Groups among control clusters would be assessed using a pre-post design.
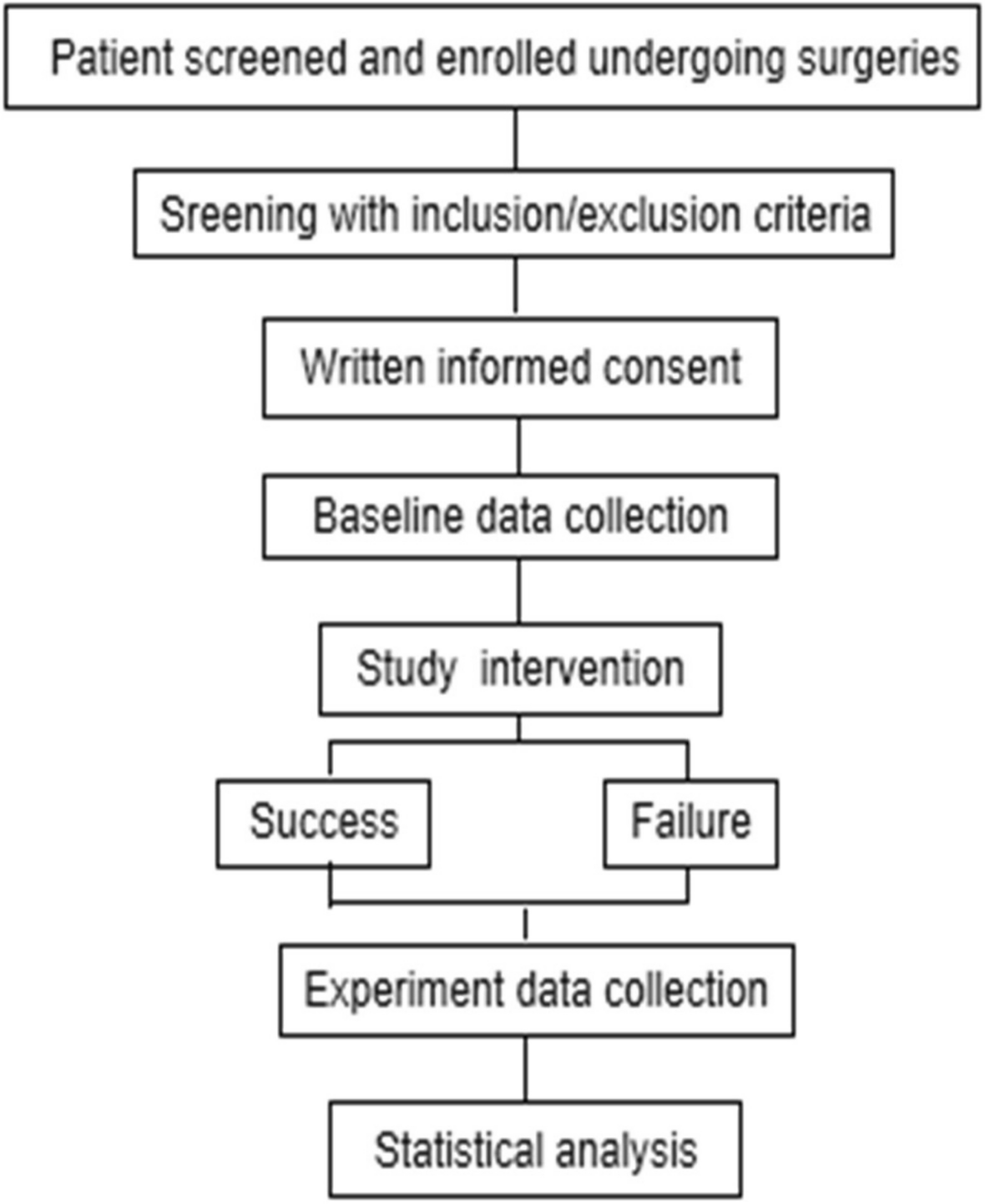
Fig. 1
Hope Groups randomized controlled trial flow chart: procedures and timeline
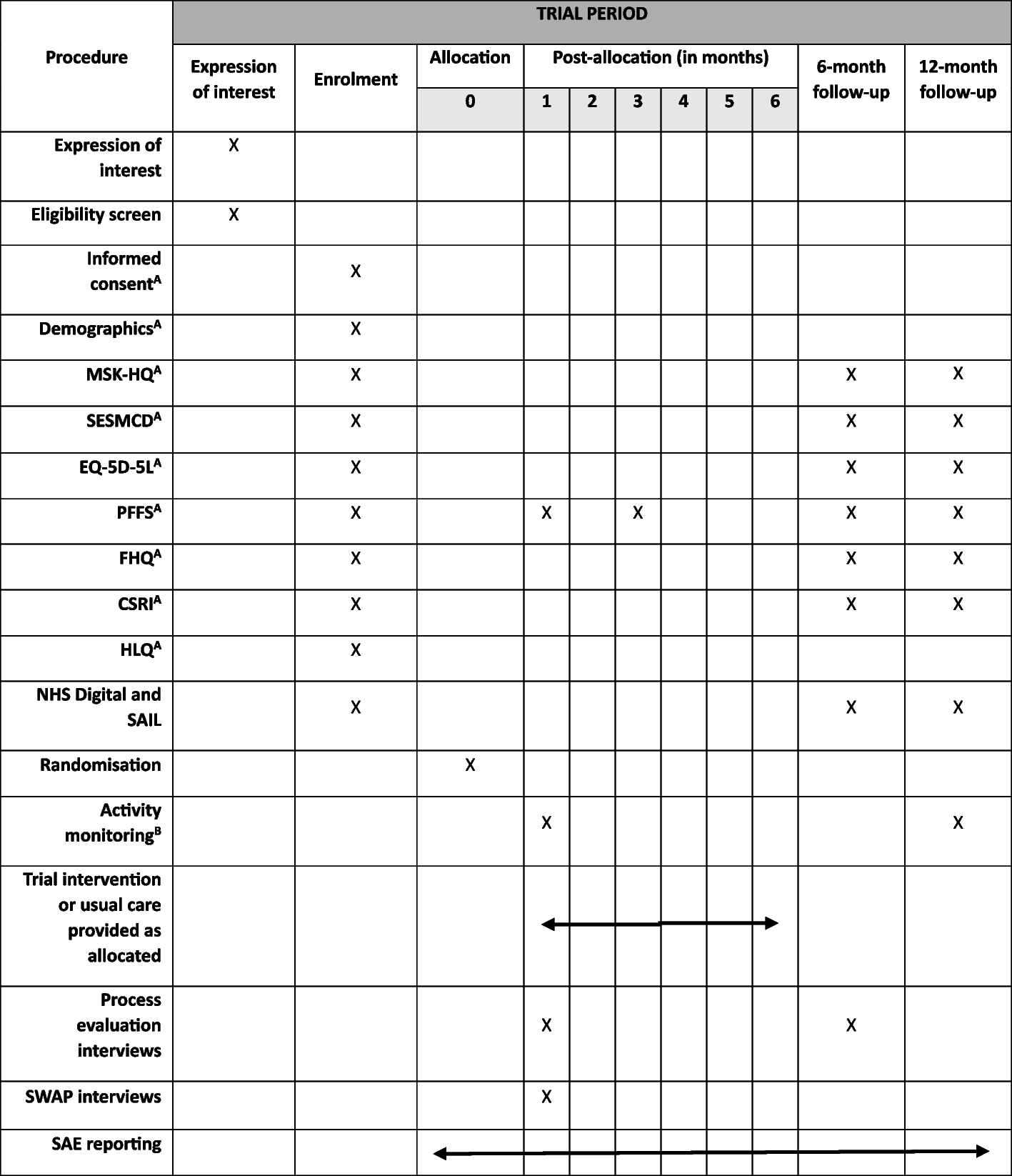
Fig. 2
SPIRIT timeline figure. t1 represents the intervention period; t2 represents the endline survey timepoint; and t3 represents the follow-up survey timepoint. The asterisk (*) indicates that the listed activity occurs only among the intervention group
Furthermore, if we find evidence of a protective effect, study investigators will design a statistical analysis plan to assess the long-term effectiveness of Hope Groups utilizing innovative approaches, as our RCT control group will have received the intervention and therefore will no longer be an appropriate comparison group. First, we will conduct a follow-up survey only among the intervention arm 6–8 weeks post-endline to assess if outcomes are receding towards baseline levels or maintaining improvement.
Second, to assess the long-term effectiveness of Hope Groups, researchers will aim to conduct 6- and 12-month quasi-experimental follow-ups, pending war circumstances and funding. Building on recent research highlighting the potential for longitudinal matching methods to yield results consistent with long-term RCT results [37], we intend to utilize multiple quasi-experimental methods, including rolling entry matching [38], a longitudinal matching method which improves exchangeability when relying on randomization is not feasible or ethical, to estimate the long-term effects of Hope Groups. Following this design, treated participants from the RCT’s intervention group will be matched with untreated participants’ baseline surveys upon their enrollment in future Hope Groups programming, at the same 6 and 12 months post-RCT timepoints. A separate statistical analysis plan will be registered for any long-term evaluations on OSF.
Sample sizeThis study will enroll k = 90 clusters of 4–7 participants, totaling approximately n = 450 participants (assuming an average cluster size of m = 5). The sample size was determined by power calculations from the pilot study and funding limitations. Based on estimated effect sizes, ICCs, and SDs of the outcome in the population from pilot data, and accounting for attrition in an active war context, we estimated that k = 90 clusters and n = 450 participants would be sufficient to detect significant effects with 80% power in all primary and secondary outcomes, except for physical abuse, which we may not be powered to detect an effect in. However, our funding limits increasing the sample size beyond this. Our final sample size may vary based on the average cluster size.
RecruitmentThere will be a rolling recruitment and enrollment strategy, with recruitment efforts ending when all facilitators have recruited the full number of participants for their groups. Hope Groups facilitators will recruit participants through their own networks (e.g., NGOs, shelters for internally displaced persons (IDPs) and/or refugees, FBOs, or churches) to participate in their 12-session Hope Groups. This approach to recruitment is based on the guidance of Ukrainian partners and humanitarian research experts [25]. It is especially important in humanitarian contexts for people to know and trust the organizations and people recruiting them for resources, especially in Ukraine, where psychosocial programming is historically uncommon. Therefore, to successfully achieve the target sample size, it is essential for participants to be recruited by someone they know and trust. Because of this programmatic necessity, our study design is matched to facilitator, to ensure all confounders within a facilitator’s recruitment network are balanced between study arms.
留言 (0)