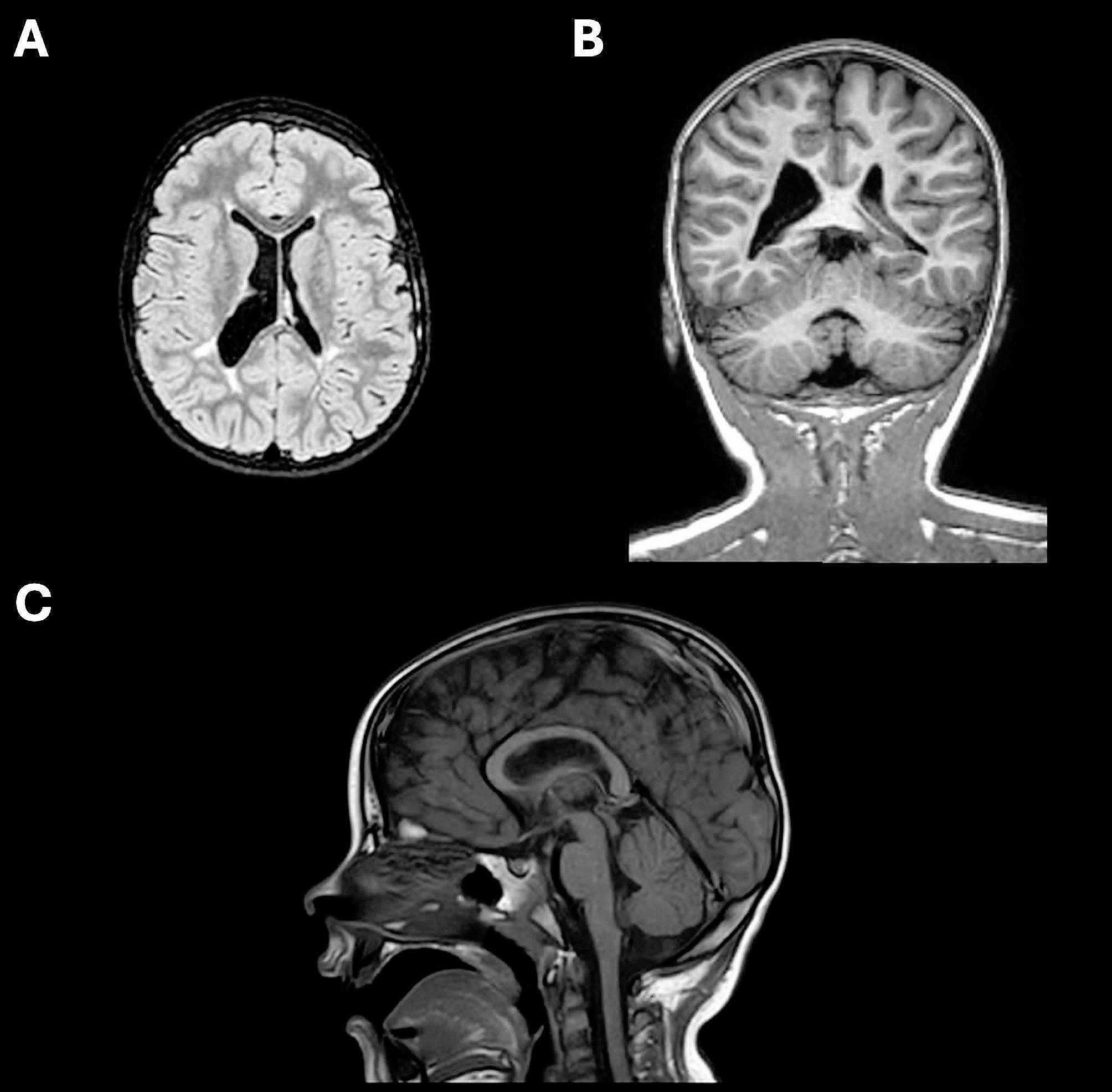
In this case report, the patient presented with visual impairment and dyspraxia, but did not meet the criteria for asymmetric refractive bilateral amblyopia. This condition is typically defined as best-corrected visual acuity of 20/40 or worse in both eyes with an interocular difference of two lines or more, in the presence of 4.00 diopters (D) or more of hypermetropia by spherical equivalent, 2.00 D or more of astigmatism, or both in each eye [7]. Additionally, the patient displayed abnormal results on VEP testing. This prompted further evaluation with a brain MRI, which revealed structural abnormalities in the brain consistent with CVI secondary to hypoxic-ischemic damage.
Many works show how MRI-detectable changes can provide valuable insights into clinical outcomes, reveals significant brain abnormalities that correlate with specific neurological manifestations [8]. In prematurely born infants, MRI-detected alterations in the corpus callosum, cingulum, anterior commissure, fornix, and right uncinate fasciculus have been reported to correlate with eye-hand coordination but not linguistic performance [9]. Conversely, impaired linguistic performance has been associated with disruptions in the frontal region, particularly the ventral precentral gyrus and the arcuate fasciculus [10]. In our case report, the impairment in eye-hand coordination can be ascribed to the alterations in the corpus callosum, and possibly in the right uncinate fasciculus (given the extent of the anterior dilation of the right lateral ventricle) detected on MRI.
CVI is the leading cause of visual impairment in children in the USA [11] and in Europe [12, 13]. Although current practice standards recommend early intervention [2] on motor and cognitive skills, little is known about which interventions are best suited to vision and there is currently no standardized treatment for CVI. The only randomized trial was conducted in 1991 and indicates that a developmental approach to early vision promotion leads to faster improvements in all vision functions [14]. Several confounding variables, such as the coexistence of other neurological and ophthalmological anomalies and the inherent processes of children’s physiological development, make it challenging to ascertain accurate correlations between interventions and outcomes [2]. However, timely interventions, including modifications to the visual environment, comprehensive multidisciplinary care and surgical procedures, have been shown to be beneficial in treating ocular and systemic comorbidities in affected children, supporting an effective rehabilitative process [15, 16].
Typical interventions in patients with CVI encompass visual stimulation techniques for both eyes, such as exposure to light, patterns, or slides [17], and strategic environmental modifications, such as simplifying the visual environment, minimizing crowding, and using objects with distinct colors, high contrast, and motion to facilitate visual recognition. Infants and toddlers under the age of two are generally the only ones targeted by these treatments. However, empirical outcomes have been variable, indicating that children diagnosed with CVI may achieve improvements with or without the application of visual stimulation strategies.
In the case study presented, the intervention was implemented at a later stage—at five years of age—yet still within the critical period of neural plasticity. The efficacy of the anti-amblyopic approach employed demonstrated the nervous system’s substantial capacity for adaptation and recovery, a phenomenon that underscores the broader principle of brain plasticity, where structural changes in brain circuitry or modifications of the synaptic connections can happen in response to variations of environmental stimuli [18]. Such plasticity, which diminishes with age, becoming mild after 8–10 years, has also been demonstrated in cases of childhood brain injuries, including cases of hypoxic ischemic encephalopathy [19].
In our case report, concurrent multidisciplinary rehabilitation has allowed for a significant improvement in motor skills as well. In fact, even a small correction of astigmatism has led to an improvement in the visual acuity of the better eye in just 4 months, while occlusion allowed a significant improvement in the worse eye within 8 months, periods too short to justify the improvement as a result of a developmental process in a child already 5 years old. Furthermore, given the absence of strabismus or significant refractive defects, these improvements cannot be due to amblyopia recovery but to a better use of the visual pathway, even if damaged.
In conclusion, this case report illustrates the successful implementation of anti-amblyopia therapy in a child with CVI (Table 1) and allows us to affirm that it is necessary to correct all refractive defects, even if of little amount, and to implement all possible therapies (occlusion, macular stimulations, and others) to improve the vision of these children, in the context of multidisciplinary rehabilitation. Further studies will be needed to understand the potential for broader application of anti-amblyopia therapy in similar cases, which could be crucial in defining treatment protocols and ultimately enhancing the quality of life for children affected by CVI.
Table 1 Case report timeline



留言 (0)