Since the use of US has increased exponentially worldwide in the last few decades, also for the pediatric age [1], we aimed to provide data on the current Italian state of pediatric US practice.
US equipment and applications
The US spread is strictly related to the availability of machines: the majority of participants declared to have a US machine available for use within the department, with percentages in line with the literature [22, 23]. Particularly, convex and linear probes have been found to be the ones most obtainable for US examinations.
US practice seems to be relatively recent tool in pediatrics [4], considering that machines have been provided mostly 1–5 years prior to the survey. Nevertheless, the vast majority of US machines have been found to be conventionally cart-based, at the expense of newer models such as portable and handheld systems [13], which have been demonstrated to improve patient outcomes also in environments with limited resources [24]. These results focus on the urgent need to direct more resources for improving US equipment and advanced scanning technologies in pediatric units.
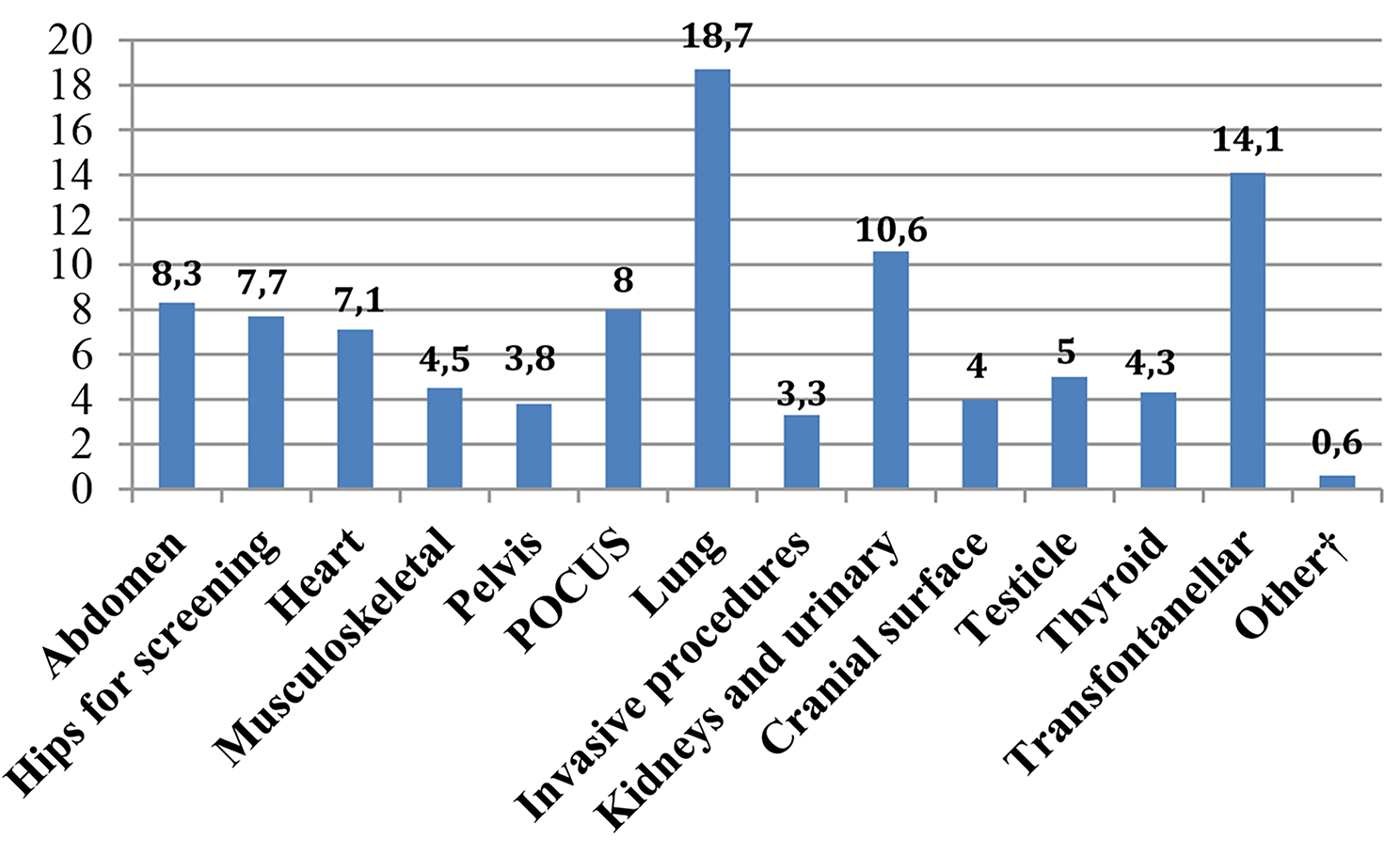
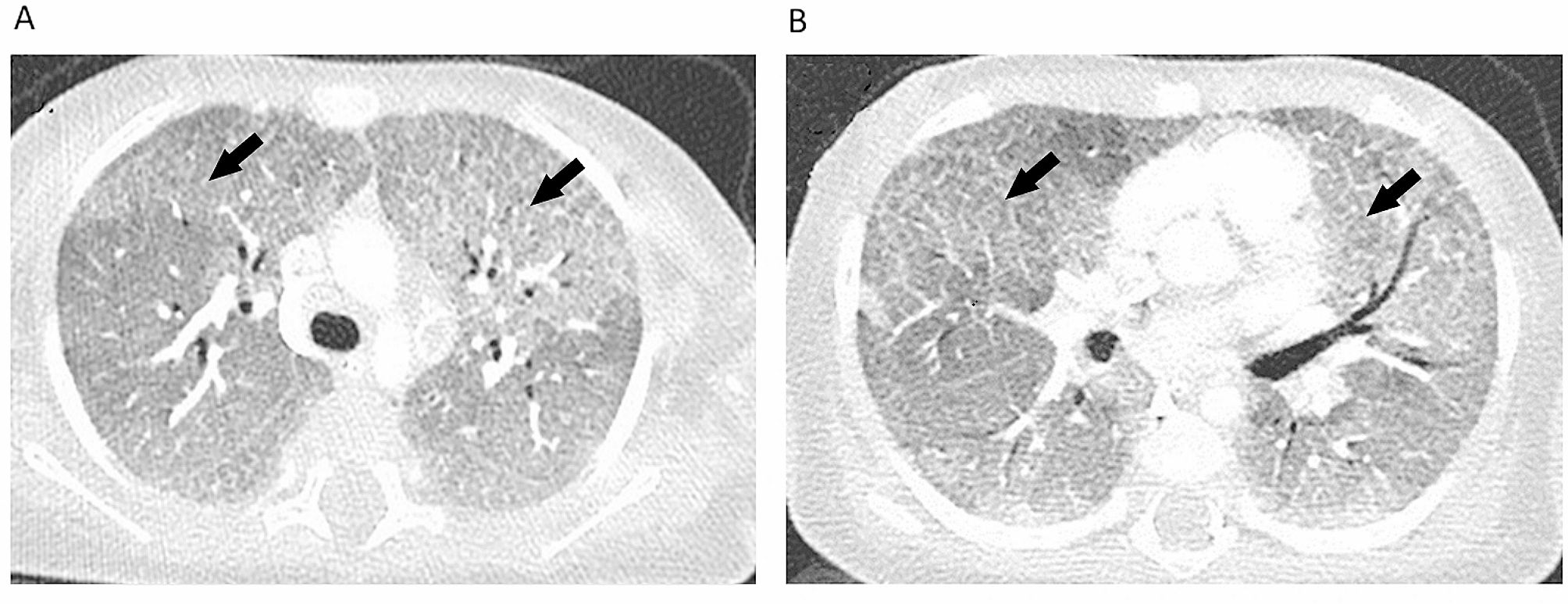
Concerning the type of examination, lung resulted to be the most common scanned region. We also found that participants working in the emergency room, mostly use US in suspicion of lung pathologies. Similar results were also highlighted for family pediatricians. A possible explanation for this finding may be the steep learning curve which also allows novices to be able to perform lung US [25]. It should be also underlined that nearly one third of respondents assessed to use US for cardiac and abdominal application: traditionally, the use of US for these two anatomic regions is a prerogative of cardiologists and radiologists, respectively [5]. This finding may be considered as the beginning of a growth path to be pursued in the future for the entire pediatric personnel [26, 27].
US practice among different pediatric settings
Some differences on US practice between pediatric residents and pediatricians have been found in this survey. Among residents, only half declared to use US, mostly with little experience and low scanning frequency. On the contrary, the majority of attending pediatricians routinely perform US, although less than half of them with experience over ten years and a scanning frequency more than twenty per month. Controversial data are reported in literature about disparity in US application between residents and pediatricians [6]: regarding the Italian situation, we can speculate that, despite the growing interest on US in last decades, the method still needs to be spread and implemented in clinical practice, especially during residency.
The vast majority of the surveyed family pediatricians report to perform US routinely. As far as we know, the present survey is the first study investigating US application in pediatric family care, so we are not able to compare our data with similar findings in literature. Our results even seem to be in contrast with those described by a recent survey which reports a low percentage of US scans performed among family medicine residents and practicing physicians [28]. We hypothesize that the high percentage of US utilization among family pediatricians may reflect a bias selection.
Finally, we did not find statistically significant differences for US practice dividing the sample by geographical area (north, central or south) or working department. We definitely believe that this last result should be verified on a larger study sample. We were not even able to compare our data with those in literature since, as far as we know, there are no studies comparing the US use in the private, public or university setting nor for different geographical areas of the same nation.
US and education
The section of the survey dedicated to training underlined interesting issues. To date, an informal experience-based training or theoretical-practical courses have been found to be the most frequently adopted while a credentialing process was missing in most cases. Similar findings are reported in literature, pointing out the lack of specific training pathways and non-homogeneous programs [29,30,31]. Learning methods also vary based on different realities. In middle and low-income countries, e-learning methods have been reported to be the commonest method, related to the high costs of face-to face training [11]. Nevertheless challenges relating to poor internet connectivity still affects access to study platform and communication with supervisors [11].
The standardization of training plans, starting preferably during residency rather than early under graduation medical period, might allow to create a US curriculum as guarantee of educational pathway and quality assessment [32, 33]. Furthermore medical school/residency directors and their institutions should consider the curriculum as a core requirement for the implementation of US technique [33]. More than half respondents within the pediatric residents subgroup declared that a specific training program has yet to be described; however, almost all of them showed a positive attitude towards US, supporting its endorsement during residency, as previously underlined in literature [5, 34].
Barriers to POCUS applications
Our survey points out possible barriers to POCUS applications. Among these barriers, the lack of well-defined training plan has been identified as a main obstacle to US expansion by respondents: we strongly believe that an educational US curriculum should be mandatory not only for residents but also for attending physicians, as reported in recent literature [35, 36].
Despite the dramatic rise of US use, it is noteworthy that the unavailability of US machine is still considered as a barrier for daily practice in both our study and literature [8, 9]. Actually, some major reasons for complaints from physicians are the expensiveness of US machines and the subsequent difficulty in affording to purchase them by institutions, the scarce use of low-cost ultraportable devices, the US equipment deficiency and the inaccessibility to US machines for bedside use, often due to resistance from other departments [5, 8, 9, 30, 37]. The lack of technological devices for performing US is reported to be a barrier to the implementation of the method even in middle and low-income countries where clinicians often deal with the high costs of equipments, adverse climatic conditions, power instability, and inadequate maintenance service [11].
If the unavailability of US machines is indeed an absolute requirement for US practice, proper education still remains a main issue to be acknowledged [15]. First of all, sufficient time for training should be given since a number of reports indicates a lack of time to learn [9, 16, 30]. Moreover, a well-structured educational program could implement the small number of trainers within various institutions [8]. Last but not least, an ongoing education should be mandatory for all credentialed US physicians [15] in order to improve and consolidate their sonographic skills.
Regarding the liability concerns, they may be closely related to the lack of credentialing plan and quality assurance program in case of misinterpretation or misdiagnosis leading to malpractice claims [29, 38]. Again, healthcare professionals should be aware that literature provides non-apprehensive data about litigation directly related to US application in the last decade [39]. Furthermore, to improve ultrasound skill and reduce concerns about the sense of responsibility, with the possibility of using US more in daily clinical practice, it is not only necessary to train ultrasound skills but also training to imaging evaluation starting, for example, from the study of CT findings or anatomical information.
From the perspective of survey respondents, US has been highly scored in term of usefulness in order to integrate the patient’s clinical evaluation and guide clinical decision, confirming positive attitude toward US application [6, 12, 40, 41].
POCUS during the COVID-19 pandemic
The last two questions of the survey investigated the perception of US role during the outbreak of the COVID19 pandemic. Italy has been the first european country to deal with COVID-19, serving a resilient assistance both in emergency departments and outpatient clinics nationwide [42]. Despite the enormous efforts to better understand clinical features of COVID-19 disease [42, 43], participants assumed that the pandemic does not seem to have implemented neither the use nor the knowledge expansion of US in pediatrics. This unexpected issue may be due to possible challenges in logistics of US examination (e.g. lack of portable ultrasound machines, high risk for contracting the COVID-19 infection) [44]. On the other hand, the further analysis for the subgroup of pediatricians working in ED found that both US use and knowledge were improved during the pandemic maybe due to a focused attention on emergency and COVID patients.
Limitations and strenghts
Our study had a number of limitations and strenghts. The first limitation is intrinsic to the nature of the survey which is self-reported designed. Another limitation low response rate, which may reflect a lack of participant involvement and motivation on this topic. Actually, a potential response-bias could be due to the overestimation of US users among respondents, as those more interested in US technique may have been more like to respond. Regarding possible strengths, this study is one of the few survey which investigated the US application not only in pediatric emergency department but also in outpatient clinics. Moreover the survey was not targeting to a specific population sample, including pediatric residents, pediatric hospitalists and family pediatricians.

留言 (0)