
記住我


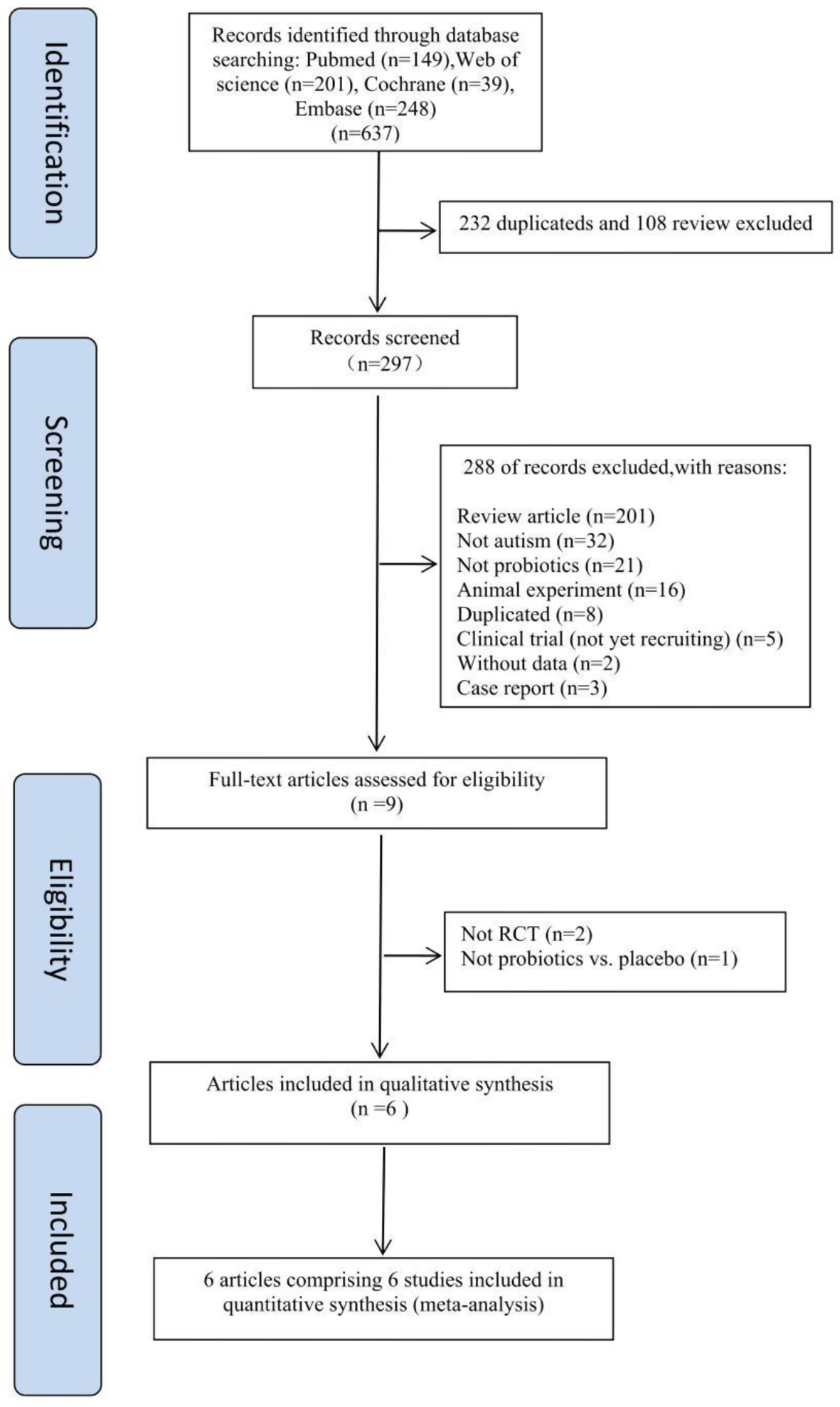
This study conducted a comprehensive search in authoritative databases including PubMed, Embase, and Web of Science by combining subject terms and free words. The subject terms comprised “Mycoplasma Pneumoniae Pneumonia,” “Thromboembolism,” and “Plastic Bronchitis.” Boolean operators “AND” and “OR” were employed to connect related synonyms and expanded vocabularies, such as “Mycoplasma infections” and “Pulmonary embolism,” ensuring the search results’ comprehensiveness and accuracy.
Previous reports have indicated that thrombosis or plastic bronchitis can manifest independently following Mycoplasma pneumoniae infection. Instances of severe Mycoplasma pneumoniae pneumonia accompanied by thrombosis and plastic bronchitis are not uncommon. Therefore, after excluding articles with incomplete data and cases of mixed infection, this paper focuses on eight relevant articles. Early detection and proactive interventions such as thrombolysis, anticoagulation, and bronchoscopy treatments often lead to improved prognoses shown in Table 4.
However, detailed case reports regarding thrombosis and plastic bronchitis resulting from Mycoplasma pneumoniae infection are lacking. Similarly, the mechanisms underlying Mycoplasma pneumoniae-induced thrombosis and plastic bronchitis remain unexplored. Although Liu J’s report mentioned four concurrent cases, no detailed introduction or summary was provided. This suggests that while cases of simultaneous thrombosis and plastic bronchitis may have occurred previously, they have not been thoroughly understood or documented. This paper presents five cases of concurrent thrombosis and plastic bronchitis, aiming to elucidate the underlying mechanisms and enhance understanding of these related conditions.
Table 4 The therapy regimens and outcome of the literature review of the MPP-associated thromboembolism with PBMycoplasma pneumoniae has been shown to directly or indirectly [3] induce airway inflammation by recruiting a substantial number of inflammatory cells and mediators, such as TNF-α, IL-1β, H2O2, and hypoxia-inducible factor [13]. These factors are known to lead to the structural damage to lymphatic vessels in the lungs [14]. Consequently, the disrupted structure of pulmonary lymphatic vessels compromises their ability to efficiently absorb inflammation [15] and regulate immune responses [16]. As a result, the accumulation of pleural effusion or pleurisy occurs [17], as observed in the cases presented in this study. Furthermore, Mycoplasma pneumoniae significantly stimulates the VEGF-C/VEGFR-3 signaling pathway, leading to lymphatic vessel hyperplasia [18]. This hyperplasia can establish a direct connection between the channels of pulmonary vein circulation. The leakage of lymph from damaged lymphatic vessels, along with the presence of inflammatory cells in the trachea, contributes to the development of type I plastic bronchitis, which is similar to the outcomes of Fontan surgery [19, 20]. Leaked lymph increases blood viscosity, damages blood vessel walls, and disrupts the balance of the fibrinolytic coagulation system, ultimately leading to the formation of blood clots. This may explain the higher susceptibility of pulmonary blood vessels to thromboembolism [21, 22], which is supported by the fact that four out of five thrombosis sites in our cases were observed in the lungs as shown in Fig. 3.
Fig. 3
MPP-associated thromboembolism with PB mechanism diagram
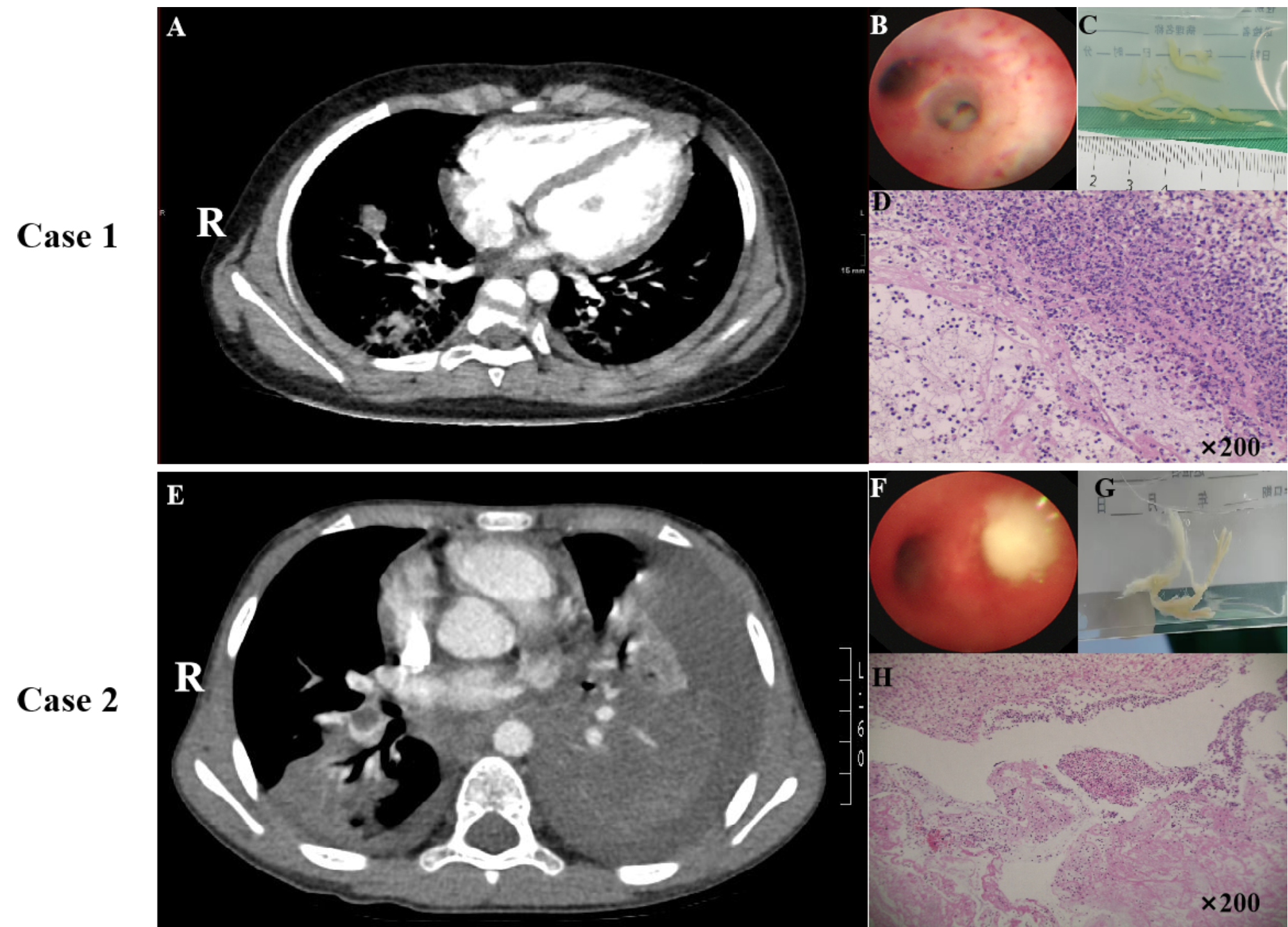
After an average time from onset of 6–13 days (mean = 9.8 days), imaging findings in patients demonstrated atelectasis and extensive pulmonary inflammation and consolidation. Bronchoscopy plays a crucial role in both diagnosing [23] and treating pulmonary inflammation and pulmonary ventilation dysfunction [24]. Following the criteria set by Wang L’s team, we conducted fiberoptic bronchoscopy and alveolar lavage fluid examination [25]. Fiberoptic bronchoscopy identified multiple plastic tracheal obstructions, which were successfully removed using forceps followed by alveolar lavage. Pathological analysis confirmed that the removed plastic substance was consistent with type I plastic bronchitis. Despite the alleviation of airway obstruction and identification of the pathogen, the consolidation area in the lungs did not show significant improvement on chest X-ray. Managing plastic bronchitis is a challenging task, often requiring repeated bronchoscopy for cast removal [26]. Subsequent bronchoscopy examination revealed a significant amount of mucus plugs in the trachea, which were cleared, resulting in improvement on chest X-ray.
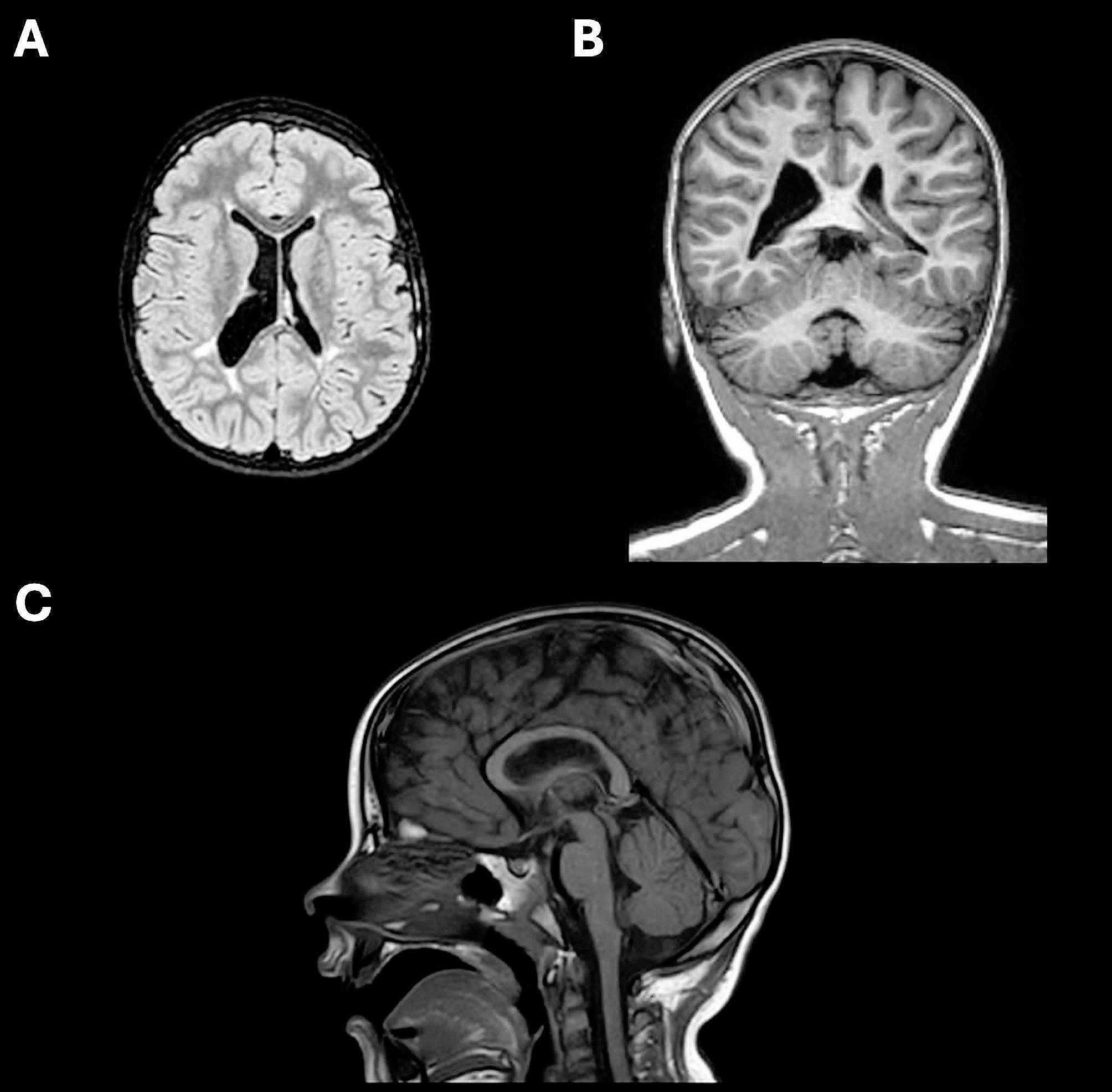
After an average duration of 13–22 days from the onset of symptoms (mean = 16 days), the children’s blood oxygen saturation remained below normal levels. Given the elevation of D-dimer levels and the possibility of pulmonary embolism [27], the children underwent a CTA examination, which confirmed the presence of pulmonary embolism in 4 cases. In three of these cases, the emboli were located in the right lower pulmonary artery, while in 1 case, both lower pulmonary arteries were affected. It is noteworthy that only one case (case 4) presented with symptoms of chest pain and hemoptysis, while the remaining cases were asymptomatic. In case 5, typical symptoms of cerebral embolism were observed, including right hemiplegia, dysarthria, and cognitive impairment. Urgent MRA was performed, revealing interruption of blood flow in the left internal carotid artery and middle cerebral artery, thus confirming the diagnosis of cerebral embolism.
Hormonal therapy, in conjunction with appropriate antimicrobial agents, has demonstrated promising outcomes in the management of refractory MPP [1]. In our treatment regimen, azithromycin was included based on the literature indicating potential immunomodulatory and anti-inflammatory effects, even in the presence of drug resistance [28]. Notably, corticosteroids have been proven to effectively suppress inflammation and offer a cost-effective solution. In our previous investigations [29], early administration of high-dose corticosteroid pulse therapy for patients with refractory Mycoplasma pneumoniae pneumonia presenting with elevated laboratory inflammatory markers and pleural effusion was shown to be advantageous in controlling the patient’s condition and prognosis. Following hormone therapy in all five cases, a rapid interruption of the inflammatory storm and swift normalization of body temperature was observed within a few days. Subsequently, we gradually and steadily reduced the hormone dosage, and importantly, no recurrence of the patient’s condition was observed thereafter. These findings suggest that a more cautious approach to the utilization of corticosteroid hormones may be warranted for similar patients.
Currently, the treatment of thrombosis consists of anticoagulant therapy, thrombolytic therapy, and surgical thrombectomy [30]. However, the management of MPP complicated with thrombosis is relatively rare and lacks a standardized approach. Drawing from the American Guidelines for the Treatment of Thrombosis in Children [31] and our team’s previous experience in managing MPP thrombosis [7], we devised a conservative management protocol that involves using low molecular weight heparin (LMWH) for anticoagulation at a dosage of 2 IU/kg/day while regularly monitoring levels of D-dimer and fibrinogen (Fg). It is important to note that relying solely on D-dimer measurement to exclude pulmonary embolism may lead to the oversight of smaller subsegmental emboli [32]. Therefore, we incorporated Fg as an additional marker to more accurately assess the body’s coagulation status. LMWH has demonstrated effectiveness, safety, and good tolerability in children, thereby reducing the risk of pulmonary necrosis [33]. However, in cases where patients present with cardiovascular or cerebrovascular embolism or experience hemodynamic changes, we employ thrombolytic therapy (case 5).
Nonetheless, it is regrettable that several limitations persist, notably a restricted sample size. Moreover, there are instances of incomplete clinical data and laboratory examinations for patients. Thirdly, it is imperative to conduct further exploration into the specific mechanisms responsible for complications related to thrombosis and pulmonary embolism induced by MPP.
留言 (0)