Search results and characteristics of the included studies
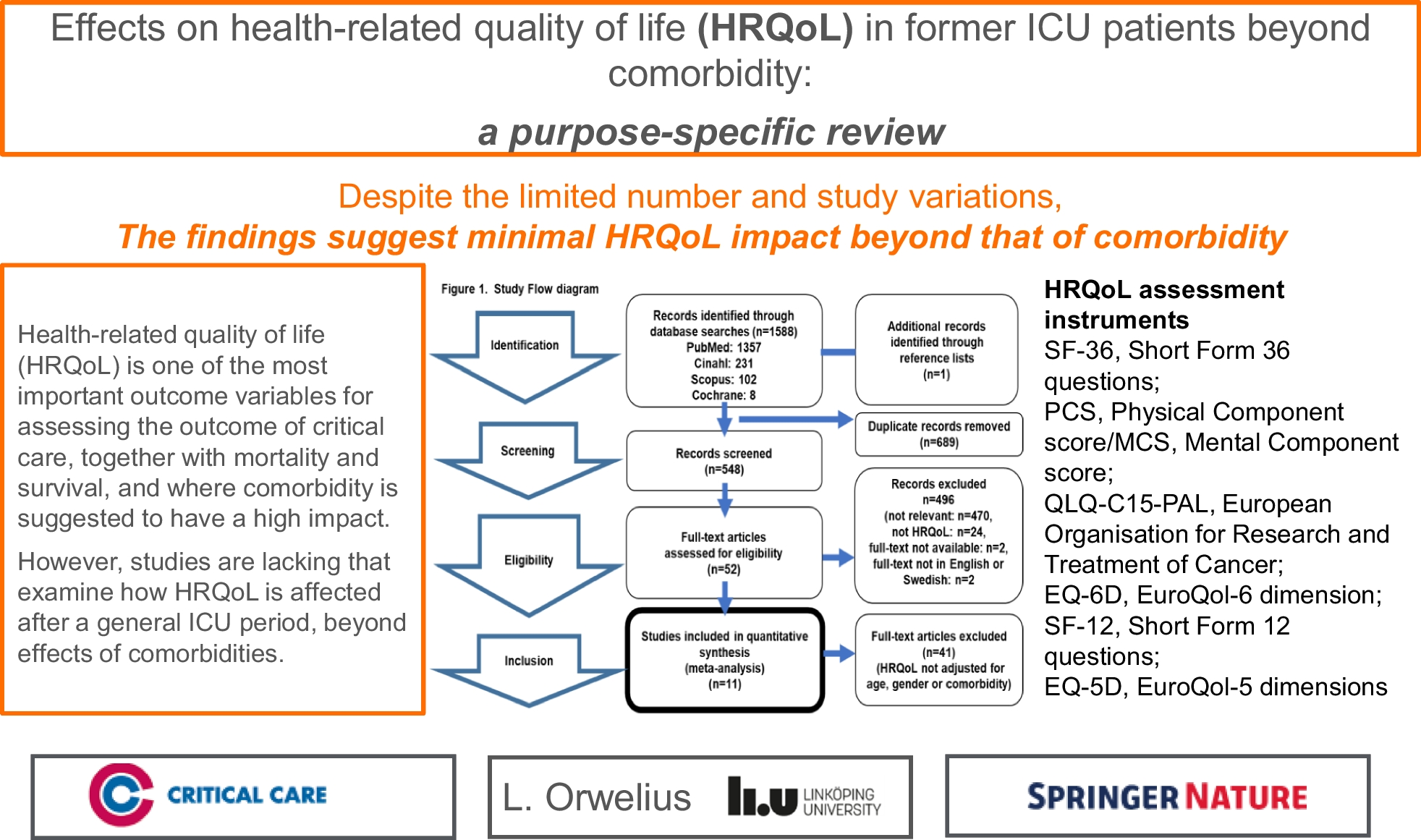
A total of 1588 references were identified by the database searches, and in addition one reference was identified through reference lists. After duplicated articles (same findings by different search engines) were removed (n = 1041) 548 abstracts were screened. Of these, 496 articles were excluded after reading the title and the abstract because they did not meet the predefined study criteria. The remaining 52 articles were read in full and of these 41 articles were excluded because they did not meet the final inclusion criteria; HRQoL comparisons adjusted for age or comorbidity. Finally, a total of 11 articles were included in the review (Fig. 1).
Most studies were conducted in Europe [13,14,15,16,17,18,19], two in Australia [20, 21], and one each in Canada [22] and USA [23]. All studies were observational prospective cohorts, except one that was a case–control study [21], one a cross-sectional comparison study [15], and one that was a retrospective cohort study (Table 1).
Table 1 Characteristics of included studiesInstrument and methods for measure of HRQoL
HRQoL was assessed using two general tools (SF-36 or SF-12 and EQ-5D) and one palliative care-specific tool (EORTC QLQ-C15-PAL). The most frequently used instrument was the Medical Outcomes Study 36-Item Short-Form health Survey (SF-36) [13, 15, 17, 19,20,21, 23] or its short-version 12-Item Short-Form Health Survey (SF-12) [22] (62%), followed by the EuroQol-5D (EQ-5D) [14, 16, 18, 22] (31%), whereas the European Organization for Research and Treatment of Cancer (EORTC) QLQ-C15-PAL were used in one study [21] (7%). Two studies used a combination of HRQoL instruments: EORTC QLQ-C15-PAL with the SF-36 [21], and the EQ-5D with the SF-12 [22] (Table 1).
Method of assessment for HRQoL varied between the 11 included studies. Almost half of them (46%) used mailed questionnaires [15, 16, 18, 19, 23], whereas two used telephone interview (18%) [17, 22], two used face-to-face interview (18%) [13, 14], and two used a combination of face-to-face interview and/or telephone interview (18%) [20, 21] (Table 1).
An overview of HRQoL assessment after ICU discharge is shown in Table 2. Inclusion periods were for most of the studies between one and four years [13, 15, 18, 20,21,22,23] and ≤ 1 year in two of the studies [16, 19], whereas the inclusion period was not presented in two of the studies [14, 17].
Table 2 Assessment of health-related quality of life after ICUA total of 18,566 critically ill patients were included in the 11 studies, and the response rate ranged between 16 and 94%.
Follow-up period
Follow-up periods for the assessment of HRQoL varied between the included studies from short follow-up (3 months) to long-term follow-up (5 years). All studies had a strict time-point for follow up except for two that had wide ranges of 18–24 months [17] and 4–5 years [20] after ICU discharge, respectively. The strict time points varied between 6 months [15, 16], 12 months [14, 18], and 18 months [13, 19]. Two of the studies assessed HRQoL over time at several occasions: 6 and 12 months after hospital discharge [22], and 3, 6, 12, 18, 24, and 30 months after enrolment [23] (Table 2).
Study criteria (Table
3
)
All the included studies met the third, and final quality criteria stage for inclusion; the HRQoL comparisons adjusted for age or comorbidity. All but one study [20] did HRQoL comparisons adjusted for comorbidity, and more than half of them (54%) did HRQoL comparisons adjusted for both comorbidity, age, and sex [13, 15, 18, 19, 22, 23].
However, only two (18%) of them met all the predefined study criteria at the second stage; assessment of HRQoL, exclusion criteria, including demographic characteristics and comparisons of responders vs. non-responders, and HRQoL comparisons adjusted for age and sex [15, 19].
Six of the studies showed detailed HRQoL scores [15, 18,19,20, 22, 23], but for one of them [22] only the component scores for SF-12 were given. Exclusion criteria were given in all but two studies [21, 23], and a description of the non-responder group and comparison with patients who responded to the HRQoL survey were given in four of the studies [15, 16, 19, 23] (Table 3).
Health-related quality of life adjusted for comorbidity
A common finding amongst the studies that fulfilled all the inclusion and none of the exclusion criteria (n = 11), was that comorbidities were found to be the most important factor affecting HRQoL after critical care. Amongst the eleven studies, seven used comorbidity scoring systems (Charlson (n = 7) and APACHE (n = 4)). A significant observation was that three studies (n = 3) included a comorbidity-adjusted control group (Table 2) [15, 21, 23]. For these three studies, there were difficulties in documenting any significant effect of the critical care period itself on the registered HRQoL after the critical care period. A summary of the major findings for long-term HRQoL per article is shown in Table 4.
Table 4 Major findings and factors influencing long-term health-related quality of life 

留言 (0)