
記住我

Between 2006 and 2010, the UK Biobank recruited approximately 500,000 individuals aged 40–69 years from the National Health Service register. Detailed information regarding the study design and methodology can be found elsewhere [17]. During the participants’ initial visit to the study centre, the research team conducted a comprehensive assessment, which included administering questionnaires, conducting brief interviews, performing physical tests, and collecting blood samples.
The blood collection vessels (vacutainers and collection pots) were processed using various automation systems to generate multiple aliquots for long-term storage. These aliquots are split equally: half stored in a fully automated − 80 °C working archive and the other half in a manual, nitrogen-vapour back-up archive at separate sites to prevent degradation from freeze-thaw cycles or loss due to archive site breakdown. Standard haematological tests were conducted on fresh whole blood within 24 h of collection for all participants. Conversely, the biochemistry assays, including albumin, were carried out after extraction from the freezer and thawing. However, only the tubes needed for the biochemistry assays were removed from the freezer and thawed, while the remaining aliquots on each plate were returned to the working archive still frozen, to prevent unnecessary freeze-thaw cycles.
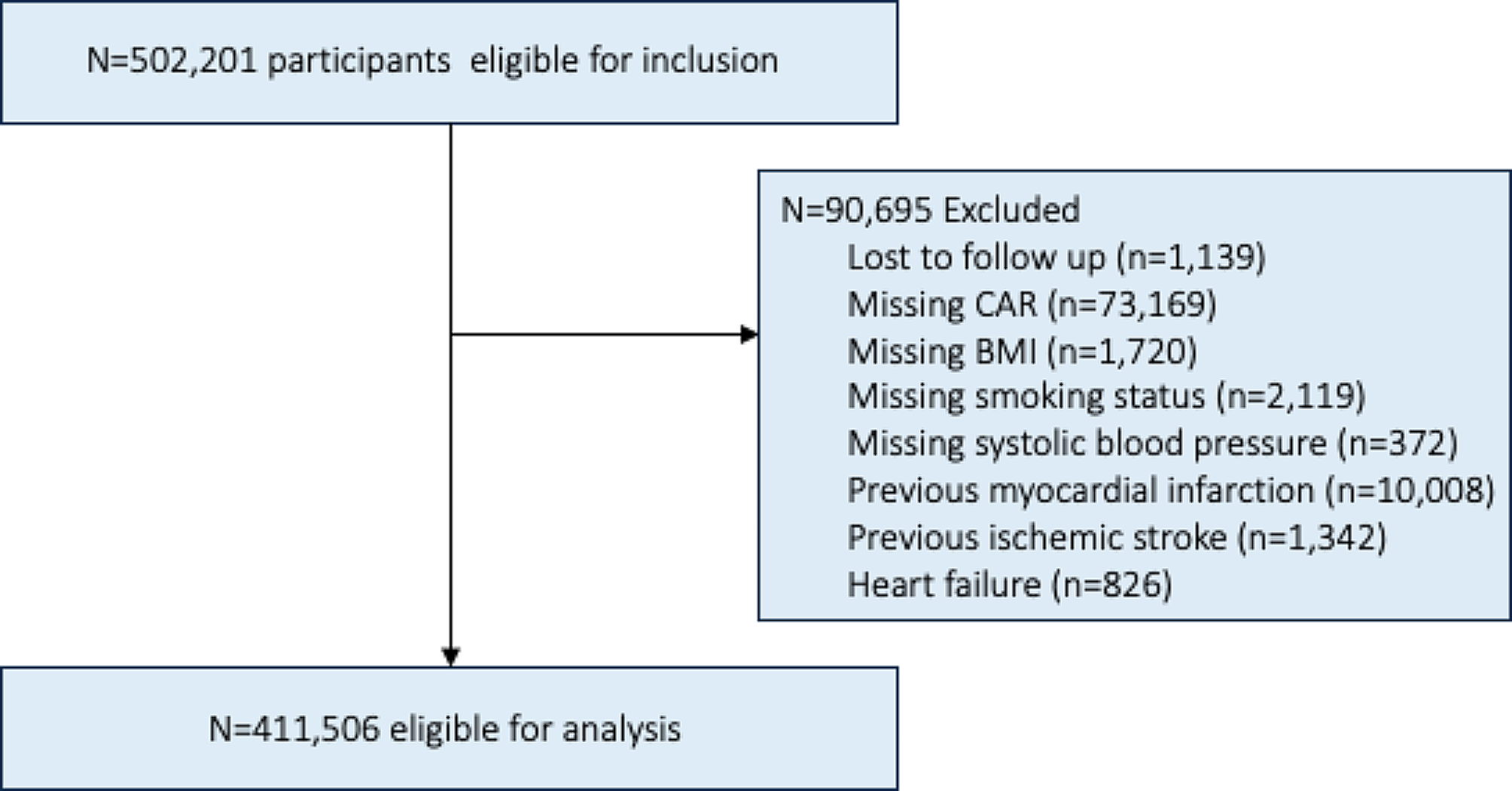
Individuals who withdrew their informed consent were consistently excluded from the UK Biobank, thus no count of their figures is available. Additionally, participants were excluded from this study if coded as lost to follow-up, had missing data on CAR, or lacked covariate information for body mass index (BMI), blood pressure, or smoking status. Furthermore, individuals who had experienced either a myocardial infarction (n = 10,008), ischemic stroke (n = 1,342), or had a diagnosis of heart failure (n = 826) were excluded (see Fig. 1). This study was carried out within the UK Biobank project 81508 and was approved by the Swedish Ethical Review Authority (2019–02328 and 2021-05762-02). Informed consent was obtained from all subjects and/or participants.
Fig. 1
Flowchart showing the road to inclusion. BMI (Body Mass Index), CAR (C-reactive Protein/Albumin Ratio)
Assessment of covariate dataSmoking status in the UK Biobank was assessed through a questionnaireFootnote 1. In the present study, individuals were categorized as never smokers, former smokers, or current smokers. Individuals who chose the ‘prefer not to answer’ option regarding their smoking status were excluded. Pack years of smoking were determined using the formula: number of years smoked multiplied by the average number of cigarettes smoked per day divided by 20. In instances where pack years of smoking were not available, the mean value for the corresponding smoking status category and sex was utilized as a substitute (n = 54,045 for previous smokers and n = 9,118 for current smokers).
Physical activity levels in the UK Biobank were assessed using a questionnaireFootnote 2. In the present study, individuals were categorized into one of three groups: sedentary, light, or high activity. This classification was based on the types of physical activities reported during the last four weeks. If data were missing, or if individuals were unsure, unwilling to respond, or only engaged in ‘walking for pleasure,’ they were classified as sedentary. Those participating in activities such as swimming, cycling, fitness exercises, bowling, or light/heavy do-it-yourself activities were categorized as having light physical activity. Individuals engaged in strenuous sports were classified as having a high level of physical activity.
Individuals were categorized as having diabetes at baseline (comprising both type 1 and type 2 diabetes) if they met any of the subsequent criteria:
1.Having an ICD-10 code ranging from E100 to E149 or an ICD-9 code ranging from 2500 to 2509 before the date of examination.
2.Exhibiting HbA1c levels equal to or exceeding 48 mmol/mol.
3.Receiving treatment involving insulin, metformin, pioglitazone, glipizide, glimepiride, rosiglitazone, or a combination of these medications during the examination.
Systolic blood pressure was assessed while individuals were in a seated position, with the measurement taken on the left arm (or right if more feasible). The arm was positioned at the level of the heart. Following a deliberate period of five slow breaths, blood pressure was measured using an Omron 705 IT electronic blood pressure monitor (OMRON Healthcare Europe B.V., Kruisweg 577, 2132 NA Hoofddorp). Blood pressure was measured twice. In this study, we utilized the average value of these two measurements, considering only the first if the second measurement was unavailable.
Low-density lipoprotein (LDL)-cholesterol levels were determined using enzymatic protective selection analysis (Beckman Coulter AU5800) with blood samples collected during the baseline examination. In individuals where LDL-cholesterol data were absent (n = 379 for women and n = 357 for men), the mean value for the corresponding sex within the overall study cohort was used as a replacement.
Information regarding statin treatment was gathered through self-reported medical conditions. Individuals were categorized as “yes” if they reported using any of the following statin medications: Rosuvastatin, Atorvastatin, Pravastatin, Simvastatin, Fluvastatin, Pitavastatin, and Lovastatin, or if the medication code or trade name corresponding to these statins was provided.
CRP levels were determined using high sensitivity immunoturbidimetric analysis on a Beckman Coulter AU5800. Albumin levels were measured through BCG analysis on the same instrument. CAR was calculated using the formula CRP/Albumin.
OutcomesThe UK Biobank database encompasses detailed information on the occurrence and advancement of various diseases, alongside dependable data regarding mortality and causes of death. Its reliability and precision are fortified by seamless integration with national health registries, ensuring comprehensive coverage and minimizing the risk of loss to follow-up.
In this study, the definitions for cardiovascular mortality, myocardial infarction, ischemic stroke, and heart failure were based on specific diagnostic codes from the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10). Cardiovascular mortality was defined as individuals with a cause of death recorded with ICD-10 codes I00-I99. Myocardial infarction, including both non-ST-elevation myocardial infarction (NSTEMI) and ST-elevation myocardial infarction (STEMI), was recorded from inpatient hospital data. Additionally, individuals with ICD-10 codes I210-I214 and I219 were included in the definition of myocardial infarction. Ischemic stroke cases were identified using ICD-10 codes I630-I639 and I693. Heart failure cases were identified using ICD-10 codes I500-I509. The individuals were censored at the occurrence of the first event for each outcome, more specifically within the analysis pertaining to that particular outcome. If no event occurred, a predefined end date was utilized, which corresponded to the latest recorded occurrence of any adverse outcome within the dataset, i.e., November 12, 2021.
Statistical analysisA multivariable Cox proportional hazard model was utilized to investigate the relationship between CAR or CRP and the occurrence of five specific outcomes: overall mortality, cardiovascular mortality, myocardial infarction, ischemic stroke, and heart failure. The multivariable model incorporated a range of covariates, comprising age, sex, BMI, smoking status (never, former, and current), level of physical activity, systolic blood pressure, LDL cholesterol, statin treatment, baseline diabetes, and prior history of myocardial infarction, ischemic stroke, and heart failure. For the Cox analysis focusing on heart failure, individuals were excluded if they had a documented history of heart failure at baseline, given its chronic nature. Standardization was applied to both CAR and CRP due to their non-normal distribution, resulting in a mean value of zero. This approach ensures comparability and facilitates interpretation of the results. We finally analysed in individuals with high and low CRP using the cutoff of 10 mg/ml to see if any difference between CAR and CRP could be seen in individuals with low grade inflammation or more acute inflammation or infection could be detected [18].
Data management and statistical analyses were performed using Stata/SE 15.1 for Mac (StataCorp, TX, USA).
留言 (0)