
記住我
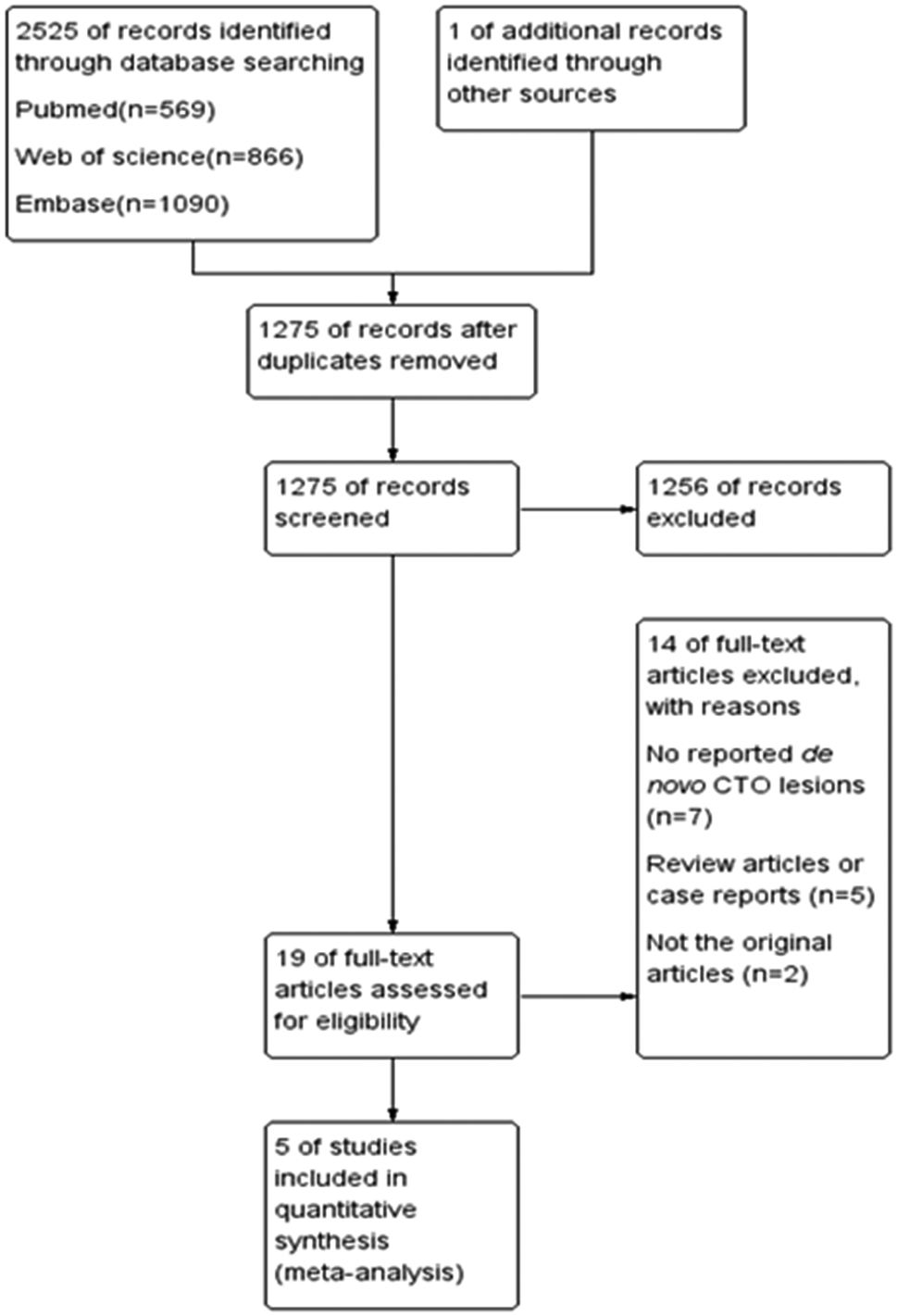

The medical records of 1032 patients after PBMV were reviewed. Seventy-six patients were excluded due to acute major complications during the first 24 h after PBMV (32 patients developed tamponade, and 44 patients underwent surgical mitral valve replacement due to valve rupture and severe MR). Of the remaining 956 patients, 80 patients were excluded due to lack of follow-up. Finally, 876 patients were included in our analysis (Fig. 1). The median age of the patients was 46.0 [28–64] years, and 81.1% of the patients (n = 710) were females. Among participants, 333 patients (38.0%) had a Wilkins score of 8 or less were included in group I, 501 patients (57.2%) had a Wilkins score of 9 or 10 and were assigned to group II, and 42 patients (4.8%) with a score greater than 10 were classified as group III. Median Wilkins score was 9 [8.5–9.5] in the overall population. Additionally, 175 (20%) patients had CC prior to PMV, from which 95 (10.8%) were on the anterolateral commissure, 64 (7.3%) were on the posteromedial commissure, and the remaining 16 had bicommissural calcification on mitral valve leaflets. Baseline characteristics and echocardiographic measurements of patients based on Wilkins score and CC are summarized in Table 1. There was a significant difference in Wilkins score between patients with and without CC (P < 0.001) (Fig. 2).
Fig. 1
Retrospective Cohort study flowchart
Table 1 Baseline Characteristics and Echocardiographic Parameters of the StudyFig. 2
Wilkins score based on the presence or absence of CC. Box and whiskers represent the distribution of the Wilkins score in patients with and without CC. Dots represent the actual value of Wilkins score for each patient. CC: commissural calcification
At baseline, there was no significant difference in MVA, MVAI, PAP, mean LA pressure and LVEF between patients with and without CC (all P > 0.05). However, there was a significant difference in MVA, MVAI, and PAP among Wilkins score groups, with patients in Wilkins group III having lower MVA and MVAI and higher PAP compared to the other groups (P < 0.001, P = 0.003, and P = 0.002, respectively).
In the short-term and mid-term echocardiographic evaluation following the PBMV, MVA increased significantly compared with baseline measurements in total cohort (baseline: 0.9 [0.8-1.0]; short-term: 2.4 [2.2–2.6]; mid-term 2.1 [2.1–2.1]; both p < 0.0001).
Mitral regurgitation at short-term follow upAt the 6-month follow-up, 246 (28.1%) patients had symptomatic significant MR. The prevalence of symptomatic significant MR was 65 (37.1%) in patients with CC and 181 (25.8%) in those without CC (P = 0.003) in short-term follow up (Fig. 3A). Among Wilkins score groups, 93(27.9%) patients in group I, 136 (27.1%) patients in group II, and 17(40.5%) patients in group III developed symptomatic significant MR in short-term follow-up (P = 0.182) (Fig. 3B).
Fig. 3
Figure 3 A-D Occurrence of short-term MR based on presence or absence of CC(3 A) and Wilkins Score (3B), and mid-term MR based on presence or absence of CC (3 C) and Wilkins Score (3D)
A univariable binary logistic regression revealed that patients with CC had significantly higher odds of experiencing short-term moderate and severe symptomatic MR that led to MVR (OR: 1.69, 95%CI 1.19–2.41, P = 0.003). This model explained 1.4% (Nagelkerke R2) of the variance in significant symptomatic MR incidence. In a multivariate logistic regression adjusted for age, sex, MVAI, PAP, and LVEF (X2 [6] = 49.11, P < 0.001), CC remained significantly associated with higher odds of short-term symptomatic significant MR (OR: 1.65, 95%CI: 1.15–2.37, P = 0.006). This model explained 7.4% (Nagelkerke R2) of the variance in MR at mid-term follow-up.
On the other hand, Wilkins groups II and III did not show significantly higher odds ratios for predicting short-term MR compared to group I (group II: OR: 0.96, 95%CI: 0.70–1.31, P = 0.784; group III: OR: 1.75, 95%CI: 0.90–3.39, P = 0.098).
Mitral regurgitation at mid-termAt two years follow up, hundred and twenty-six (14.4%) patients had significant symptomatic MR that led to MVR. (Fig. 3C). There was a significant difference in the prevalence of MR in mid-term evaluation between patients with and without CC (CC: 54 (30.9%); no CC: 72 (10.3%), P < 0.001). Although there was an incremental increase in the prevalence of MR in mid-term follow up among Wilkins groups I through III, this difference was not statistically significant (group I: 41 (12.3%); group II: 77 (15.4%); group III: 8 (19%), P = 0.317) (Fig. 3D).
In univariable binary logistic regression analysis, Wilkins groups II and III had higher odds of developing MR in mid-term, however these differences were not statistically significant (group II: OR:1.29, 95%CI: 0.86–1.94, P = 0.216; and group III: OR: 1.68, 95%CI: 0.73–3.87, P = 0.227). In contrast, CC was significantly associated with higher odds of MR incidence at mid-term follow-up in univariate (OR: 3.90, 95%CI 2.61–5.83, P < 0.001), as well as multivariate model adjusted for age, sex, MVAI, PAP, and LVEF (X2 [6] = 49.11, OR: 3.78, 95%CI: 2.52–5.68, P < 0.001). Univariate and multivariate models could predict 8.2% and 9.7% (Nagelkerke R2) of the variation in MR occurrence at mid-term follow-up, respectively.
Mitral valve restenosis at mid-term follow-upMitral valve restenosis occurred in 45 (5.1%) patients during the 24-month follow-up. There was no significant difference in the prevalence of restenosis among patients with and without CC (CC: 13 (7.4%), no CC: 32 (4.6%), P = 0.125) (Fig. 4A). However, a significant difference in restenosis was observed among Wilkins score categories (P = 0.016). Patients in Wilkins group III had the highest occurrence rate of restenosis, followed by group II, and patients in group I had the lowest rate of restenosis (group III: 3 (7.1%), group II: 34 (6.8%), and group I: 8 (2.4%)) (Fig. 4B).
Fig. 4
4A and 4B Occurrence of mitral valve restenosis based on presence or absence of CC (4A) and Wikins score (4B)
Binary logistic regression was used to examine the effects of Wilkins categories and CC on restenosis incidence at follow-up. While patients with CC showed higher odds of experiencing restenosis, this difference was not statistically significant (OR: 1.68, 95%CI: 0.861–3.27, P = 0.128).
The univariate model for Wilkins score was statistically significant (X2(df = 2) = 9.18; P < 0.001). In comparison to group I, the odds of experiencing restenosis in follow-up were significantly higher for group II (OR: 2.96,95%CI: 1.35–6.27, P = 0.007). However, the odds for group III, while elevated, did not reach statistical significance (OR: 3.13, 95%CI: 0.80-12.27; P: 0.103). In multivariable logistic regression model adjusted for age, sex, MVAI, PAP, and LVEF (X2 [7] = 14.52, P = 0.043), Wilkins group II still had significantly higher odds for developing restenosis (OR: 2.97, 95%CI: 1.35–6.55, P = 0.007). Patients in Wilkins group III had higher odds of having restenosis compared to group I, however this difference was not statistically significant (OR:3.49, 95%CI: 0.85–14.26, P:0.082).
留言 (0)