Study design and data
This study was a secondary analysis of the multicenter retrospective cohort study, the Study of Advanced life support for Ventricular fibrillation with Extracorporeal circulation in Japan II (SAVE-J II) in Japan. Thirty-six institutions in Japan participated in this registry. This multicenter study was pre-registered at the Japanese clinical trial registry (registration number: UMIN000036490) [20], and approved by the institutional review board of Kagawa University (approval number: 2018-110) and each participating institution. Owing to the retrospective study design, informed consent was not required. However, patients were given the opportunity to opt out of the study at any time by withdrawing permission to use their data. To ensure patients’ right to refuse participation, the methods of utilizing patient information were disclosed on the websites and notice boards of each participating institution.
SAVE-J II included all patients aged ≥ 18 years who were admitted to the emergency department for OHCA and underwent ECPR between January 1, 2013 and December 31, 2018. In this registry, ECPR was defined as resuscitation for cardiac arrest using veno-arterial ECMO. The exclusion criteria were patients with in-hospital cardiac arrest and refusal to participate in the study communicated by the patients themselves, family, or others. The following data were collected: patient characteristics, prehospital information, information on hospital arrival, diagnosis, interventions, mechanical support information, time course, and outcomes [21].
Study population and data collection
We included all patients of the SAVE-J II study. The exclusion criteria of this secondary analysis were as follows: return of spontaneous circulation before ECMO pump on; transfer from another hospital; and missing data on outcomes (survival to hospital discharge and cerebral performance category [22] at hospital discharge), low-flow time, body temperature at hospital arrival, and covariates, as mentioned below.
The following patient data were used for this secondary analysis: age, sex, location of cardiac arrest (home, public space, or ambulance), witnessed cardiac arrest, bystander CPR, initial cardiac rhythm (shockable or unshockable) at the scene and at hospital arrival, body temperature at hospital arrival, the detailed time course of resuscitation, survival to hospital discharge, and cerebral performance category at hospital discharge. Initial shockable rhythm was defined as ventricular fibrillation, pulseless ventricular tachycardia, or rhythm for defibrillation in an automated external defibrillator used by emergency medical staff.
Variables of interest
The variables of interest were body temperature at hospital arrival and low-flow time. Body temperatures were measured at the body surface or core body temperature, which were not recorded in this registry. Following the previous studies on AH [9, 23], we defined AH as body temperatures < 32 °C.
Low-flow time was defined as follows: (i) the duration from cardiac arrest to the establishment of ECPR when the cardiac arrest occurred in the ambulance, (ii) the duration from the call for an ambulance to the establishment of ECPR when the cardiac arrest occurred before ambulance arrival with bystander CPR, or (iii) the duration from the arrival of emergency medical service to the establishment of ECPR when the cardiac arrest occurred before ambulance arrival without bystander CPR.
Outcomes
The primary outcome was survival at hospital discharge. The secondary outcome was favorable neurological outcome, defined as a cerebral performance category of 1 or 2 at hospital discharge.
Statistical analysis
Categorical variables were counted and presented as proportions. Continuous variables were expressed as medians and interquartile ranges.
First, we compared the baseline characteristics and outcomes using the Wilcoxon rank-sum test for continuous variables and the Chi-square test for categorical variables.
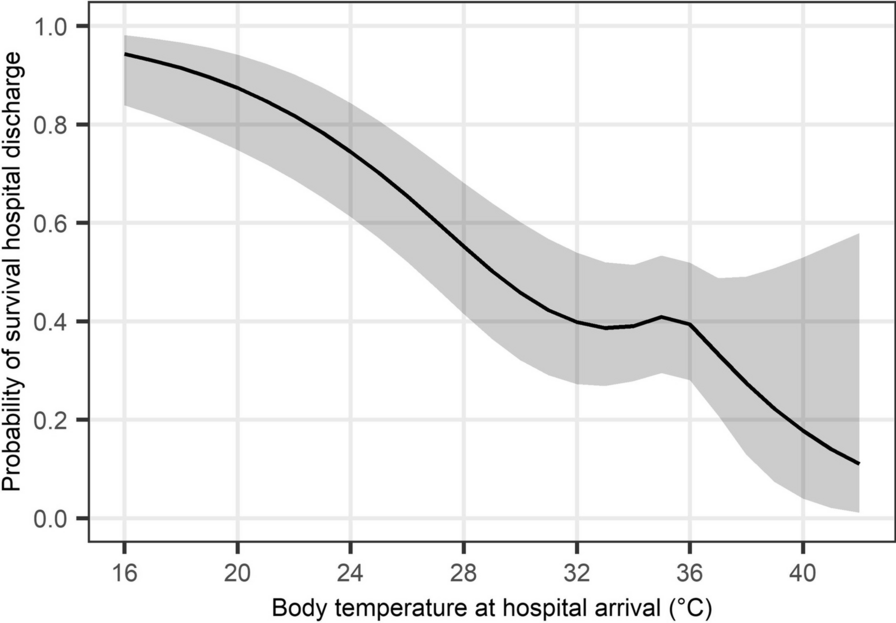
Next, we examined the non-linear associations between body temperature at hospital arrival and outcomes for all eligible patients using restricted cubic spline analyses [24]. We set four knots in the cubic splines, placed on the fifth, 35th, 65th, and 95th percentile of body temperature [25]. We adjusted for age, sex, the location of cardiac arrest, witnessed cardiac arrest, bystander CPR, the initial cardiac rhythm at the scene and upon hospital arrival and low-flow time. We calculated the adjusted outcomes and their 95% confidence intervals (CIs) for each value of body temperature.
Then, we examined the non-linear associations between low-flow time and outcomes using restricted cubic spline analyses stratified by the presence or absence of AH (hypothermia defined as body temperature below 32 °C). We set four knots in the cubic splines, placed on the fifth, 35th, 65th, and 95th percentiles of low-flow time. We adjusted for age, sex, location of cardiac arrest, witnessed cardiac arrest, bystander CPR, and the initial cardiac rhythm at the scene and upon hospital arrival. We calculated the adjusted outcomes and their 95% CIs for each value of low-flow time.
Finally, we stratified the patients into two groups according to the cut-off value of low-flow time. Since a method has not been universally accepted for determining the cut-off value, we defined a new method in this study to assess the association between low-flow time and outcomes in patients with AH and compared them with those of patients without AH. We defined the cut-off value based on the qualitative assessment of the appearance of the restricted cubic spline curves on the survival discharge rate. Then, we investigated whether the presence of AH had interactions on the association between low-flow time and outcomes by performing multivariable logistic regression analyses for the outcomes with the category of low-flow time (short or long), the presence of AH, their interaction term, and same covariates adjusted in the restricted cubic spline analyses. The odds ratios (ORs) and their 95% CIs on outcomes were calculated for each body temperature group with respect to the reference group with long low-flow time.
As a sensitivity analysis, with the definition of AH as below 28 °C instead of below 32 °C, we examined the non-linear association between low-flow time and outcomes and investigated whether AH had interactions on the association between low-flow time and outcomes in the same way as in the main analysis. AH was defined as a body temperature below 28 °C because the risk of cardiac arrest increases substantially if the core temperature drops below 28 ℃ [1], and severe hypothermia is usually defined as a core temperature below 28 ℃ [26].
Statistical analyses were performed using STATA/BE 17.0 software (StataCorp, College Station, TX, USA) and R 4.3.1 software (R Foundation for Statistical Computing, Vienna, Austria).



留言 (0)