According to the Guidelines (S3-Leitlinie Kolorektales Karzinom 2019), the colorectal carcinoma is with an incidence of more than 64,000 and a death toll of 26,000 a year the prevalent malignant tumor in Germany [9]. Colonoscopy is by far the most sensitive and specific method to detect colorectal neoplasia and therefore is recommended as a gold standard.
Removal of polyps before they develop to a carcinoma can significantly reduce the rates of colorectal carcinoma [10]; however, there is a misrate in lesions which are not detected within colonoscopy (5%) in high-risk patients up to 66%. Often, it is the flat polyps and adenomas which are missed. That is why Jung et al. point out not only the importance of follow-up colonoscopies but also the necessity of technical improvements.
For the esophagus, there are studies that directly compare the methods of EMR and ESD in the removal of superficial esophageal cancer (SEC). It shows a higher success rate in the removal of lesions < 2 cm regarding the en bloc resection as well as the curative resection rate for ESD. However, ESD takes much more time than EMR and has a higher risk potential. Comparing the rate of bleedings, no difference is seen; however, the ESD shows a higher rate of perforations [11].
While there are promising developments on the technical side of flexible endoscopy like new resection instruments [12, 13], we think that the results of resection can be improved by choosing an optimized injection solution.
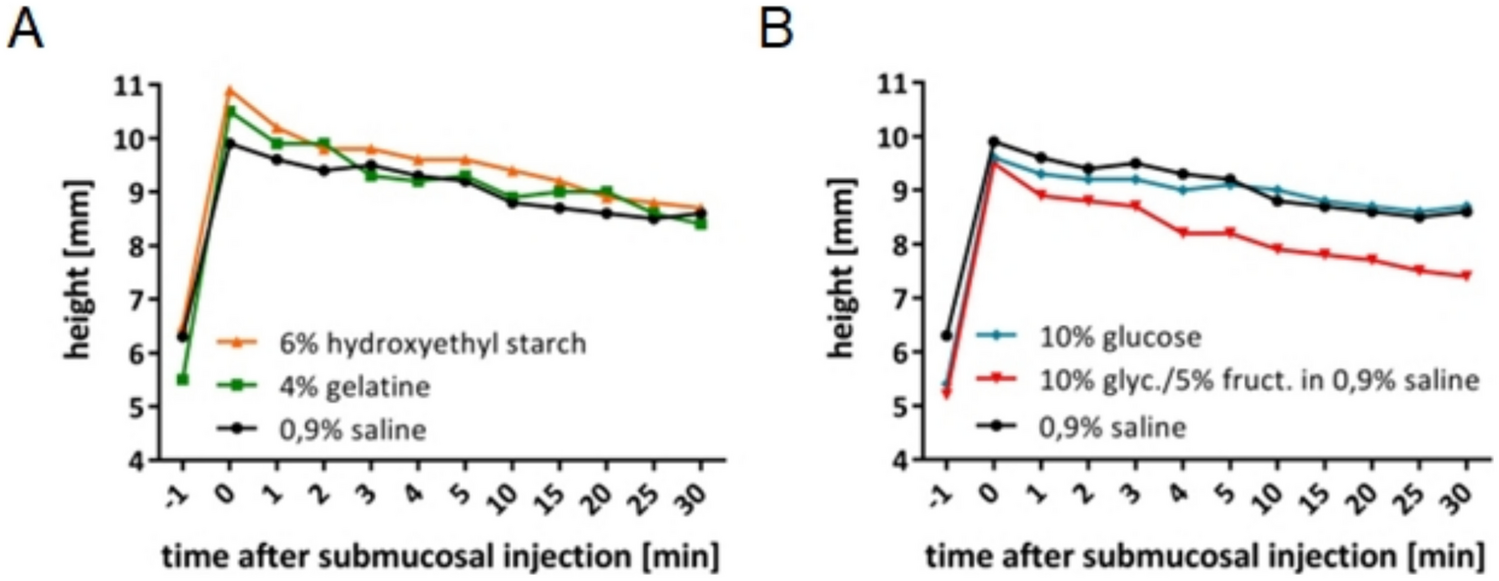
The commonly used injection solution is 0.9% NaCl. That is why in most studies 0.9% NaCl is used as standard injection solution. Studies show that 0.9% NaCl gives a good initial elevation which then declines relatively fast compared to, e.g., 10% glycerin/5% fructose solution [5, 7]. In vitro a longer lasting elevation of 10% glycerin/5% fructose solution compared to 0.9% NaCl is shown in human tissue [7] but cannot be seen in porcine tissue (1 ml) [5] and the effect of better results for an en bloc resection is limited to lesions < 2 cm. The same holds true for most tested glucose solutions; however, due to the high osmolarity of these solutions (glucose > 15%), tissue damages can be observed [5, 7]. This is why in this study glucose solutions of 6% have been used.
Other studies used the Hydro-Jet technique to inject 5 ml 4% gelatine, 10% hydroxyethl starch, and 50% glucose solution compared to 0.9% NaCl in vivo in pigs that showed a higher elevation and a slower decline for hydroxyethyl starch and glucose solution. A snare-resection afterwards was performed without problems [6].
Our work shows no significant difference in height and duration of the elevation within all tested solutions. These varying findings show the dependence of the results from the kind of tissue, technique, and volume of injection solution that is used.
There are other studies that discuss the usage of autogenic blood as injection solution. Compared to 0.9% NaCl, it shows higher and longer lasting elevations; it is available and very cost effective, but it can lead to blood coagulation and impaired sight during the procedure [8, 14].
In this work, for the first time, the specific impedances of surface and tissue after injection of various solutions were analyzed and compared regarding the laws of every RF surgical cutting process. It clearly shows that aqua destillata and 10% glucose, to a lesser content also autogenic blood, lead to significantly higher impedances and therefore can optimize the electrosurgical cutting results. These results should be respected in further research in RF surgery as well as in clinical practice, especially for larger lesions or in critical situations. If a problem with the cut occurs during a procedure a low-impedance solution could be injected additionally to 0.9% saline solution. Other tested solutions did not show any significant differences regarding their impedance and are at the same level than the standard solution.
In accordance to our hypothesis, these solutions did not show any better results in the cutting process at lesions > 2 cm (data not shown).
Our findings underscore the significance of comprehensively understanding the electrosurgical cutting process, particularly in critical cases, and emphasize the role of impedance as a crucial factor for achieving the necessary voltage for cutting. Further research in this area is imperative for enhancing safety and reducing the risk of bleeding or even perforation. We think our research illuminates the potential for innovation in conventional resection techniques like polypectomy and EMR, as well as in advanced methods such as ESD and ESR. Prioritizing impedance considerations could be the beginning of a new field of research, one that merits attention not only in research but also in everyday clinical practice, by ensuring safety for patients by mitigating risks of RF surgery.

留言 (0)