
記住我



Nearly one-third of patients with diffuse large cell lymphoma present with extra nodal involvement.1 The most frequent site of involvement is the gastrointestinal tract, more specifically the stomach and intestines.2 Primary pancreatic involvement is a rarity as it accounts for less than 2% of all lymphomas and approximately 0.5% of all pancreatic lymphomas.3 Pancreatic involvement may be misdiagnosed as a pancreatic cancer, which can lead to incorrect therapeutic management. Previously, pancreatic tissue was only able to be obtained by percutaneous biopsy or exploratory laparotomy, but recent studies have shown that although difficult, fine-needle aspiration (FNA) can make the diagnosis of a pancreatic lymphoma.3 Lymphomas can show different patterns of pancreatic involvement. The most common is the nodular, hypodense lesion at radiological investigations. The most common histotypes of pancreatic involvement are non-Hodgkin or diffuse large B-cell.4
We report the utility of endoscopic ultrasound (EUS) in a patient who underwent a repeat EUS to diagnose the transformation of follicular lymphoma to large cell lymphoma with pancreatic involvement.
CASE REPORTA 70-year-old man with a history of tobacco abuse initially presented with a greater than 1 year history of a right shoulder mass that increased in size. He was evaluated by general surgery, and the mass was excised in 2016 with biopsies demonstrating B-cell non-Hodgkin lymphoma with germinal center phenotype, which stained positive for CD45, CD20, PAX4, CD10, bcl-6, bcl-2, and CD23. He then had a positron emission tomography-computed tomography (PET-CT) demonstrating enlarged lymph nodes in the peripancreatic, retroperitoneal, and mesenteric locations along with focal uptake in the ileocecal valve. As a result, he underwent a colonoscopy with pathology consistent with follicular B-cell lymphoma. He was treated with maintenance rituximab.
While undergoing chemotherapy, 2 years later, he began having hearing loss after sustaining a dog bite to his left nostril. Magnetic resonance imaging noted a left palatine tonsillar mass. As a result, he underwent a laryngoscopy/esophagoscopy/bronchoscopy with biopsy, which demonstrated invasive squamous cell carcinoma with immunostaining positive for P16 consistent with human papilloma virus positivity. He subsequently underwent left neck dissection and transoral robotic left tonsillectomy with weekly cisplatin and beam radiation for 6 weeks.
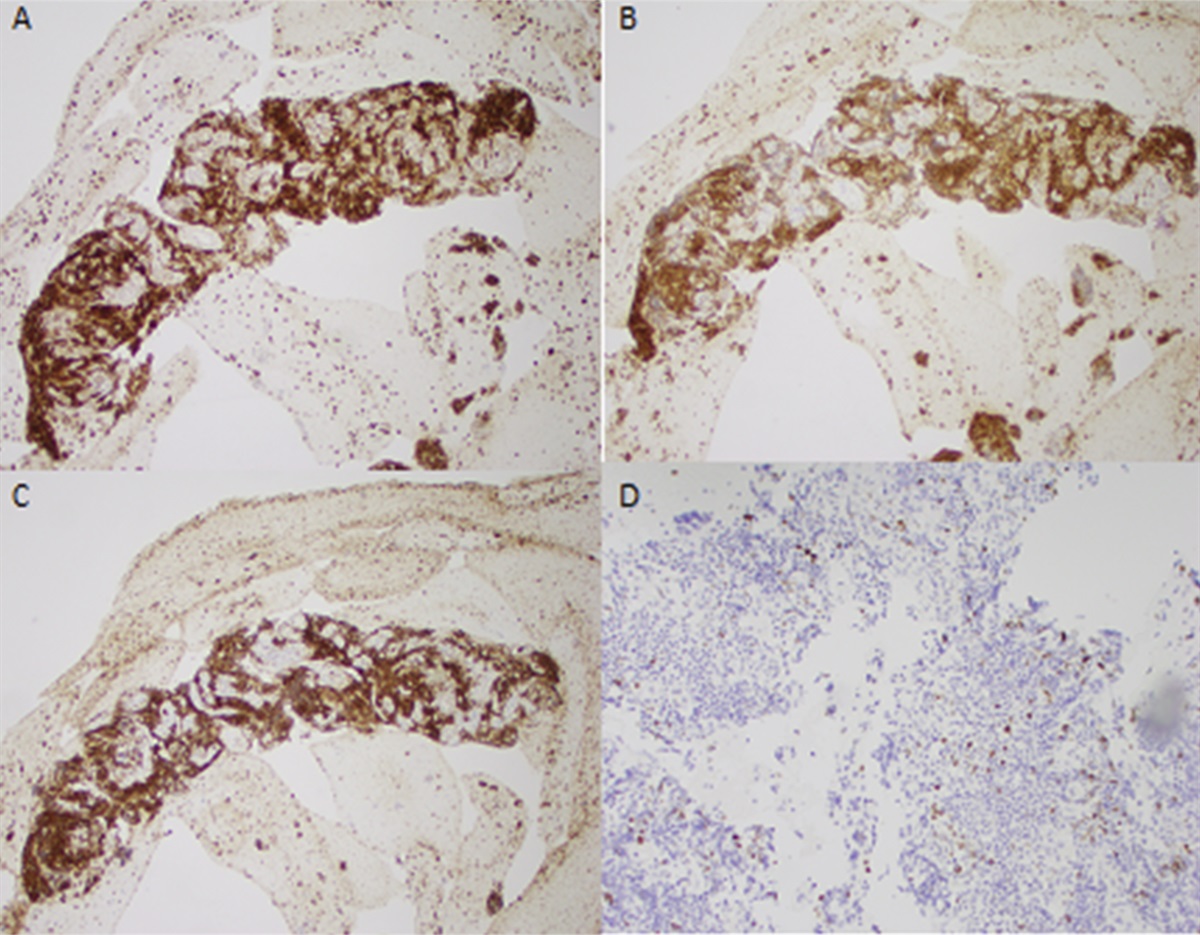
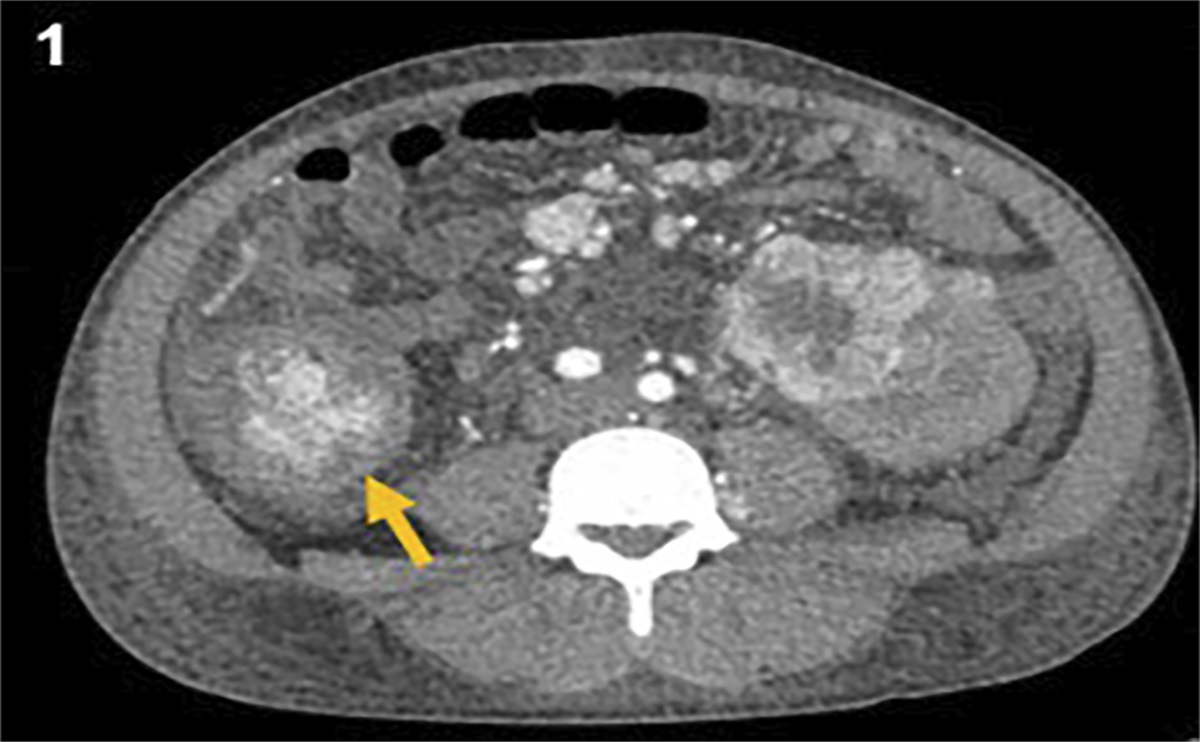
Five years after the initial diagnosis, he underwent more episodes of chemotherapy for his residual lymphoma and a follow-up PET-CT demonstrated a matted mass-like lymphadenopathy involving small bowel mesentery and new uptake in the body of the pancreas. An esophagogastroduodenoscopy/EUS with FNA demonstrated gastritis with a mass adjected to the pancreatic body concerning for lymphoma. The biopsy of the pancreatic lesion noted CD10+ lymphoma with atypical cells positive for CD20, PAX5, CD10, BCL2, and BCL6 (Figure 1).
 Figure 1.:
Figure 1.: (A) BCL 2, (B) CD10, (C) CD20, (D) Ki67.
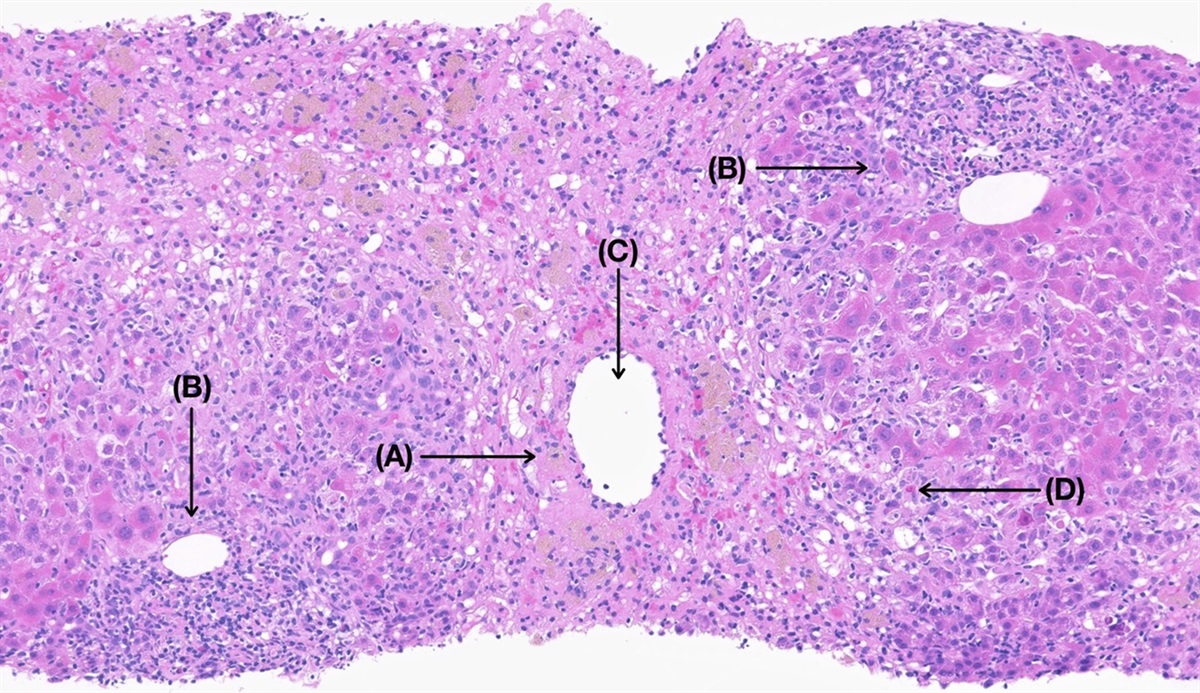
After another 2 years, a follow-up PET-CT showed a mass like-adenopathy abutting the pancreatic body. He then underwent a repeat esophagogastroduodenoscopy/EUS with FNA to re-evaluate the pancreatic mass and guide further chemotherapy. It demonstrated normal esophagus, normal stomach, and normal duodenum. Biopsies of the peripancreatic adenopathy noted CD10+ large B-cell lymphoma favoring follicular lymphoma with large cell transformation. Flow cytometry noted B-cell lymphoma CD5-/CD10+ compatible with high grade/large B-cell lymphoma. Compared with the prior biopsy, the current tumor cells showed larger sizes and higher KI67, further supporting the follicular to large cell transformation (Figure 2).
 Figure 2.:
Figure 2.: (A) BCL2, (B) CD10, (C) CD20, (D) Ki67.
As a result of these findings, oncology induced the patient on fludarabine/cytoxan and later with axicabtagene ciloleucel infusion. A follow-up PET-CT 1 month after the beginning of infusion showed a decrease in size and metabolic activity of the abutting pancreatic lesion.
DISCUSSIONEUS with FNA has been shown to play an important role in diagnosing pancreatic cancers.3 It provides detailed radiologic information with utmost importance to vascular and lymph node involvement by pancreatic malignancies. In our case, the utility of EUS with FNA allowed us to track the transformation of this patient's follicular to large B-cell lymphoma. Furthermore, its utility allowed oncology to guide treatment options which resulted in the patient being started on a new therapy.
Follicular lymphoma is the second most common type of non-Hodgkin lymphoma. Its transformation to an aggressive lymphoma typically occurs at a rate of 2% to 3% each year. Furthermore, it is associated with rapid progression, treatment resistance, and a poor prognosis.5 Typically, pancreatic lymphomas occur in the pancreatic head.6 Our patient's lesion was in the pancreatic body. The primary novelty of this case lies primarily in the utility of EUS with FNA. Literature review shows no reported cases of EUS with FNA being done twice on the same patient demonstrating the transformation/progression of his or her lymphoma.
In addition, the skill of the advanced endoscopist also cannot be understated. There have been multiple cases of difficulty diagnosing pancreatic lymphomas. While the procedure is more cost-effective and safer than percutaneous biopsy, it is a difficult procedure with mixed success rates. There have been reports of difficulty trying to diagnose diffuse large B-cell lymphomas. Upon literature review, 2 cases reached a diagnosis only after the EUS-FNA session and one case failed to reach a conclusive diagnosis despite finding atypical lymphocytes.7,8 Furthermore, neither of those cases demonstrated surveillance of the same patient's transformation to a large B-cell lymphoma.
Pancreatic malignant lymphomas are unusual solid tumors that are characterized as being nonepithelial neoplasms. While primary pancreatic lymphoma is a rare finding, secondary pancreatic involvement occurs in up to 30% of patients. This case demonstrated the utility of FNA in 2 important aspects of patient care. First, it allowed us to see the transformation of this patient's follicular lymphoma to large B-cell lymphoma. Second, it was used to guide treatment management in this patient which was crucial as he had an excellent response to the new therapy.
DISCLOSURESAuthor contributions: R. Patel: lead writer, lead investigator and guarantor; E. Bley and CJ Foster: editors and guidance of the case; S. Patel: analyzed pathology slides.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Castillo JJ, Winer ES, Olszewski AJ. Sites of extranodal involvement are prognostic in patients with diffuse large B-cell lymphoma in the rituximab era: An analysis of the surveillance, epidemiology and end results database. Am J Hematol. 2014;89(3):310–4. 2. Saif MW. Primary pancreatic lymphomas. JOP. 2006;7(3):262–73. 3. Chang KJ. State of the art lecture: Endoscopic ultrasound (EUS) and FNA in pancreatico-biliary tumors. Endoscopy. 2006;38(Suppl 1):56–60. 4. Khashab M, Mokadem M, DeWitt J, et al. Endoscopic ultrasound-guided fine-needle aspiration with or without flow cytometry for the diagnosis of primary pancreatic lymphoma - a case series. Endoscopy. 2010;42(3):228–31. 5. Fischer T, Zing NPC, Chiattone CS, Federico M, Luminari S. Transformed follicular lymphoma. Ann Hematol. 2018;97(1):17–29. 6. Okamoto T, Sasaki T, Nishimura N, et al. Pancreatic follicular lymphoma: A report of two cases and literature review. Clin J Gastroenterol. 2021;14(6):1756–65. 7. Savari O, Al-Duwal Z, Wang Z, Ganesan S, Danan-Rayes R, Ayub S. Pancreatic lymphoma: A cytologic diagnosis challenge. Diagn Cytopathol. 2020;48(4):350–5. 8. Kopel J, Swarup K, Thein K, Swarup S. Primary B cell lymphoma of the pancreas. J Gastrointest Cancer. 2020;51(3):1077–80.
留言 (0)