
記住我



Barrett's esophagus (BE) is a premalignant condition that develops as a result of long-standing gastroesophageal reflux disease (GERD), which leads to transformation of the normal distal esophageal squamous mucosa to be replaced by a specialized metaplastic columnar mucosa.1 In GERD, the esophagogastric junction barrier is incompetent in preventing reflux of gastric contents back into the esophagus.2 By contrast, achalasia is characterized by failure of the lower esophageal sphincter (LES) to relax with swallowing and absence of normal peristalsis, impeding passage of liquids and solids from the esophagus to the stomach.3 Given that BE is a consequence of chronic GERD and achalasia coincides with a tight LES preventing reflux, the presence of both pathologies is paradoxical and extremely rare.4 We describe a patient case with long-segment BE and simultaneous achalasia.
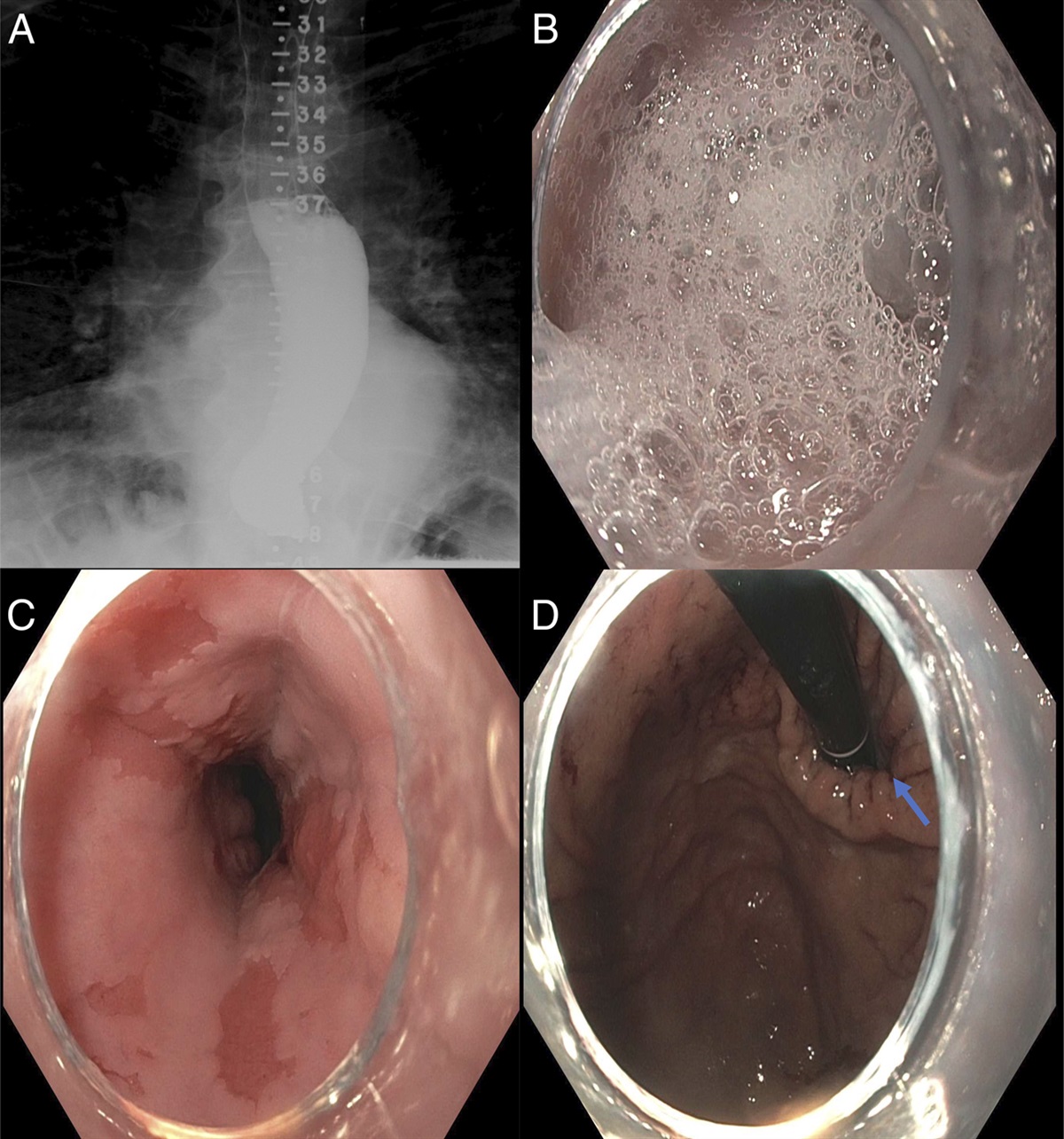
CASE REPORTA 73-year-old man with a history of GERD was referred to our clinic for further evaluation of achalasia. His predominant symptoms were dysphagia, regurgitation, and thick secretions/foam in his mouth. He reported being diagnosed with BE at least 10 years ago and achalasia 8 years ago (the patient confirmed being diagnosed with BE before he was diagnosed with achalasia. His achalasia was diagnosed based on endoscopic appearance, and no manometry was performed). Since then, his achalasia had been managed with LES botulinum toxin injection with symptom improvement lasting 6–12 months each time. During his last esophagogastroduodenoscopy (EGD) 6 months before his presentation, he underwent balloon dilation to 18 mm in addition to LES botulinum toxin injection. During the same EGD examination, he was found to have a 4 cm long BE with biopsies revealing intestinal metaplasia. His Eckardt score was 7/12 on presentation to our center.5 A timed barium esophagram showed a 10 cm column while drinking the contrast (Figure 1) but cleared by 2 minutes. His EGD at our institution showed dilated esophageal lumen, stasis changes, and excessive amount of retained foam and narrowed distal esophagus with no significant resistance advancing the scope into the stomach (Figure 1). He was also found to have 4 cm salmon-colored mucosa (circumferential length: 0 cm, maximal length: 4 cm C0M4 per Prague classification) in addition to scattered islands above the area (Figure 1).6 A small 2 cm hiatal hernia (HH) was also noted. Pathology from pinch biopsies showed specialized intestinal metaplasia, consistent with BE. Functional lumen imaging probe during the same endoscopic examination showed absent esophageal contractility to volumetric distension with tight LES (distensibility index 1.8 mm2/mm Hg [normal >3 mm2/mm Hg] and esophagogastric junction diameter 8.3 mm at 60 mL fill volume, Figure 2).7 Subsequent high-resolution esophageal manometry was consistent with achalasia type II (Figure 2). He underwent laparoscopic HH repair with Heller myotomy and Dor fundoplication. The patient reported resolution of his symptoms during a follow-up visit 4.5 months later (Eckardt score 0/12).
 Figure 1.:
Figure 1.: (A) Timed barium esophagram showing a 10 cm column while drinking the contrast. The contrast cleared by 2 minutes, which is likely affected by recent LES botulinum toxin injection. (B) An endoscopic image showing an excessive amount of retained foam and thick secretions in the esophageal lumen. (C) An endoscopic view of Barrett's esophagus in the distal esophagus (circumferential length: 0 cm, maximal length: 4 cm). (D) A retroflexed endoscopic view showing the gastric cardia and a loose esophagogastric junction. Notice the gastric folds (arrow) going into the loose esophagogastric junction in the setting of dilated diaphragmatic hiatus and hiatal hernia.
 Figure 2.:
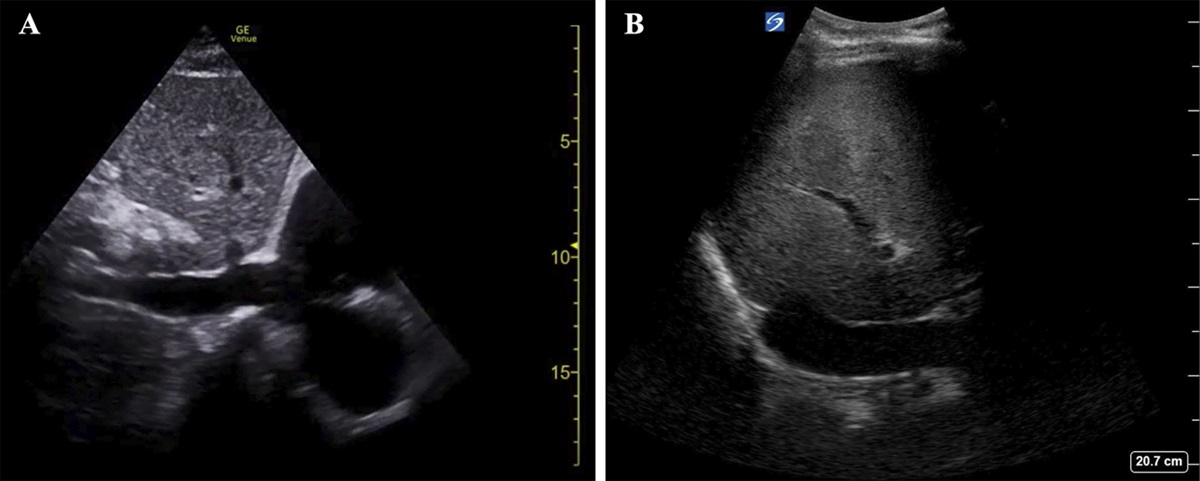
Figure 2.: (A) Functional lumen imaging probe showing a distensibility index of 1.8 mm Hg/mm2 and diameter of 8.3 mm at 60 mL fill volume. (B) Three representative swallows on high-resolution esophageal manometry showing panesophageal pressurization in the setting of achalasia type 2. The panesophageal pressurization bands are not homogeneous (as usually seen in achalasia type 2) since the patient was belching (black arrows) and preventing adequate esophageal pressurization after swallowing.
The patient's esophageal pinch biopsies obtained at our center were sent for a tissue system pathology test known as the TissueCypher assay to assess the risk of progression over 5 years, which returned as low risk (risk score: 5.2, probability of progression to high-grade dysplasia or adenocarcinoma over the next 5 years: 6%).8
DISCUSSIONFrom a pathophysiologic standpoint, GERD and achalasia are opposite conditions that may affect the esophagus. Although GERD is common with an estimated prevalence of 15.4% in North America, BE develops in only 5%–12% of patients with GERD.9 Achalasia is a rare disease with an estimated incidence of 2–3 per 100,000.10 Owing to their differing pathologic processes, BE and achalasia can be rarely encountered in the same patient. While chronic GERD is a known consequence of definitive achalasia treatment modalities aiming to disrupt the LES, which could then increase the risk of developing BE, coexistence of BE and untreated achalasia is extremely rare.4 In the case presented here, it appears that the patient developed BE from chronic GERD and later developed achalasia. Our case presents a challenging situation. Since the patient had HH and risk of reflux after POEM is higher than post-Heller myotomy with Dor fundoplication and since the patient had already developed BE, a consequence of long-standing GERD, we opted for Heller myotomy with HH repair and Dor fundoplication to decrease the possibility of significant reflux, which could theoretically increase the risk of BE progressing to esophageal adenocarcinoma.11 Despite HH repair and performing a partial Dor fundoplication after undergoing Heller myotomy, he is still expected to have GERD, although one would hope the volume of reflux is less with the HH repair and partial fundoplication. Now that his achalasia has been treated, we plan to monitor him closely for possible progression of his BE to esophageal adenocarcinoma. Going forward, we plan to perform annual endoscopic surveillance for both achalasia and BE, especially that his risk of progression may be higher now after LES myotomy and the theoretical increase in esophageal squamous carcinoma in the setting of achalasia.12 The result of TissueCypher would not have changed our management plan. In fact, the patient underwent Heller myotomy with HH repair and Dor fundoplication before the result of his TissueCypher was available. Although TissueCypher is reported as low risk based on a score of 5.2 (low risk if score <5.5), the probability of progression over the next 5 years is 6%, which is similar to progression rate of BE with low-grade dysplasia.13 Therefore, this is an additional factor supporting our intensive annual endoscopic surveillance plan. TissueCypher cannot be requested again on the same patient within 3–5 years unless there is a change in the baseline environment. In this case, since the patient underwent myotomy and potential worsening of his reflux, we plan to request TissueCypher again on his follow-up surveillance biopsies to assess for any change in his risk of progression.
DISCLOSURESAuthor contributions: C. Altfillisch and S. Samo: wrote the first draft of the manuscript. All authors reviewed and approved the final draft. S. Samo is the article guarantor.
Financial disclosure: S. Samo: Castle Biosciences-speaker's bureau, advisory board; Evoke-speaker's bureau; Sanofi-scientific program speaker, scientific advisory board; EndoGastric Solutions-speaker's bureau. Other authors declare no conflict of interest.
Informed consent was obtained for this case report.
REFERENCES 1. Shaheen NJ, Falk GW, Iyer PG, et al. Diagnosis and management of Barrett's esophagus: An updated ACG guideline. Am J Gastroenterol. 2022;117(4):559–87. 2. Katz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, Spechler SJ. ACG clinical guideline for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2022;117(1):27–56. 3. Vaezi MF, Pandolfino JE, Yadlapati RH, Greer KB, Kavitt RT. ACG clinical guidelines: Diagnosis and management of achalasia. Am J Gastroenterol. 2020;115(9):1393–411. 4. Guo J-P, Gilman PB, Thomas RM, Fisher RS, Parkman HP. Barrett's esophagus and achalasia. J Clin Gastroenterol. 2002;34(4):439–43. 5. Eckardt VF, Aignherr C, Bernhard G. Predictors of outcome in patients with achalasia treated by pneumatic dilation. Gastroenterology. 1992;103(6):1732–8. 6. Sharma P, Dent J, Armstrong D, et al. The development and validation of an endoscopic grading system for Barrett's esophagus: the Prague C & M criteria. Gastroenterology. 2006;131(5):1392–9. 7. Carlson DA, Gyawali CP, Khan A, et al. Classifying esophageal motility by FLIP panometry: A study of 722 subjects with manometry. Am J Gastroenterol. 2021;116(12):2357–66. 8. Duits LC, Khoshiwal AM, Frei NF, et al. An automated tissue systems pathology test can standardize the management and improve health outcomes for patients with Barrett's esophagus. Am J Gastroenterol. 2023;118(11):2025–32. 9. Fass R. Gastroesophageal reflux disease. N Engl J Med. 2022;387(13):1207–16. 10. Samo S, Carlson DA, Gregory DL, Gawel SH, Pandolfino JE, Kahrilas PJ. Incidence and prevalence of achalasia in central Chicago, 2004-2014, since the widespread use of high-resolution manometry. Clin Gastroenterol Hepatol. 2017;15(3):366–73. 11. Werner YB, Hakanson B, Martinek J, et al. Endoscopic or surgical myotomy in patients with idiopathic achalasia. N Engl J Med. 2019;381(23):2219–29. 12. Low EE, Demb J, Shah SC, et al. Risk of esophageal cancer in achalasia: A matched cohort study utilizing the nationwide veterans affairs achalasia cohort (VA-AC). Am J Gastroenterol. 2024;119(4):635–45. 13. Muthusamy VR, Wani S, Gyawali CP, Komanduri S, CGIT Barrett's Esophagus Consensus Conference Participants. AGA clinical practice update on new technology and innovation for surveillance and screening in Barrett's esophagus: Expert review. Clin Gastroenterol Hepatol. 2022;20(12):2696–706.e1.
留言 (0)