
記住我



Renal cell carcinoma (RCC) is the third most common urological cancer and can have a variety of different presentations with many patients presenting with vague clinical symptoms. Localized disease is often treated with surgical resection; however, almost 40% of patients can develop metastatic disease after a nephrectomy.1 In addition, around 30% of patients who are diagnosed with RCC have metastases at the time of diagnosis.2 The most common place of metastasis for RCC is the lung, followed by bone and liver.3 Gastrointestinal (GI) tract involvement with primary RCC is extremely rare and only a handful has been reported. There have been previous case studies looking at duodenal metastasis presenting as upper GI bleeding.4,5 There was another case report demonstrating metastatic RCC to the gastric body.6 There have been a few reports of rectosigmoid metastasis and the transverse colon.7-10 In addition, there has been other reports of metastasis in the splenic flexure.11,12 However, to our knowledge, there is no reported case of metastasis to the cecum. Here, we present a rare case of cecal metastasis of clear cell RCC.
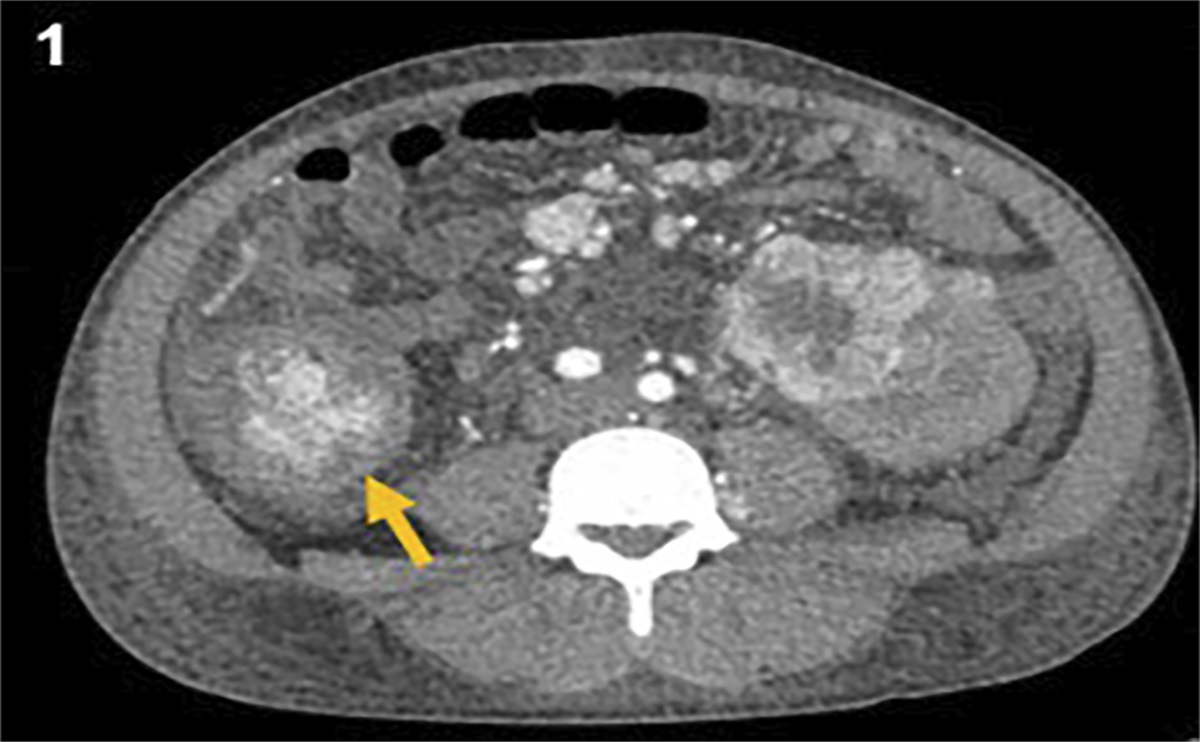
CASE REPORTA man in his 40s with a history of RCC and diabetes presented to the emergency department for abdominal pain, generalized weakness, and melena. He was found to be anemic with hemoglobin of 3.1 g/dL. The patient had a history of clear cell RCC for which he had underwent a right radical nephrectomy 7 years before this presentation and was found without evidence of disease after his nephrectomy. Five years after the nephrectomy, he was found to have extensive abdominal wall and brain metastases and underwent radiation (20 Gy) and 3 cycles of nivolumab. A bone scan at that time showed no evidence of metastasis. A computed tomography scan a month after his radiation and nivolumab application showed decrease in size of previously seen metastatic lesions. The patient was subsequently lost to follow-up as he moved to a different state. On this presentation to our hospital, computed tomography of the abdomen and pelvis demonstrated new bone metastases and a hyperenhancing lesion in the ascending colon with associated intussusception measuring 4.8 cm at the largest dimension (Figure 1). Surgery was consulted for the mass and concern of intussusception, and the patient was deemed not a surgical candidate given widely metastatic disease. The patient then underwent a colonoscopy that showed a partially obstructing large nonbleeding mass in the cecum that measured 6 cm, which was biopsied and revealed RCC primary (Figure 2). Microscopic examination of the biopsy showed malignant cells with abundant clear cytoplasm and round nuclei and nuclear PAX-8 positivity consistent with metastatic clear cell RCC (Figure 3). Unfortunately, the patient's clinical status deteriorated shortly after this metastatic diagnosis, and he enrolled into hospice care.
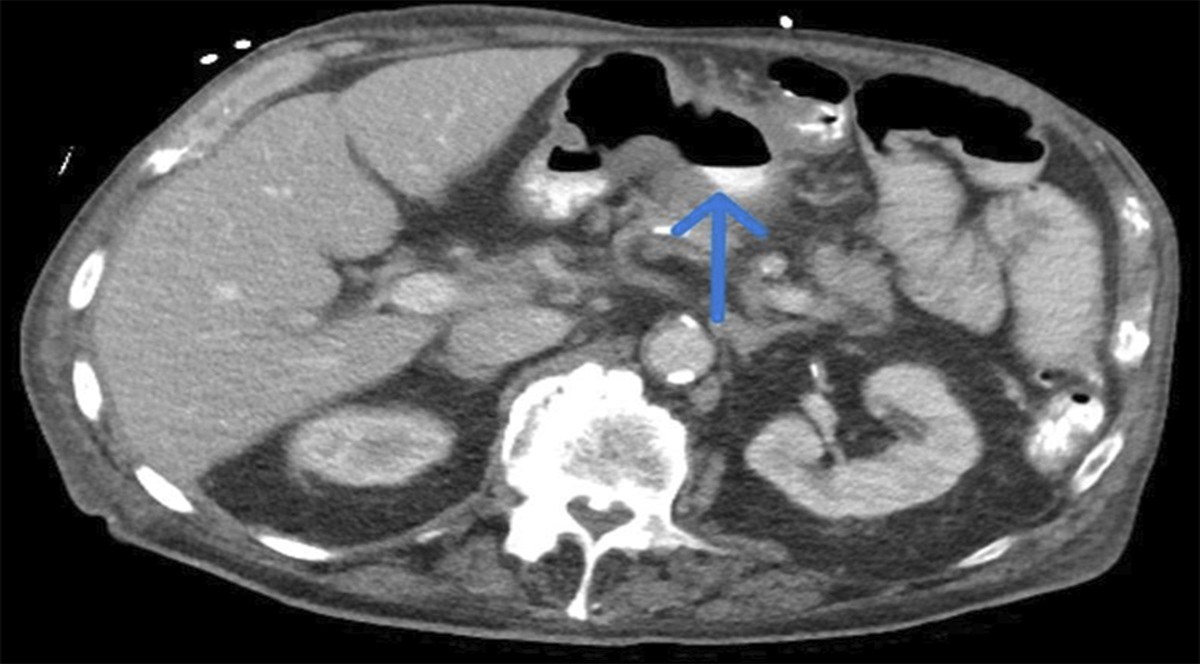
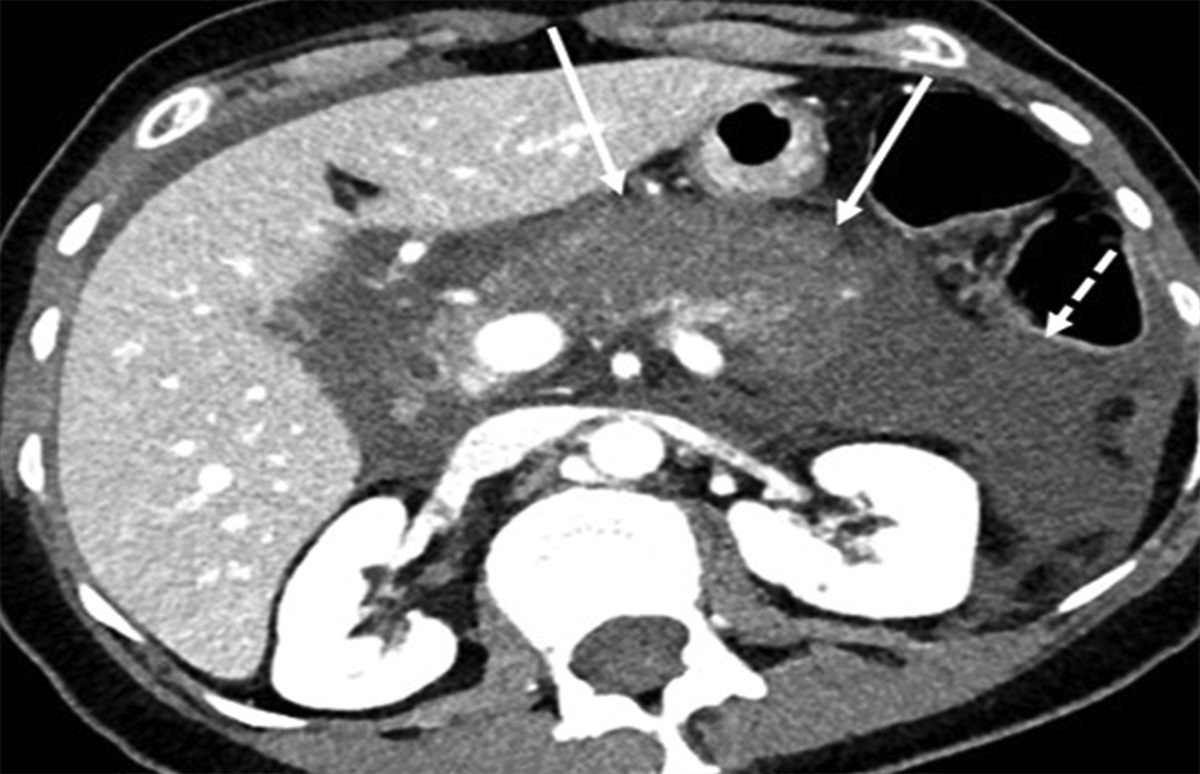
 Figure 1.:
Figure 1.: Computed tomography of the abdomen and pelvis showing a new right colonic mass with associated intussusception.
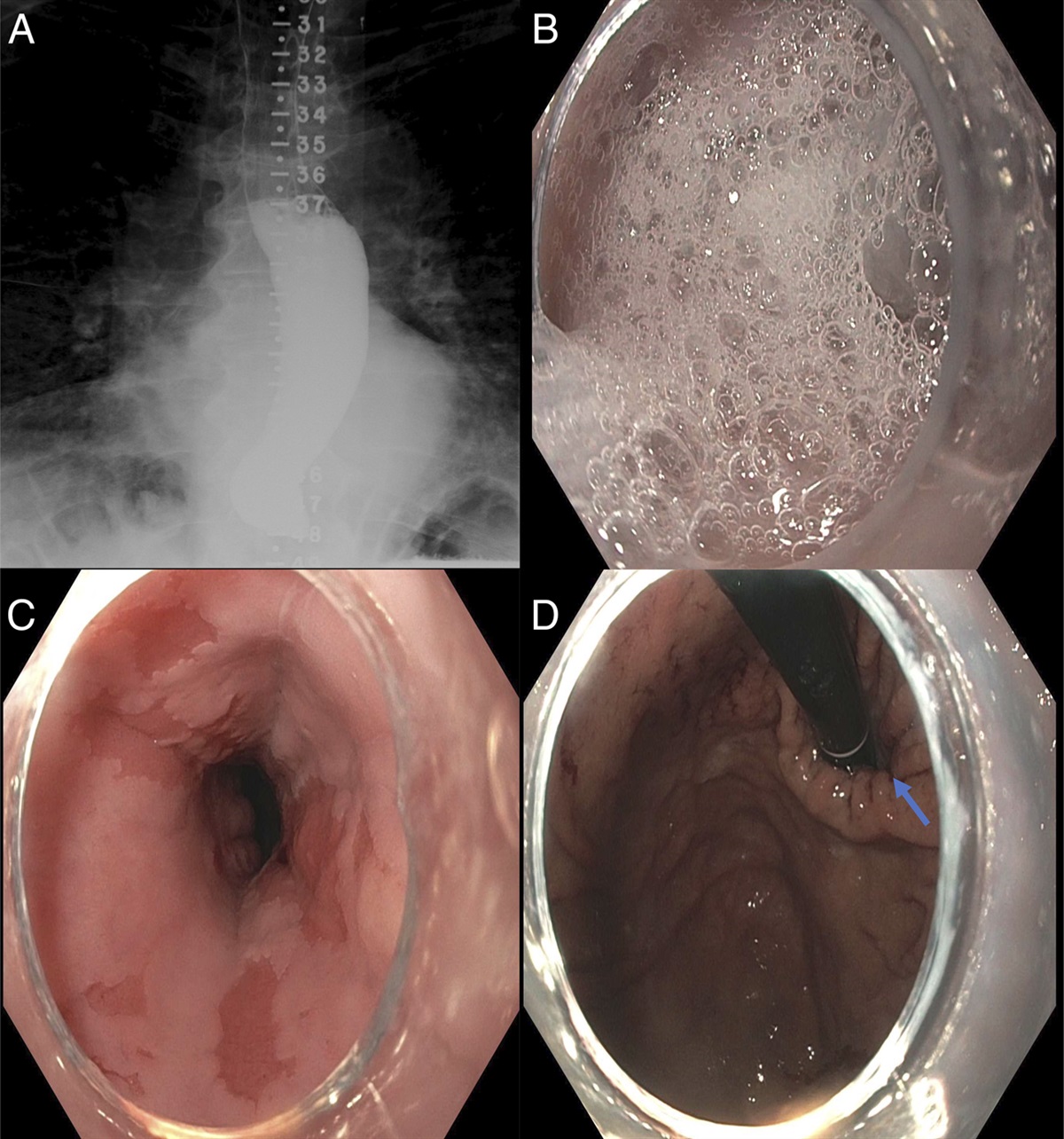
 Figure 2.:
Figure 2.: Colonoscopy showed a large fungating mass in the cecum that was 6 cm in size and occupying two-thirds of the cecal circumference.
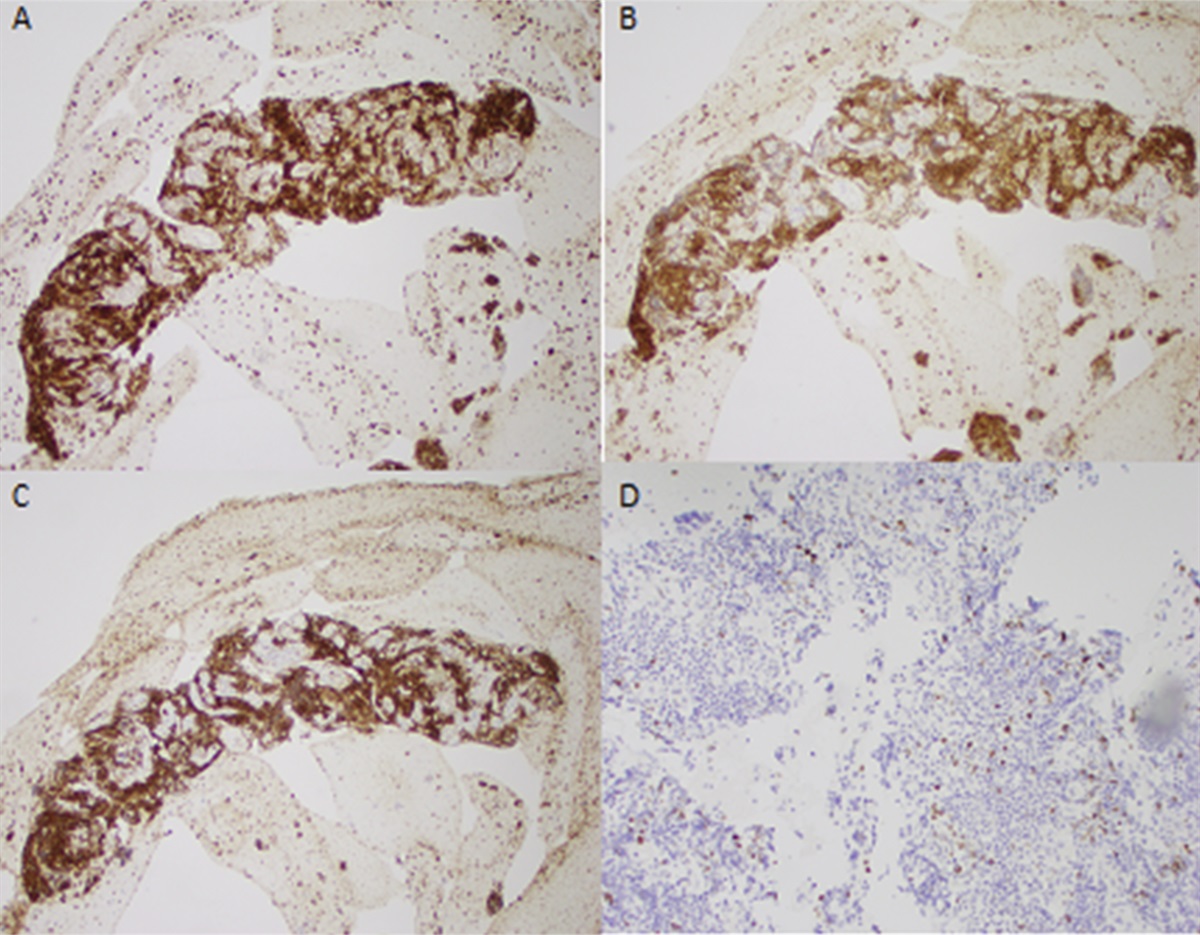
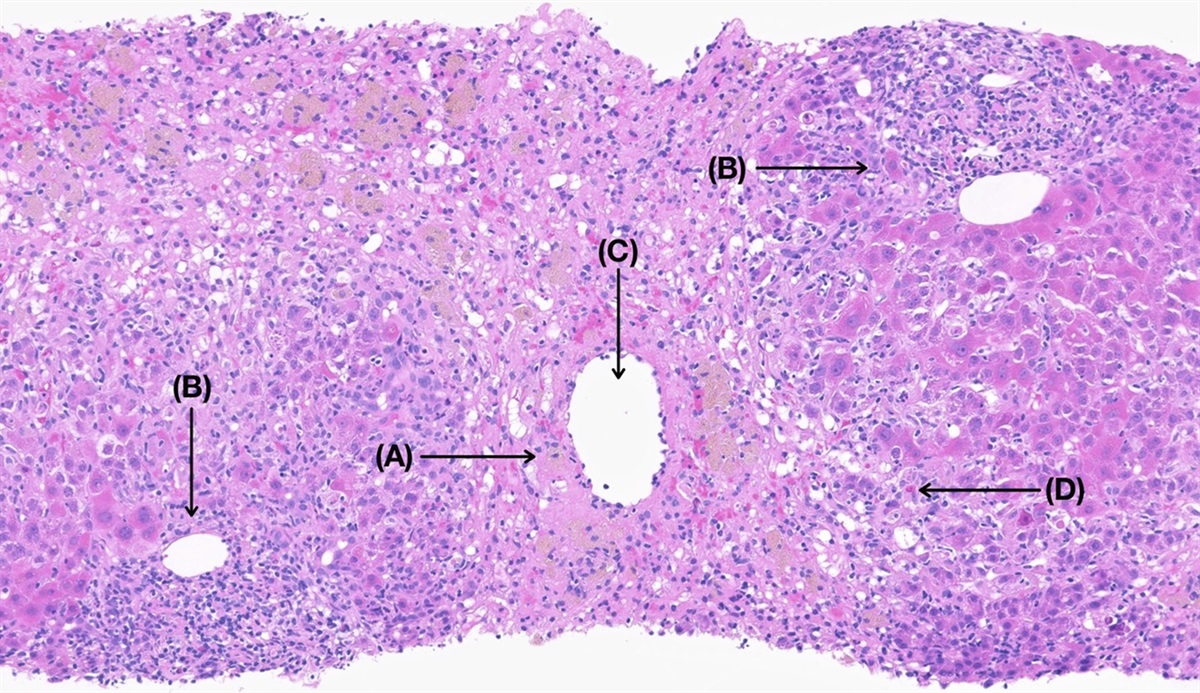
 Figure 3.:
Figure 3.: Malignant cells with abundant clear cytoplasm and round nuclei and nuclear PAX-8 positivity consistent with metastatic clear cell renal cell carcinoma.
DISCUSSIONRCC is most frequently seen in patients in the sixth and seventh decades of life and more common in men.13 The majority of RCC occurs sporadically with around 4% of the malignancies being related to familial syndromes.14 After curative resection of the patients with RCC, the recurrence rate is 20%–40%.10 RCC can metastasize to various areas of the body through lymphatic, hematogenous, or direct invasion. Location of metastasis varies on different factors including the time of recurrence and the initial size of the tumor. Lymph node and distant metastasis could be seen in early recurrence, and the risk is higher if the tumor is larger.15
GI metastasis from RCC is rare and only occurs in 0.2%–0.7% of RCC cases.16 Metastasis can occur in the stomach, small bowel, or colon, and the most common presentation that has been reported is GI bleeding. The most common site of GI metastasis is the duodenum given the close proximity to the right kidney.17 Colonic metastasis is usually seen in patients with widely metastatic disease which was seen in our patient case.18 Interestingly, the majority of recurrence of RCC occurs in the first 3 years of disease and late recurrence beyond 5 years is what is typically seen in colonic metastases.1,19 In our case, the patient presented with metastatic colon disease 7 years after his resection. Guidance of treatment of GI metastasis from RCC is lacking given the rare occurrences. In previous case reports, several patients died before treatment. In one case, the patient was found to have splenic flexure metastasis and underwent colectomy and was found to be doing well 6 months after surgery.12 In another case, the patient with rectosigmoid colon involvement underwent a sigmoidectomy who then presented 6 months later with liver metastases.7
To our knowledge, there have been no other reported cases of RCC metastasizing to the cecum. In general, 5-year survival rates of patients with metastatic RCC are poor and reported to be around 12%.20 This patient case emphasizes the importance for carefully evaluating patients with a history of RCC who present with concerning symptoms, such as GI bleeding. This case along with other previously reported cases with RCC metastasizing to various areas in the GI tract demonstrate the importance of closer routine surveillance particularly since many of the cases were at least 5 years after a nephrectomy.7–10,12 Given high mortality, providers should have high clinical suspicion of metastatic RCC in less common metastatic sites such as the GI tract in patients who present with atypical symptoms. This case also adds to the need to investigate further treatments for patients with metastatic RCC to the GI tract as there are currently no clear guidelines.
DISCLOSURESAuthor contributions: RY Lin, S. Shen, PL Donabedian, C. Kiani, JA Chatzkel, JL Kresak, and L. Dakhoul: conception, writing manuscript, final review; JL Kresak: providing pathology; RY Lin: final review and submission, is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Fujii Y, Ikeda M, Kurosawa K, et al. Different clinicopathological features between patients who developed early and late recurrence following surgery for renal cell carcinoma. Int J Clin Oncol. 2015;20(4):802–7. 2. Pavlakis GM, Sakorafas GH, Anagnostopoulos GK. Intestinal metastases from renal cell carcinoma: A rare cause of intestinal obstruction and bleeding. Mt Sinai J Med. 2004;71(2):127–30. 3. McKay RR, Kroeger N, Xie W, et al. Impact of bone and liver metastases on patients with renal cell carcinoma treated with targeted therapy. Eur Urol. 2014;65(3):577–84. 4. Sadler GJ, Anderson MR, Moss MS, Wilson PG. Metastases from renal cell carcinoma presenting as gastrointestinal bleeding: Two case reports and a review of the literature. BMC Gastroenterol. 2007;7:4. 5. Munir A, Khan AM, McCarthy L, Mehdi S. An unusual case of renal cell carcinoma metastasis to duodenum presenting as gastrointestinal bleeding. JCO Oncol Pract. 2020;16(1):49–50. 6. Hakim C, Mendelson A, Patel J, Greer J, Sorser S. Metastatic renal cell carcinoma presenting as gastrointestinal bleeding. Case Rep Gastroenterol. 2021;15(2):478–81. 7. Vo E, Palacio CH, Omino R, Link RE, Sada Y, Avo A. Solitary colon metastasis from renal cell carcinoma nine years after nephrectomy: A case report. Int J Surg Case Rep. 2016;27:55–8. 8. Zhang F, Zhao G, Wu P, et al. Asynchronous abdominal wall and sigmoid metastases in clear cell renal cell carcinoma: A case report and literature review. Asian J Urol. 2019;6(2):210–4. 9. Jadav AM, Thrumurthy SG, DeSousa BA. Solitary colonic metastasis from renal cell carcinoma presenting as a surgical emergency nine years post-nephrectomy. World J Surg Oncol. 2010;8:54. 10. Tokonabe S, Sugimoto M, Komine Y, Horii H, Matsukuma S. Solitary colonic metastasis of renal cell carcinoma seven years after nephrectomy: A case report. Int J Urol. 1996;3(6):501–3. 11. Valdespino-Castillo VE, Ruiz-Jaime A. Renal cell carcinoma with colon metastases: An infrequent site for metastases [in Spanish]. Cir Cir. 2008;76(4):339–42. 12. Subasi O, Aziret M, Karaman K, Ercan M. Colonic metastasis of renal cell carcinoma following curative nephrectomy: A case report and review of the literature. Int J Surg Case Rep. 2019;65:152–5. 13. Chow WH, Devesa SS, Warren JL, Fraumeni JF Jr. Rising incidence of renal cell cancer in the United States. JAMA. 1999;281(17):1628–31. 14. Brookman-May SD, May M, Shariat SF, et al. Time to recurrence is a significant predictor of cancer-specific survival after recurrence in patients with recurrent renal cell carcinoma: Results from a comprehensive multi-centre database (CORONA/SATURN-Project). BJU Int. 2013;112(7):909–16. 15. Guðmundsson E, Hellborg H, Lundstam S, Erikson S, Ljungberg B, Swedish Kidney Cancer Quality Register Group. Metastatic potential in renal cell carcinomas ≤7 cm: Swedish kidney cancer quality register data. Eur Urol. 2011;60(5):975–82. 16. Namikawa T, Hanazaki K. Clinicopathological features and treatment outcomes of metastatic tumors in the stomach. Surg Today. 2014;44(8):1392–9. 17. Ouellet S, Binette A, Nguyen A, Garde-Granger P, Sabbagh R. Metastatic renal cell carcinoma initially presenting with hematochezia and subsequently with vaginal bleeding: A case report. BMC Urol. 2018;18(1):4. 18. Saitoh H. Distant metastasis of renal adenocarcinoma. Cancer. 1981;48(6):1487–91. 19. Kavolius JP, Mastorakos DP, Pavlovich C, Russo P, Burt ME, Brady MS. Resection of metastatic renal cell carcinoma. J Clin Oncol. 1998;16(6):2261–6. 20. Motzer RJ, Jonasch E, Michaelson MD, et al. NCCN guidelines insights: Kidney cancer, version 2.2020. J Natl Compr Canc Netw. 2019;17(11):1278–85.
留言 (0)