
記住我



Severe acute pancreatitis (AP) can cause systemic complications including renal failure, respiratory failure, among others, increasing the risk of associated morbidity and mortality. Severity of AP can be evaluated through laboratory and computed tomography (CT) imaging findings. Bowel complications associated with AP are rare. Extravasation of pancreatic enzymes into the abdominal cavity can cause an inflammatory reaction, leading to bowel wall inflammation and possible progression to bowel ischemia, necrosis, and/or perforation.1
CASE REPORTA 60-year-old woman with history of eosinophilic esophagitis presented with acute-onset nausea, vomiting, and diffuse abdominal pain of 24-hour duration that radiated to her midback. Abdominal pain was constant, graded at 10 of 10 in severity, without any aggravating or relieving factors. She denied ever experiencing similar symptoms previously. She denied history of gallstones or alcohol use. Vitals showed temperature 36.6°C, heart rate 81, respiratory rate 18, blood pressure 140/78, and oxygen saturation 94% on room air. Initial physical examination demonstrated an ill-appearing patient with hypoactive bowel sounds and generalized abdominal tenderness without rigidity or rebound tenderness.
Laboratory test results on initial presentation were significant for lipase 14,800 U/L (13-60), white blood cell (WBC) 19.8 × 109/L (3.4–9.6), triglycerides 186 mg/dL (<150), aspartate aminotransferase (AST) 30 U/L (8–43), alanine aminotransferase (ALT) 22 U/L (7–45), alkaline phosphatase (ALP) 90 U/L (35–104), total bilirubin 0.5 mg/dL (<1.2), direct bilirubin 0.1 mg/dL (<0.3), and lactate 3.0 mmol/L (0.5–2.2). Basic metabolic panel showed a blood urea nitrogen (BUN) of 15 mg/dL (6–21), creatinine of 0.71 mg/dL (0.59–1.04), and mild hypokalemia at 3.3 mmol/L (3.6–5.2). The patient was admitted to the hospital for evaluation and management of AP.
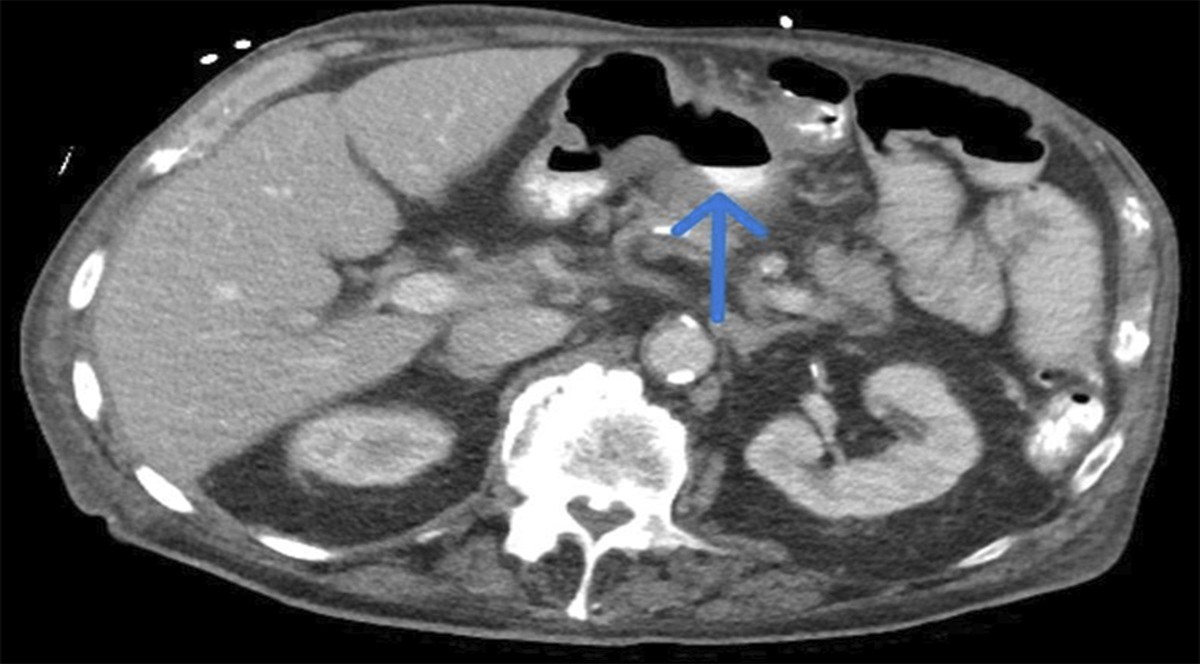
Abdominal CT with intravenous contrast on admission showed severe necrotizing pancreatitis (80% necrosis) with abdominopelvic free fluid (Figures 1 and 2). No obvious etiology of the pancreatitis was found. Abdominal ultrasound revealed mild common bile duct dilation at 8 mm. A nasoenteric feeding tube was placed for nutritional supplementation. On hospital day 3, repeat CT showed worsening necrotizing pancreatitis and new thrombosis of the superior mesenteric vein and splenic vein. The patient was subsequently started on a heparin infusion.
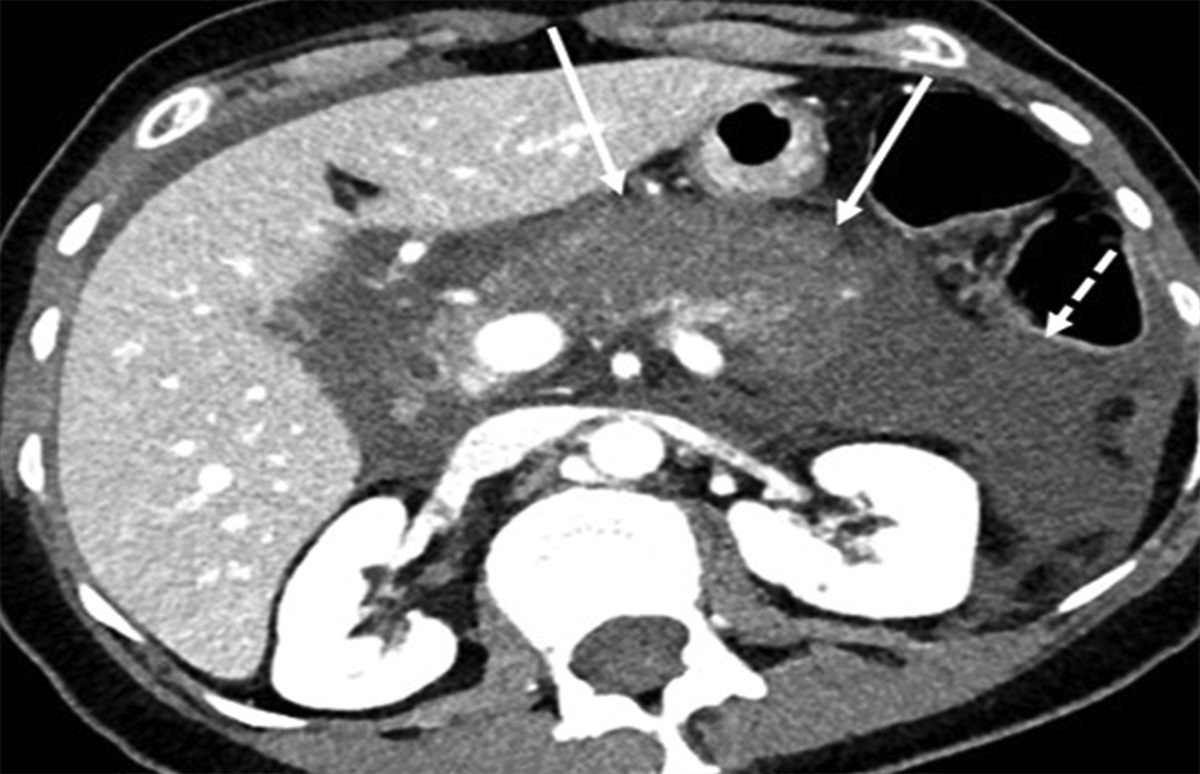
 Figure 1.:
Figure 1.: Axial computed tomography on admission demonstrating hypoenhancement of the pancreas (white solid arrows) and upper abdominal free fluid (white dashed arrow), consistent with acute necrotizing pancreatitis.
 Figure 2.:
Figure 2.: Coronal computed tomography on admission demonstrating normal wall thickness of the proximal sigmoid colon in the region of subsequent perforation (white dashed arrows). Upper abdominal free fluid consistent with acute pancreatitis.
On hospital day 8, the patient developed a fever up to 38.6°C with continued leukocytosis at 19.1 ×109/L (3.4–9.6). She was started on meropenem and vancomycin. Abdominal examination showed a tense and distended abdomen with decreased bowel sounds and generalized tenderness, so enteral nutrition was withheld. Repeat CT demonstrated necrotizing pancreatitis with new thickening of the descending and sigmoid colon with resolution of superior mesenteric vein and splenic vein thrombosis (Figure 3). Concurrently, the patient developed dyspnea requiring new oxygen supplementation. Chest CT imaging showed inflammation in the lungs with bilateral pleural effusions. Oxygen requirement increased up to high flow nasal cannula, and the patient was transferred to the intensive care unit for diuresis and closer monitoring. After successful diuresis and improvement of respiratory status leading to clinical stabilization, tube feeding was resumed. To evaluate for any biliary source of pancreatitis, magnetic resonance cholangiopancreatography was performed and showed no evidence of biliary duct dilation or biliary stones.
 Figure 3.:
Figure 3.: Coronal computed tomography on hospital day 8 demonstrating wall thickening of the distal descending and proximal sigmoid colon (white dashed arrows) with immediately adjacent free fluid (solid white arrow). Persistent changes of necrotic pancreatitis.
On hospital day 14, the patient had worsening abdominal pain and distension. Physical examination showed abdominal distension with new diffuse abdominal tenderness and tension but without any peritonitic signs. Urgent CT was performed and revealed new sigmoid colon perforation (Figure 4). The patient was taken for emergent exploratory laparotomy by colorectal surgery. A large 5-cm defect was found at the anterior sigmoid colon consistent with perforation. There was pancreatic free fluid in the abdomen with purulent and feculent material at the site of colonic perforation. A transverse loop colostomy was created with placement of 2 abdominal drains. Sigmoid colectomy was not performed because of high intraoperative pressor and oxygen requirements in the setting of acute respiratory distress syndrome.
 Figure 4.:
Figure 4.: Coronal computed tomography on hospital day 14 demonstrating a new large pelvic abscess (white solid arrows) contiguous with the proximal sigmoid colon (white dashed arrows), consistent with colonic perforation. Upper abdominal fluid collections (asterisks) and free fluid, consistent with evolving necrotizing pancreatitis.
The patient had a lengthy hospital stay lasting 4 weeks, but she recovered well. She continued to follow-up in the outpatient gastroenterology clinic and is currently doing well, 10 months after discharge from the hospital. She is planned for takedown of her diverting colostomy soon.
DISCUSSIONColonic complications in severe AP can occur in up to 15% of patients and include ileus, abscess, obstruction, fistula, and/or perforation.2 Colonic perforation is extremely rare, and literature is almost entirely limited to case reports. Severity of AP is graded through CT imaging by the CT severity index and Balthazar score (grade A–E), which consider the extent of AP-related inflammatory changes, fluid collections, and/or necrosis. In a retrospective study involving 75 patients with AP Balthazar grades B–E, the incidence of colon perforation was 5.3%, and the median time of onset was 13 days after the start of symptoms.3 In our case, there was severe pancreatitis by the CT severity index because of peripancreatic fluid and extensive pancreatic necrosis that was associated with the sigmoid colon rupture. Our patient's colon perforation occurred at 15 days from initial symptoms of AP, close to median time of onset seen in other cases.
Pathogenesis of colon perforation in severe AP is theorized to be a combination of colon ischemia and direct pancreatic enzyme-induced inflammation of the colon. The site of colon perforation usually occurs at the splenic flexure because of proximity to the pancreas and decreased vascularity (watershed zone).1
In our case, free fluid was present in the abdominal cavity, including immediately adjacent to the distal descending and sigmoid colon on the CT preceding the perforation. This suggests the pancreatic enzymes were associated with irritation of the sigmoid colon, leading to progressive inflammation and possible ischemic changes eventually resulting in perforation. The extent of our patient's colon perforation, as seen during laparotomy, highlights the severity of colonic complications that can occur in the setting of severe necrotizing pancreatitis.
Physicians should be aware of the potential colonic manifestations of severe AP. Colonic pathology may be clinically obscured by systemic involvement in severe AP. Physicians should closely monitor patients with serial abdominal examinations and imaging as needed. Perforation should be treated urgently with colectomy or ostomy formation to prevent associated morbidity and mortality.4
DISCLOSURESAuthor contributions: H. Saleh, IR Nimma, Y. Huang, D. Amiraian, M. Pang, M. DeLeon, J. Chan, MD Lewis, and JG Hashah contributed to multiple aspects of patient care and drafting of this manuscript and are the article guarantors. All authors approve the final draft submitted.
Financial disclosure: JG Hashah: Advisory Board for BMS.
Previous presentation: This case was presented at the ACG 2023 Annual Scientific Meeting; October 23, 2023; Vancouver, Canada.
Informed consent was obtained for this case report.
REFERENCES 1. Bansal A, Gupta P, Singh H, et al. Gastrointestinal complications in acute and chronic pancreatitis. JGH Open. 2019;3(6):450–5. 2. Dhadlie S, Ratnayake S. A rare case report of ascending colon perforation secondary to acute pancreatitis. Int J Surg Case Rep. 2019;55:62–5. 3. Nakanishi N, Shimono T, Yamamoto A, Miki Y. CT evaluation and clinical factors predicting delayed colonic perforation following acute pancreatitis. Jpn J Radiol. 2016;34(1):10–5. 4. Nagpal AP, Soni H, Haribhakti S. Severe colonic complications requiring sub-total colectomy in acute necrotizing pancreatitis: A retrospective study of 8 patients. Indian J Surg. 2015;77(1):3–6.
留言 (0)