
記住我



Chronically elevated hepatic venous pressure due to right-sided heart failure causes congestive hepatopathy (CH). Chronically untreated CH can lead to cirrhosis and hepatocellular carcinoma, thereby increasing mortality. A major challenge is that physical examination cannot accurately diagnose organ dysfunction due to CH. Furthermore, laboratory findings are nonspecific for CH, often normal until advanced disease, and do not correlate with the grade of fibrosis on biopsy.1 A relatively new point-of-care ultrasound (POCUS) examination, Venous Excess Ultrasound Score (VExUS), is gaining popularity for diagnosing and grading the severity of venous congestion, but its utility in CH is unknown. VExUS differentiates between normal, mild, moderate, and severe venous congestion by combining multiple ultrasonographic measurements, including inferior vena cava (IVC) diameter and pulsed-wave Doppler assessments of the portal, hepatic, and intrarenal veins.2 We present a case of acute liver injury secondary to CH where the diagnosis and management was guided by VExUS. This case demonstrates how VExUS may support a diagnosis of CH and can spare some patients from an invasive liver biopsy.
CASE REPORTA 73-year-old man with pancreatic adenosquamous carcinoma, biventricular heart failure with reduced ejection fraction (30%-35%), and paroxysmal atrial fibrillation presented to the hospital with a 2-day history of bilateral lower extremity edema and 5-pound weight gain. He was admitted for acute decompensated heart failure and diuresed with intravenous furosemide until he was deemed euvolemic by physical examination. He subsequently developed worsening mental status and increasing liver enzymes.
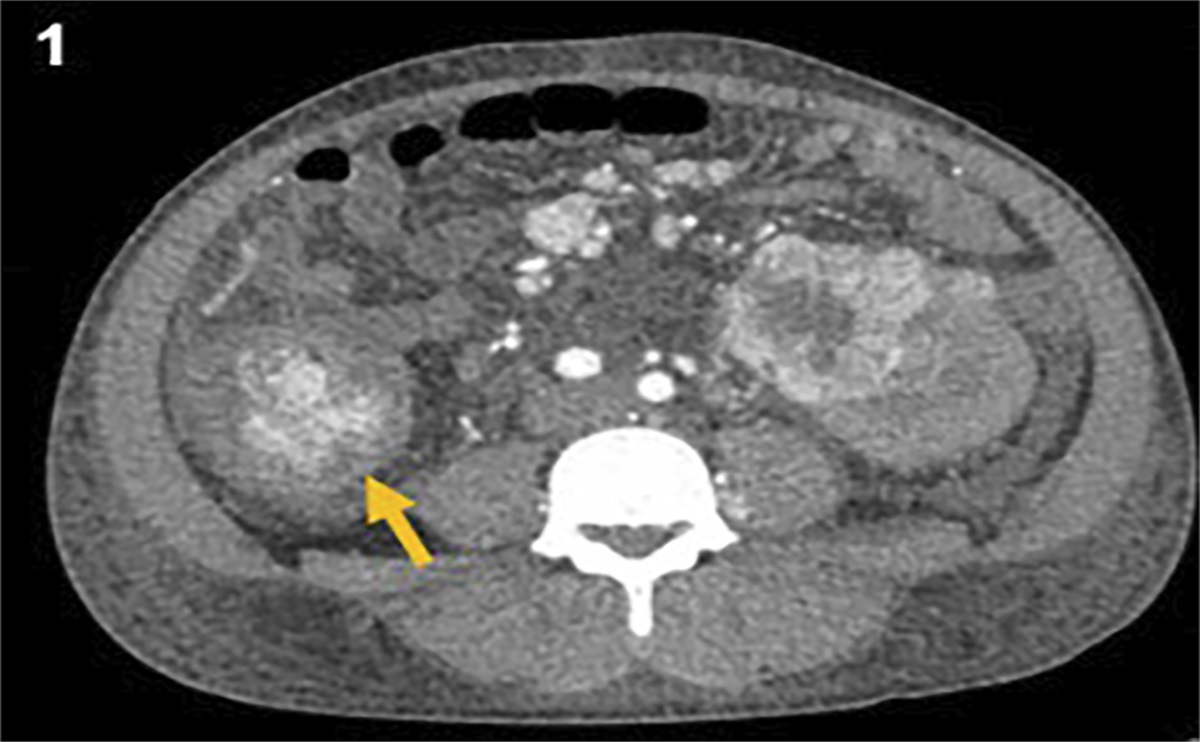
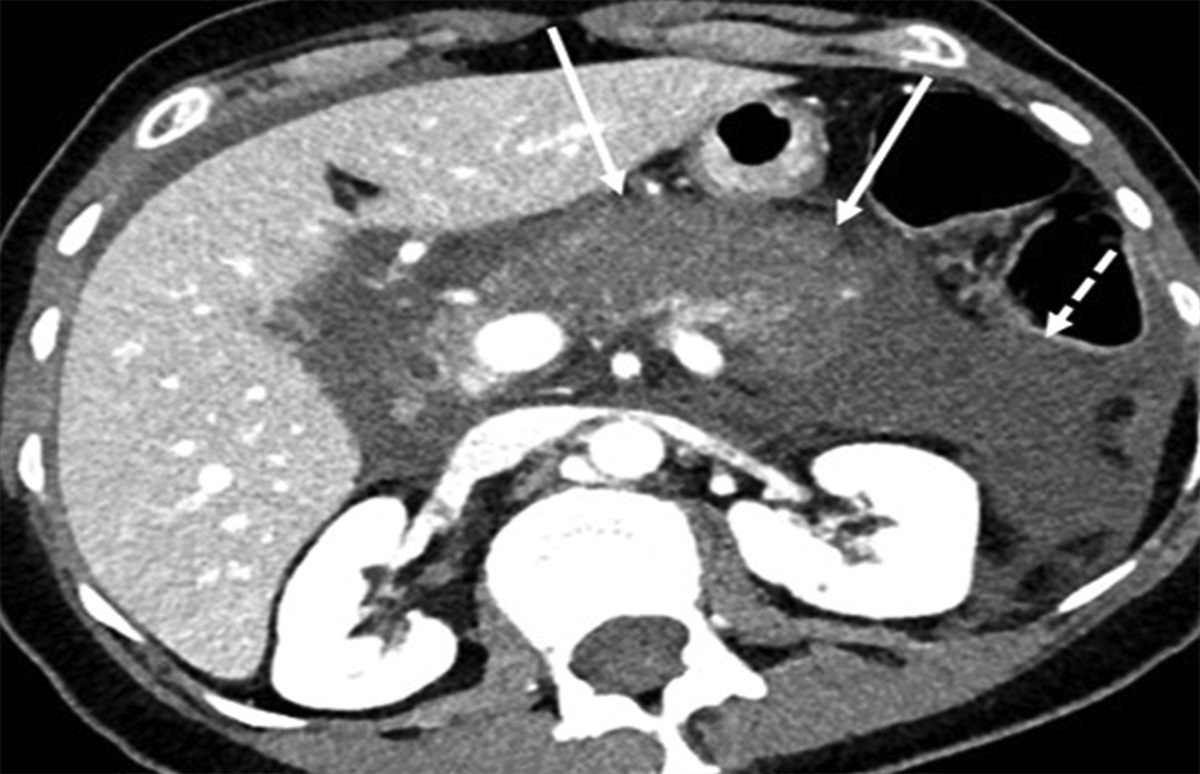
On physical examination, he was hemodynamically stable and had confusion, asterixis, scleral icterus, lower extremity edema, clear lungs bilaterally, and difficult to appreciate jugular venous distention. Laboratory results were remarkable for elevated B-type natriuretic peptide (2,883 pg/mL), alanine aminotransferase (487 U/L), aspartate aminotransferase (727 U/L), alkaline phosphatase (293 U/L), total bilirubin (4.9 mg/dL), international normalized ratio (3.1), and ammonia (65 mg/L). Liver enzymes were normal 1 month before hospitalization. Abdominal computed tomography with contrast was remarkable for passive congestion of the liver from right heart failure with overlapping steatosis and a known enlarging pancreatic tail mass (5.7 cm) without intraductal biliary dilation. Gastroenterology was consulted for liver dysfunction, and workup for infiltrative, obstructive, autoimmune, and ischemic hepatopathies was negative. Although CH was the most likely etiology in the setting of chronic right-sided heart failure, a transjugular liver biopsy for a definitive diagnosis was recommended.
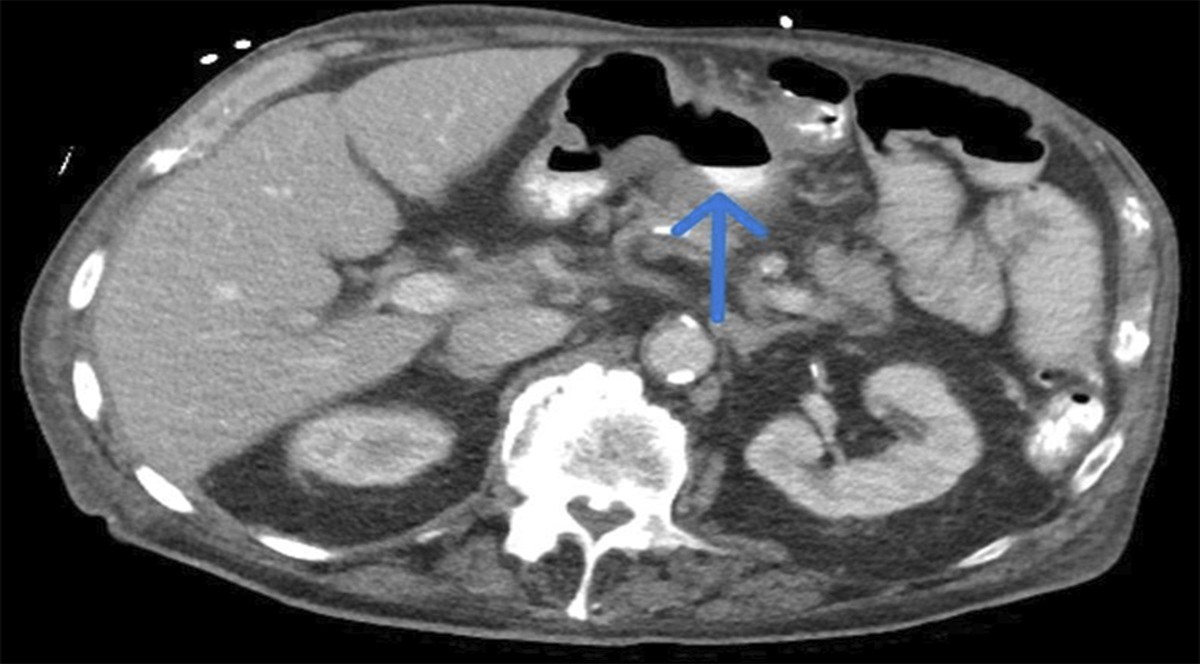
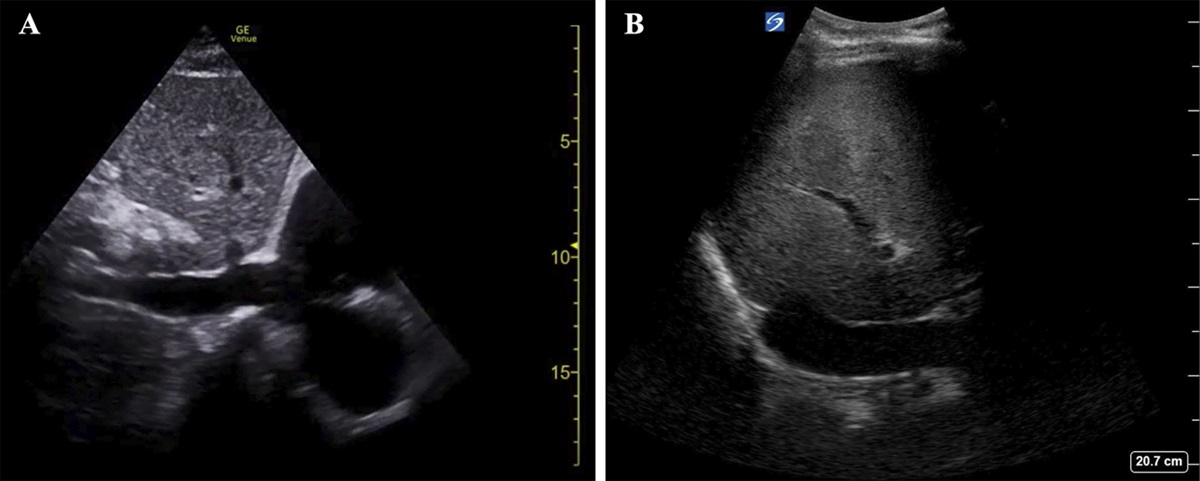
Before liver biopsy, VExUS was performed at the bedside and demonstrated grade III severe congestion. The IVC was dilated >2 cm without respiratory variation consistent with a central venous pressure >15 mm Hg (Figure 1). The hepatic and portal venous spectral Doppler waveforms were severely abnormal demonstrating flow reversal and pulsatility, respectively (Figure 2). The VExUS findings strongly supported a diagnosis of CH and aggressive diuresis was initiated, despite the patient being deemed euvolemic by physical examination. After escalating diuretic therapy, the patient's encephalopathy resolved, and his liver enzymes decreased over the subsequent 24–48 hours. Based on his clinical improvement, a liver biopsy was no longer indicated and was canceled.
 Figure 1.:
Figure 1.: Inferior vena cava (IVC) longitudinal view. (A) Normal IVC with a diameter of 1.2–1.7 cm. (B) Patient's IVC was abnormal with dilatation >2.1 cm without inspiratory collapse consistent with a central venous pressure >15 mm Hg.
 Figure 2.:
Figure 2.: Bedside Venous Excess Ultrasound Score (VExUS) images with normal references for comparison. (A) Normal hepatic vein spectral Doppler waveform showing S-wave amplitude greater than D-wave amplitude. (B) Patient's abnormal hepatic vein spectral Doppler waveform showing S-wave reversal. (C) Normal portal vein spectral Doppler waveform showing <30% pulsatility index (pulsatility index = [Velocity max − Velocity min]/Velocity max). (D) Patient's abnormal portal vein spectral Doppler waveform showing >50% pulsatility index. (E) Normal renal vein spectral Doppler waveform showing continuous monophasic flow (red arrow). (F) Patient's renal vein spectral Doppler examination was nondiagnostic.
DISCUSSIONBased on our literature search, this is the first documented case illustrating the use of VExUS as a bedside diagnostic tool for CH. CH occurs due to chronically elevated hepatic venous pressures secondary to right-sided heart failure.1 Acute elevations in these pressures can result in acute liver injury and transient elevations in transaminases. Morbidity in this setting is driven primarily by the severity of cardiac disease. Meanwhile, chronic CH carries high morbidity and mortality due to the development of hepatic fibrosis, cirrhosis, and hepatocellular carcinoma.3 CH has been traditionally diagnosed clinically by physical examination and laboratory testing. However, defining euvolemia by physical examination has been controversial and is often debated between specialists caring for the same patient.4,5 Common metrics, such as daily fluid balance, body weight, and physical examination (jugular venous distention, pulmonary edema, and peripheral edema), are largely subjective and not proportionate to a patient's true degree of systemic venous congestion.2 In addition, CH is a noninflammatory condition where early clinical signs are due to portal hypertension in the setting of preserved synthetic function, and therefore, the diagnostic tests are nonspecific and may not be abnormal until advanced disease.1,6 Prompt diagnosis of CH is critical to guide early therapeutic management, prevent acute liver injury or failure, and mitigate the long-term risk of developing cirrhosis and hepatocellular carcinoma.1
POCUS allows clinicians to systematically and objectively diagnose and grade the severity of venous congestion compared with physical examination. Past studies have demonstrated how POCUS can noninvasively estimate right atrial pressure by measuring IVC diameter and collapsibility, even using handheld ultrasound devices, to guide diagnosis of acute heart failure.7,8 However, measurement of IVC diameter and collapsibility is a poor diagnostic indicator for venous congestion with a specificity of only 41%. Assessment of venous congestion with VExUS is more accurate because it requires spectral Doppler interrogation of additional distal veins, namely the portal, hepatic, and interlobular renal veins, providing a more comprehensive evaluation of hypervolemia that can guide therapy.2
There is evidence in the literature suggesting that VExUS can be used as a real-time hemodynamic marker to objectively monitor venous congestion in different clinical scenarios.9 However, there is currently limited literature on the use of VExUS for diagnosing and monitoring CH. As illustrated in our case, VExUS offered a more accurate and rapid assessment of volume status and venous organ congestion compared with traditional physical examination. This protocol has demonstrated favorable performance in predicting right arterial pressure >12 mm Hg (AUC 0.99, 95% CI 0.96–1) compared with alternative established methods, such as IVC diameter (Area Under the Curve (AUC) 0.79, 95% Confidence Interval (CI) 0.65–0.92).10 VExUS has potential to support a diagnosis of CH, reduce the need for invasive testing such as liver biopsy, and facilitate targeted management of venous congestion, which can ultimately improve patient outcomes. Further investigation is warranted to determine the utility of VExUS in diagnosing and managing CH, a disease associated with significant morbidity and mortality when diagnosis is delayed.
DISCLOSURESAuthor contributions: All authors participated in the preparation and finalization of this manuscript. F. Dollar, R. Nathanson, NJ Soni, and L. Kuo gathered, organized, and synthesized patient data to report the case. F. Dollar, R. Nathanson, NJ Soni, LK, I. Gonzalez, and N. Shankar reviewed relevant literature, discussed, and drafted the discussion section. F. Dollar is the article guarantor.
Financial disclosure: NJ Soni receives funding from the US Department of Veterans Affairs (VA), Quality Enhancement Research Initiative (QUERI) Partnered Evaluation Initiative Grant (HX002263-01A1) and the VA National Center for Patient Safety. The contents of this publication do not represent the views of the US Department of Veterans Affairs or the US Government.
Previous presentation: To Diurese Or Biopsy? VExUS to the Rescue; Society of Hospital Medicine Conference 2023; March 28, 2023, Austin, Texas, USA
Informed consent was obtained for this case report.
REFERENCES 1. Lemmer A, VanWagner L, Ganger D. Congestive hepatopathy: Differentiating congestion from fibrosis. Clin Liver Dis (Hoboken). 2017;10(6):139–43. 2. Beaubien-Souligny W, Rola P, Haycock K, et al. Quantifying systemic congestion with point-of-care ultrasound: Development of the venous excess ultrasound grading system. Ultrasound J. 2020;12(1):16. 3. Lemmer A, VanWagner LB, Ganger D. Assessment of advanced liver fibrosis and the risk for hepatic decompensation in patients with congestive hepatopathy. Hepatology. 2018;68(4):1633–41. 4. Maw AM, Lucas BP, Sirovich BE, Soni NJ. Discharge-ready volume status in acute decompensated heart failure: A survey of hospitalists. J Community Hosp Intern Med Perspect. 2020;10(3):199–203. 5. Maw A, Ortiz-Lopez C, Morris M, et al. Hospitalist perspectives of available tests to monitor volume status in patients with heart failure: A qualitative study. Cureus. 2020;12(6):e8844. 6. Morales A, Hirsch M, Schneider D, González D. Congestive hepatopathy: The role of the radiologist in the diagnosis. Diagn Interv Radiol. 2020;26(6):541–5. 7. Darwish OS, Mahayni A, Kataria S, Zuniga E, Zhang L, Amin A. Diagnosis of acute heart failure using inferior vena cava ultrasound: Systematic review and meta-analysis. J Ultrasound Med. 2020;39(7):1367–78. 8. Elzeneini M, Gupta S, Li Y, Guo Y, Hamburger R. Estimation of right atrial pressure using a portable handheld ultrasound device. Am J Med. 2022;135(11):1378–81. 9. Rola P, Miralles-Aguiar F, Argaiz E, et al. Clinical applications of the venous excess ultrasound (VExUS) score: Conceptual review and case series. Ultrasound J. 2021;13(1):32. 10. Longino A, Martin K, Leyba K, et al. Correlation between the VExUS score and right atrial pressure: A pilot prospective observational study. Crit Care. 2023;27(1):205.
留言 (0)