
記住我



Hepatocellular carcinoma (HCC) is the fifth most common cancer and the fourth leading cause of cancer-related deaths worldwide.1 Well-established risk factors of HCC include chronic hepatitis B or chronic hepatitis C virus infection, excessive alcohol consumption, and metabolic factors (diabetes, obesity, hypertension, dyslipidemia). These factors contribute to hepatic fibrosis and cirrhosis, which further increase the risk of HCC.2
There are a few case reports on development of HCC in patients with chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL). Some of them have detailed concurrent HCC and CLL/SLL in people with preexisting liver damage from hepatitis C.3,4 Only 2 reports to date have described this phenomenon in patients without preexisting liver damage, with CLL/SLL diagnosed a substantial time before HCC in both cases.5,6 To the best of our knowledge, we present the first case of HCC without chronic liver disease or hepatic fibrosis where coexisting CLL/SLL was not clinically apparent before the diagnosis of HCC.
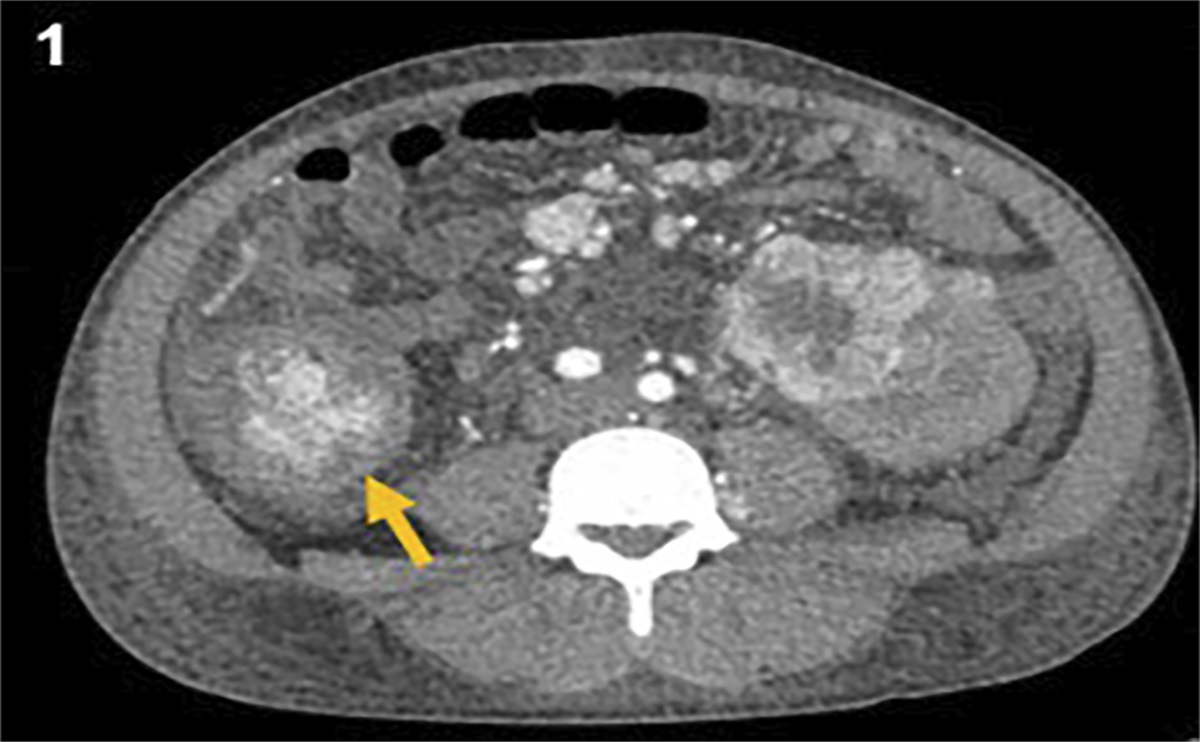
CASE REPORTThe patient is a 77-years-old African American man with a medical history of gastroesophageal reflux disease, type 2 diabetes mellitus, hypertension, benign prostatic hyperplasia, coronary artery disease, aortic dissection, and paroxysmal atrial fibrillation who initially presented to a local community hospital with hematuria. As part of the workup for hematuria, he underwent a computed tomography (CT) of the abdomen with an incidental finding of a 2.2 cm lesion in segments 7 and 8 of the liver. The patient otherwise had no evidence of cirrhosis on CT of the abdomen. Magnetic resonance imaging (MRI) of the abdomen was recommended after the index CT (within 1 month), and the MRI showed 1.7 cm lesion in the right lobe with rapid arterial enhancement and wash out and a questionable pseudo capsule. This was felt to represent an adenoma vs atypical hemangioma. His liver chemistries Aspartate aminotransferase (AST) 27 U/L, Alanine aminotransferase (ALT) 34 U/L, alkaline phosphatase (ALP) 69 IU/L, Tbili 0.7 mg/dL), platelet count (182 × 103 μL), and International Normalized Ratio (INR) (1.1) were within normal range. Viral hepatitis serologies (hepatitis A virus IgM antibody, hepatitis B virus total core antibody, hepatitis B virus surface antigen, hepatitis C virus antibody, hepatitis C virus RNA) were unremarkable. AFP level was 4 ng/mL. He had no significant alcohol or recreational drug use. His body mass index was 31.77 kg/m2.
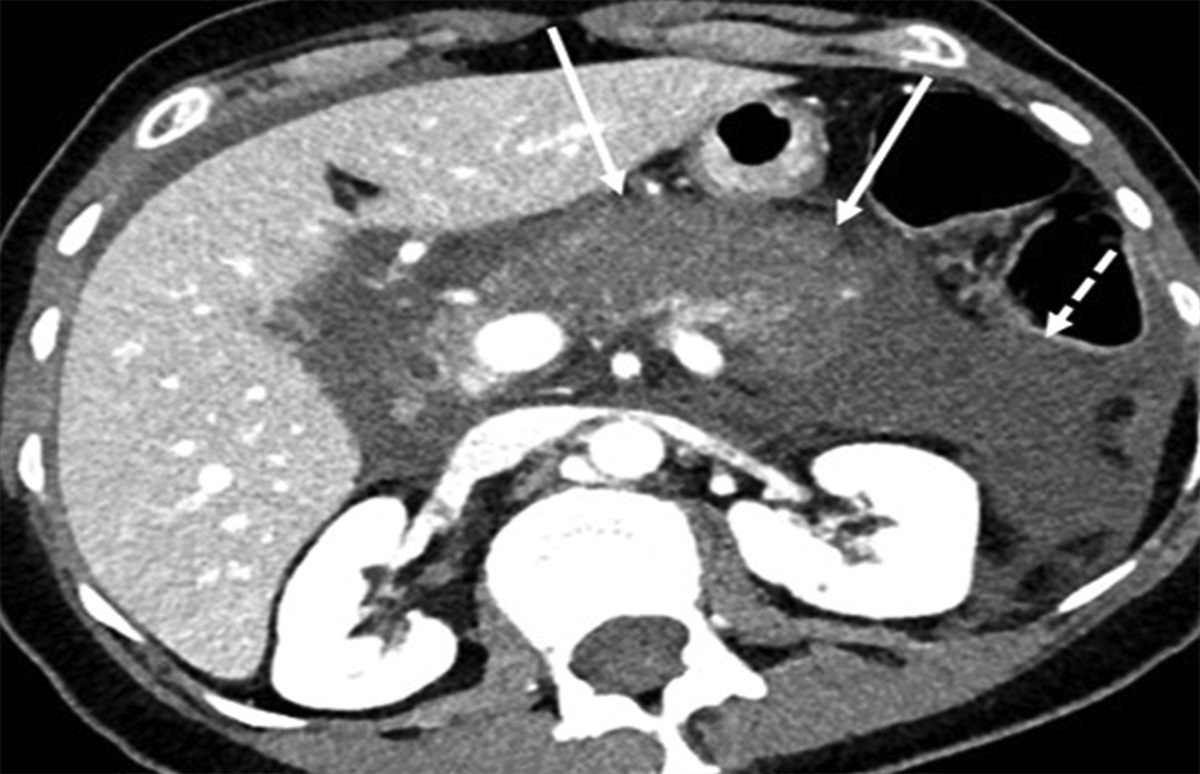
A follow-up MRI of the abdomen with contrast was performed at the local community hospital 7 months after the index CT, which showed increased size of the liver lesion to 5.6 × 4.3 cm with diffusely steatotic liver. The lesion was mildly hypointense on T1, minimally hyperintense on T2, restricted diffusion, showed heterogeneous early enhancement, and washed out to hypointensity with delayed enhancing pseudocapsule, Liver Imaging Reporting and Data System 5, consistent with HCC.7 The MRI also showed prominent lymph nodes in the porta hepatis.
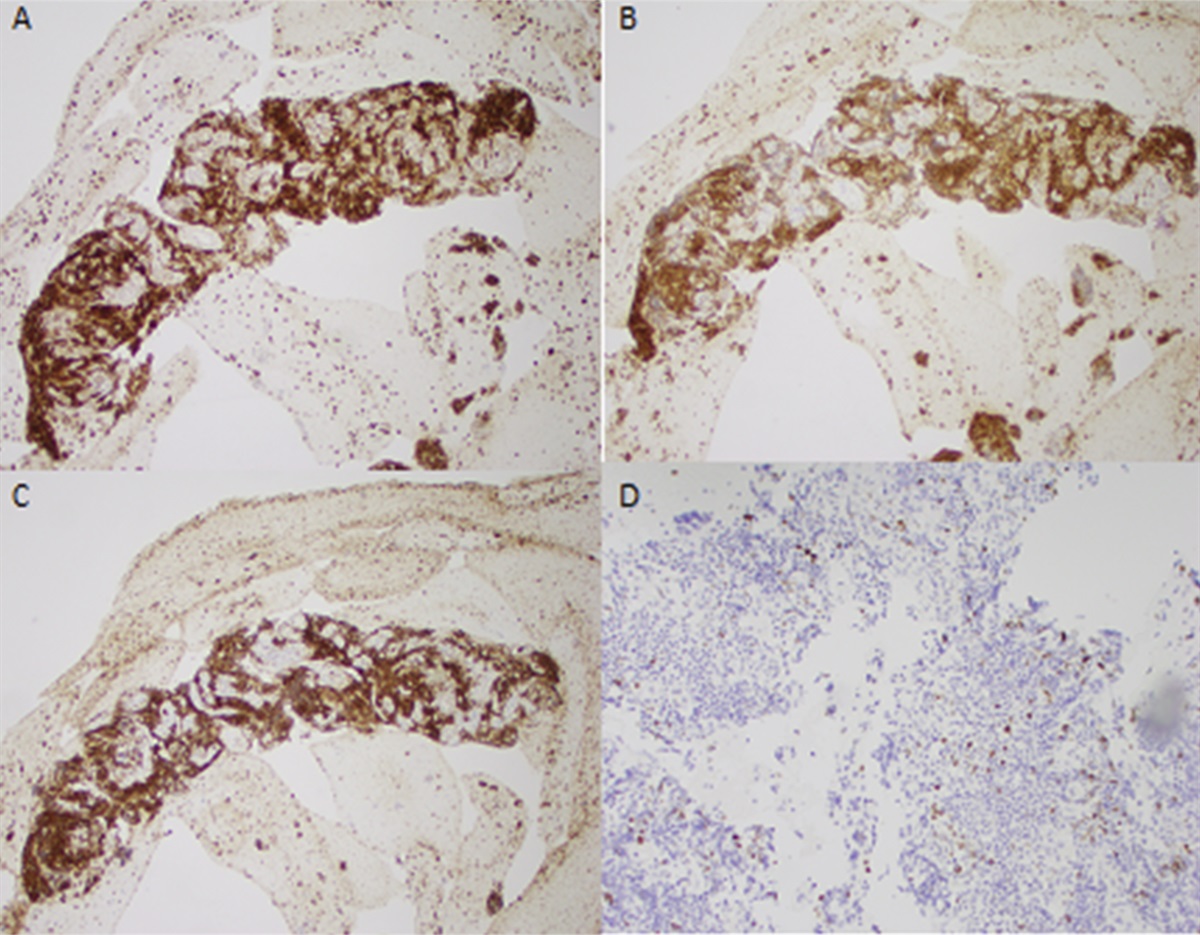
The patient was then referred from the local community practice to our center for further management. Upper endoscopic ultrasound was performed soon after which redemonstrated enlarged lymph nodes, with fine-needle aspiration showing reactive lymph nodes. Ten months after the index CT, the patient underwent open right hepatectomy of segments 7 and 8 with surgical pathology consistent with moderately differentiated HCC (52 mm in diameter) at our center. There was an incidental finding of portal-caval involvement of CLL/SLL and mild steatosis (10%), but no hepatic fibrosis was noted (Figure 1). Before this incidental finding, the patient did not have objective evidence suggestive of CLL/SLL including leuko/lymphocytosis, anemia, thrombocytopenia, splenomegaly, or nodal involvement on imaging.
 Figure 1.:
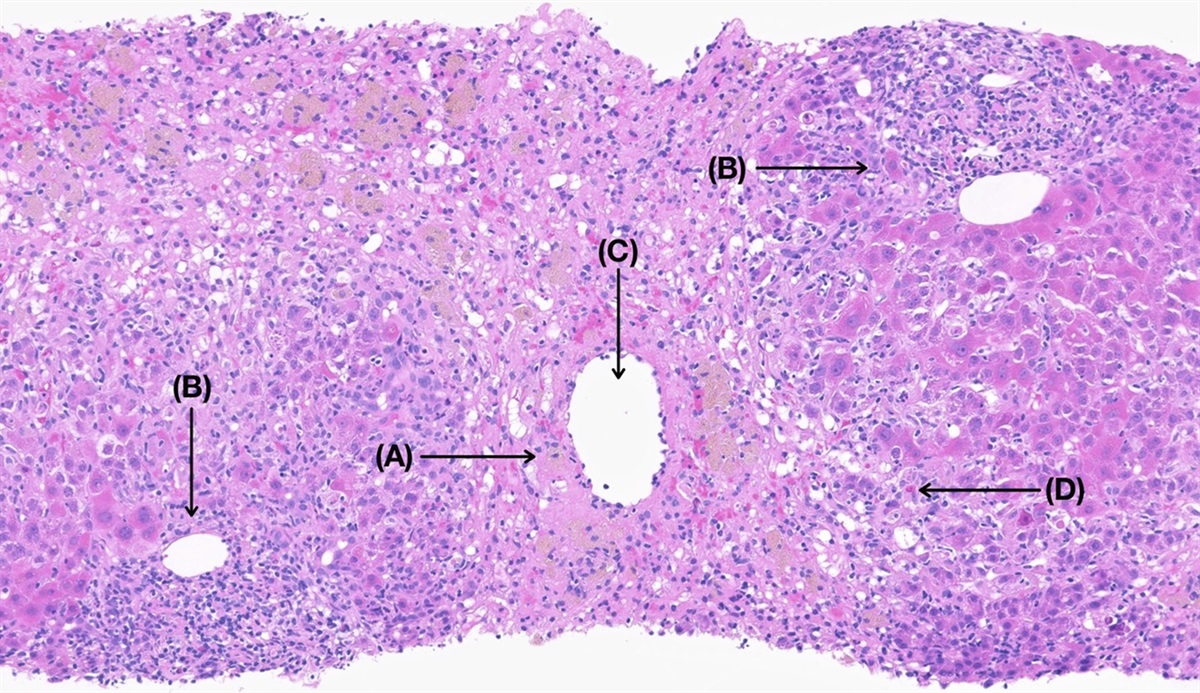
Figure 1.: Concurrent hepatocellular carcinoma and chronic lymphocytic leukemia/small lymphocytic lymphoma: (A) 6× Low-power photomicrograph demonstrates HCC at left and CLL/SLL, involving the background liver as a dense, portal-centric infiltrate, at right. (B) 200× High-power photomicrograph of the HCC demonstrates thickened cell plates, capillarization of the sinusoids, increased nucleus-to-cytoplasm ratio, scant mitotic activity, and some bile stasis. (C) 200× High-power photomicrograph demonstrating the CLL/SLL infiltrate filling and expanding a portal tract without interface activity; mild macrovesicular steatosis is noted in the adjacent lobule. Immunohistochemistry shows the infiltrate to express CD20 (D) 10× and not CD3 (E) and to aberrantly coexpress CD5 (F), and Lymphoid enhancer-binding factor 1 (LEF1) (G), supporting the diagnosis of CLL/SLL. CLL/SLL, chronic lymphocytic leukemia/small lymphocytic lymphoma.
He was referred to hematology/oncology for further evaluation and management of his newly diagnosed CLL/SLL along with HCC. Treatment of CLL/SLL was not indicated; instead, it was followed closely by oncology. A repeat MRI of the abdomen was obtained 15 months postsurgery and showed multiple new enhancing nodules in segments 2, 6, and 7 consistent with multifocal HCC. Multiple prominent axillary, mesenteric, and retroperitoneal lymph nodes related to his CLL/SLL were also newly noted. For his multifocal HCC, he began chemotherapy with lenvatinib but stopped 4 months later due to significant fatigue and physical decline. Another MRI abdomen was obtained 2 months later (21 months postsurgery) which showed increased size of all HCCs compared with prior. Since then, the patient has been on pembrolizumab therapy with no significant adverse effects. The patient has not required treatment of CLL/SLL and is closely followed by hematology/oncology.
DISCUSSIONThis case report highlights a rare instance of HCC in a patient with concurrent chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) but without traditional risk factors such as viral hepatitis, hepatic fibrosis, or cirrhosis.
Although HCC and CLL have been associated in prior case reports, an exact mechanistic association has yet to be elucidated. Genetic mutations involved in hereditary hemochromatosis, glycogen storage diseases, and Wilson disease have been associated with greater risk of HCC.8–10 While case reports exist on patients with these genetic diseases developing concurrent leukemias or lymphomas, there is no strong evidence of any genetic mutations that are common to individuals with HCC and individuals with CLL/SLL.11 Some causes of chronic liver disease, including hepatitis B, hepatitis C and iron overload, have been postulated to be associated with greater risk of non-Hodgkin lymphoma.12–14 However, our case did not involve any of these. Another potential hypothesis involves increased inflammatory cells from CLL/SLL in the liver leading to an inflammatory milieu, which ultimately leads to HCC. Our case is also unique as our patient had an atypical presentation of CLL, characterized by lack of clinical signs or symptoms of CLL before diagnosis. He was noted to have developed lymphadenopathy rapidly after tissue diagnosis. It is difficult to discern whether he had quiescent disease vs rapid onset of disease that was incidentally found. If he had rapid onset of CLL/SLL, this may argue more toward a common oncogenic cellular pathway between CLL/SLL and HCC. In fact, there is evidence that both cancers are related to the extracellular signal-regulated kinase pathway.15,16
All case reports to date showing a link between HCC and CLL have been in a background of chronic liver disease before HCC.3,4,6 It is noteworthy that our patient lacked a background liver disease including viral hepatitis or hepatic fibrosis before diagnosis of HCC.
In conclusion, our case demonstrates that there may be an association between an atypical presentation of CLL/SLL (characterized by lack of common clinical criteria before tissue diagnosis) and HCC in patients with HCC without traditional risk factors including viral hepatitis and advanced hepatic fibrosis. Further studies will be necessary to provide a possible linking mechanism.
DISCLOSURESAuthor contributions: BH Tu and A. Khalyfa and T. Tanaka wrote and edited the manuscript. AM Bellizzi reviewed the histological images. T. Tanaka is the article guarantor.
Financial disclosure: Tomohiro Tanaka is supported by AHRQ Mentored Clinical Scientist Research Career Development Award (K08): K08HS029195-01A1.
Informed consent was obtained for this case report.
REFERENCES 1. Chidambaranathan-Reghupaty S, Fisher PB, Sarkar D. Hepatocellular carcinoma (HCC): Epidemiology, etiology and molecular classification. Adv Cancer Res. 2021;149:1–61. 2. McGlynn KA, Petrick JL, El-Serag HB. Epidemiology of hepatocellular carcinoma. Hepatology. 2021;73(Suppl 1):4–13. 3. Becker DJ, Sevilla DW, O'Connor O. Concurrent and apposed hepatocellular carcinoma and small lymphocytic lymphoma/chronic lymphocytic leukemia in a patient with hepatitis C virus. Acta Haematol. 2010;123(2):77–80. 4. Lee SI, Heo NY, Park SH, et al. Synchronous hepatocellular carcinoma and B-cell non-Hodgkin's lymphoma in chronic hepatitis C patient. Korean J Gastroenterol. 2014;64(3):168. 5. Heidecke S, Stippel DL, Hoelscher AH, Wedemeyer I, Dienes HP, Drebber U. Simultaneous occurrence of a hepatocellular carcinoma and a hepatic non-Hodgkin's lymphoma infiltration. World J Hepatol. 2010;2(6):246–50. 6. Mogrovejo E, Gjeorgjievski M, Cappell MS. Coexistence of hepatocellular carcinoma and small lymphocytic lymphoma in the absence of pre-damaged liver parenchyma: Case report and review of literature. Am J Gastroenterol. 2015;110:S385. 7. Chernyak V, Fowler KJ, Kamaya A, et al. Liver imaging reporting and Data System (LI-RADS) version 2018: Imaging of hepatocellular carcinoma in at-risk patients. Radiology. 2018;289(3):816–30. 8. Elmberg M, Hultcrantz R, Ekbom A, et al. Cancer risk in patients with hereditary hemochromatosis and in their first-degree relatives. Gastroenterology. 2003;125(6):1733–41. 9. De Moor RA, Schweizer JJ, Van Hoek B, Wasser M, Vink R, Maaswinkel-Mooy PD. Hepatocellular carcinoma in glycogen storage disease type IV. Arch Dis Child. 2000;82(6):479–80. 10. Ohkoshi-Yamada M, Kamimura K, Kamimura H, Terai S. Rare complication of hepatocellular carcinoma in Wilson's disease. JGH Open. 2021;5(10):1220–2. 11. Fan HB, Zhu YF, Chen AS, et al. B-cell clonality in the liver of hepatitis C virus-infected patients. World J Gastroenterol. 2009;15(13):1636–40. 12. Yoffe B, Noonan CA, Melnick JL, Hollinger FB. Hepatitis B virus DNA in mononuclear cells and analysis of cell subsets for the presence of replicative intermediates of viral DNA. J Infect Dis. 1986;153(3):471–7. 13. Ferri C, Monti M, La Civita L, et al. Infection of peripheral blood mononuclear cells by hepatitis C virus in mixed cryoglobulinemia. Blood. 1993;82(12):3701–4. 14. Ali M, Yassin MA. Iron overload in patients with chronic lymphocytic leukemia complicated by autoimmune hemolytic anemia: A case report. Case Rep Oncol. 2020;13(1):219–24. 15. Liu L, Cao Y, Chen C, et al. Sorafenib blocks the RAF/MEK/ERK pathway, inhibits tumor angiogenesis, and induces tumor cell apoptosis in hepatocellular carcinoma model PLC/PRF/5. Cancer Res. 2006;66(24):11851–8. 16. Muzio M, Apollonio B, Scielzo C, et al. Constitutive activation of distinct BCR-signaling pathways in a subset of CLL patients: A molecular signature of anergy. Blood. 2008;112(1):188–95.
留言 (0)