
記住我



Colonoscopy is a procedure with a wide range of applications, both diagnostic and therapeutic. However, it is not without risks.1 Complications such as bleeding, perforation, sedation side effects, and postprocedure pain are not infrequent, and patients are consented for these accordingly.2
Diverticular disease is a common diagnosis globally, particularly in Western countries such as the United Kingdom, where approximately half of the individuals over 50 are affected. Although traditionally associated with older age, it is increasingly found in younger populations and, in some cases, it can progress to diverticulitis, that is, acute inflammation of one or more of the diverticular pouches. Diverticulitis typically manifests with abdominal pain, fever, and change in bowel habit.3
The Diverticular Inflammation and Complication Assessment (DICA) score is used to evaluate and assess the severity and characteristics of diverticular disease. It is calculated based on the following parameters: the extent of diverticulosis, the number of diverticula per colonic region (left, right, or both), the presence and nature of inflammation, and the presence and nature of potential complications.4
Postcolonoscopy diverticulitis (PCD) has been reported as a complication of colonoscopy.5 The literature suggests that this is a rare event with a prevalence along the lines of 0.04% to 0.08%.6 The underlying pathogenesis remains unclear, although several mechanisms have been speculated.7
This report describes 2 cases of PCD we encountered recently in our endoscopy practice, at North Tees and Hartlepool National Health Service (NHS) Foundation Trust, United Kingdom.
CASE REPORT Case 1A 63-year-old woman had a polyp surveillance colonoscopy under the English NHS Bowel Cancer Screening Programme. During the procedure, a total of 9 polyps (all smaller than 5 mm) were identified in the transverse and ascending colon. These were successfully removed via cold snare polypectomy. Diverticula were noted in the sigmoid colon with a DICA score of 2 (reflecting more than 15 diverticula extending through the left and right sides of the colon) without any obvious signs of inflammation (Figure 1).
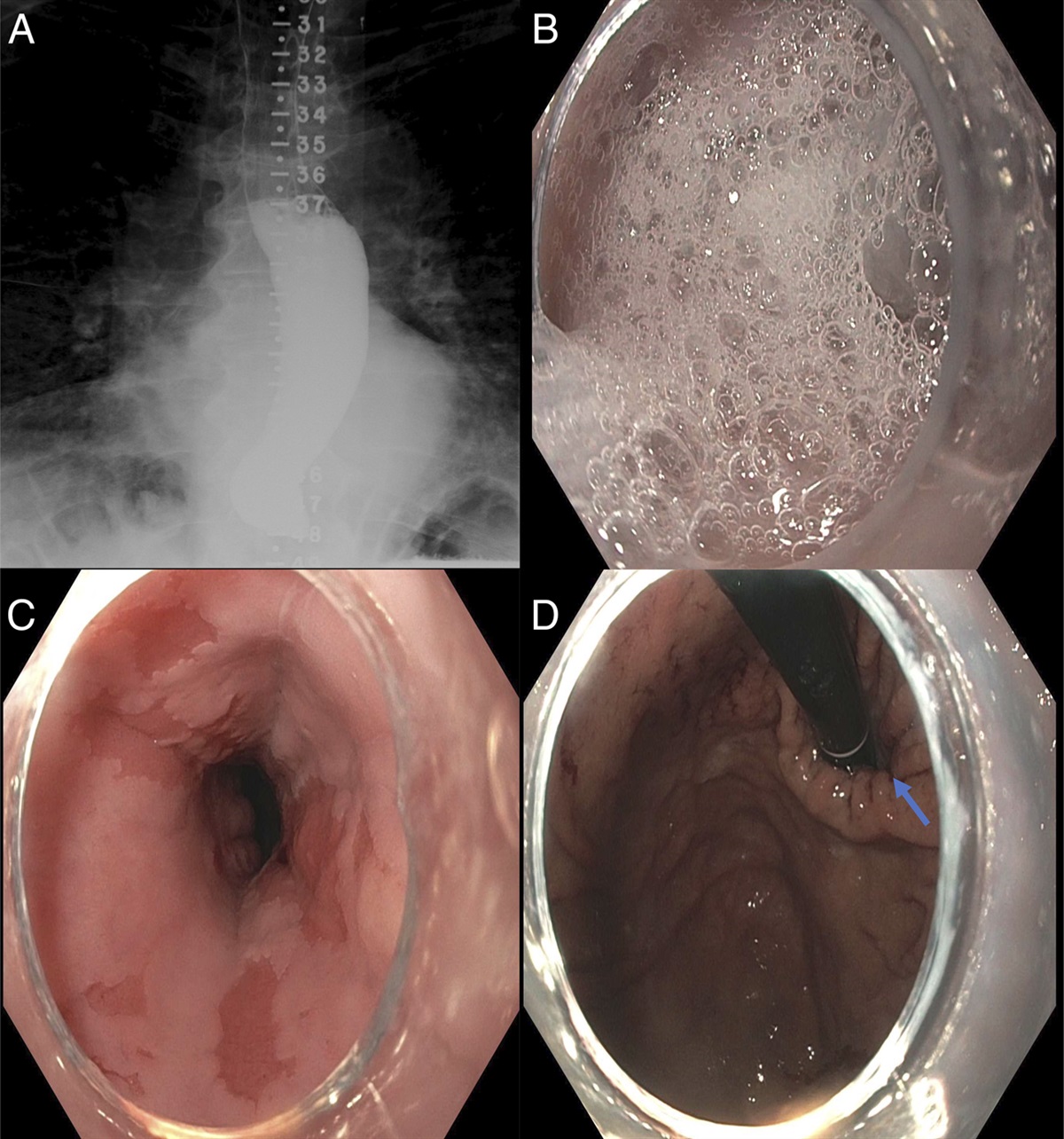
 Figure 1.:
Figure 1.: Colonoscopy showing sigmoid diverticula (A) and small polyps (B).
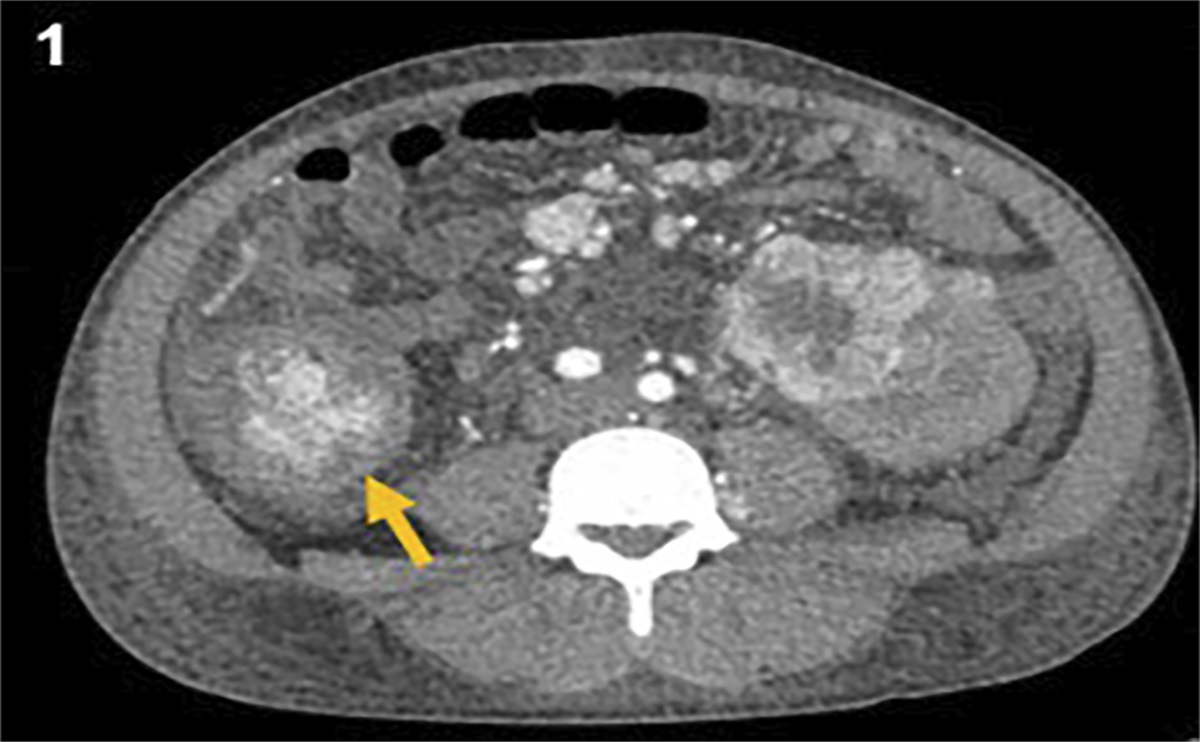
Two days after colonoscopy, the patient developed diffuse abdominal pain and fever. Laboratory tests showed elevated inflammatory markers, with leukocytosis of 18 × 109/L (4.0–11.0 × 109/L) and a CRP (C-reactive protein) of 150 mg/L (0–5 mg/L). A computed tomography (CT) scan confirmed the diagnosis of acute sigmoid diverticulitis, with no signs of perforation or abscess formation.
The patient was admitted and treated with a 5-day course of intravenous antibiotics, consisting of amoxicillin-clavulanic acid and metronidazole. Interestingly, she had a further admission 1 month later with abdominal pain, with a repeat CT revealing ongoing acute diverticulitis changes (again, without signs of perforation or abscess formation). Conservative management resulted in significant improvement in the patient's symptoms, and she was discharged uneventfully (Table 1).
Table 1 - Summary of postcolonoscopy acute diverticulitis cases Age Sex History Indication of colonoscopy preceding diverticulitis Findings Diverticular Inflammation and Complication Assessment (DICA) score Interventions done during the procedure Timing of onset of symptoms Imaging Management 63 Female Chronic codeine intake for joint painsCT, computed tomography; EMR, endoscopic mucosal resection; IV, intravenous.
A 74-year-old woman underwent 2 serial colonoscopies under the NHS Bowel Cancer Screening Programme. During the initial procedure, 6 small polyps (<5 mm) were detected in the ascending colon and cecum, resected using cold snare polypectomy. In addition, a mid-transverse 12 mm polyp was removed via endoscopic mucosal resection (EMR) using a 15 mm hot snare, followed by clipping, and a 40 mm sessile, proximal transverse polyp was left for multidisciplinary team discussion. Owing to marked diverticulosis, the procedure was completed using a slimmer (pediatric) scope (Figure 2).
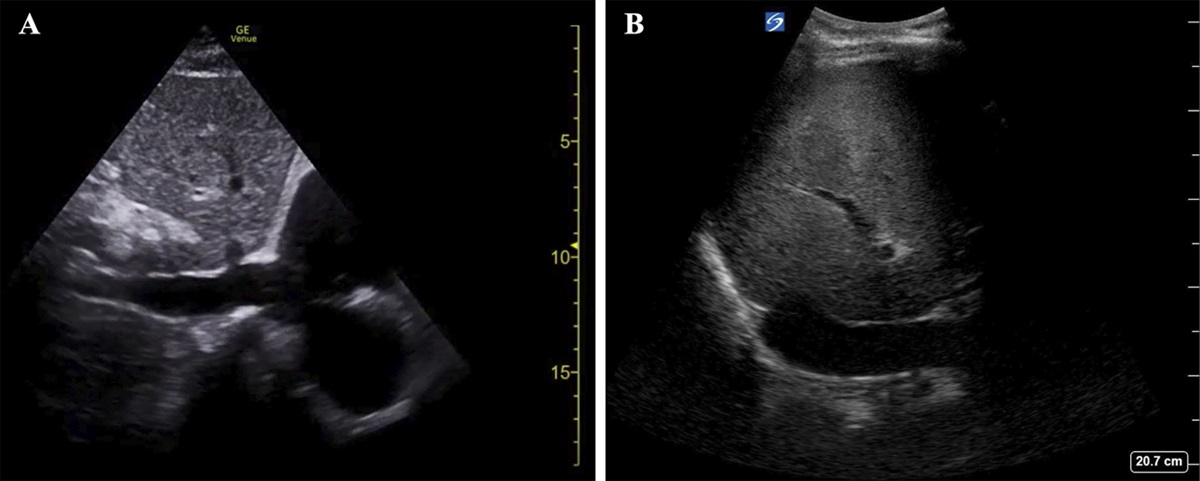
 Figure 2.:
Figure 2.: Scattered diverticula in the cecum (A) and a 40 mm sessile transverse colon polyp (B).
The second colonoscopy was performed a month later with a pediatric scope as well. Piecemeal EMR was performed for the aforementioned 40 mm transverse colon polyp, with a hot snare. Resection was followed by snare-tip soft coagulation and prophylactic clipping (Figure 3). Histopathological analysis showed a tubular adenoma with low-grade dysplasia. Both colonoscopies revealed pancolonic diverticulosis with a DICA score of 2, without endoscopic features of inflammation (Table 2).
 Figure 3.:
Figure 3.: Case 2: Endoscopic mucosal resection defect after snare-tip soft coagulation and clipping.
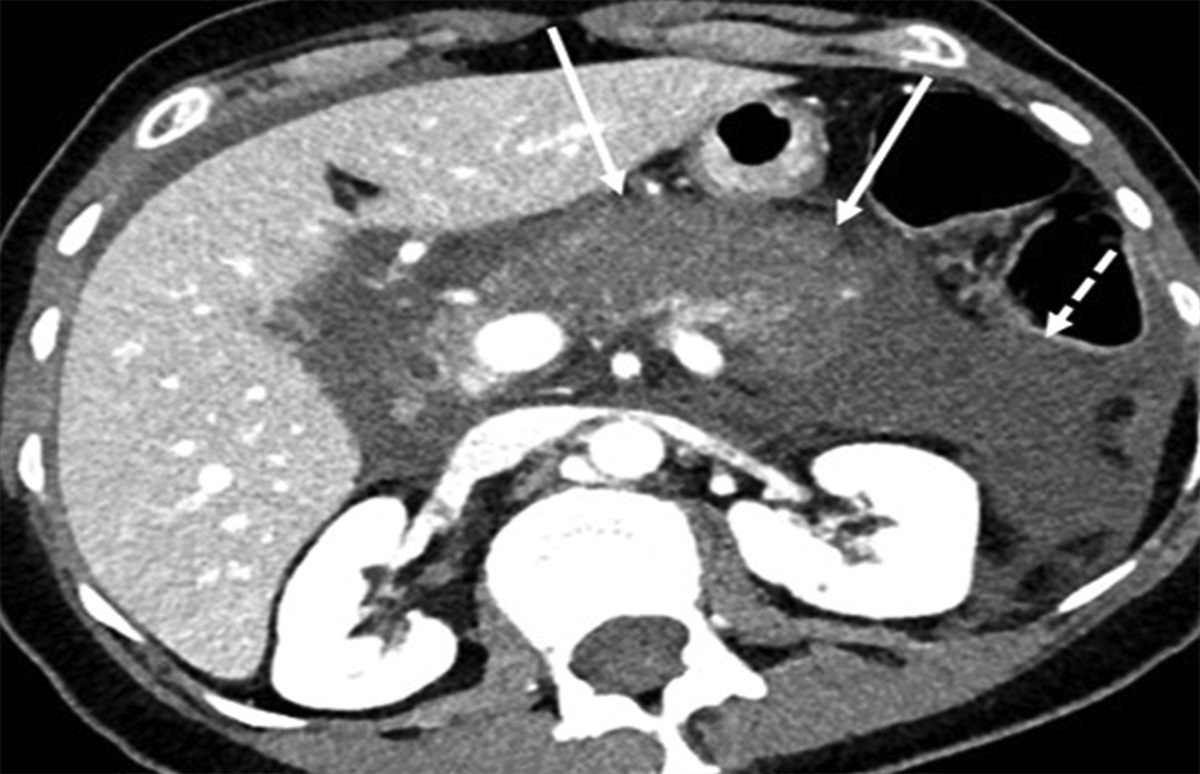
Table 2. - Diverticular Inflammation and Complication Assessment (DICA) simplified score Score Description 0 No diverticula identified 1 Few diverticula (<10), primarily in the sigmoid 2 Moderate diverticula (10–100), throughout the colon 3 Numerous diverticula (>100), throughout the colonFive days following her second colonoscopy, the patient presented with a single episode of mild rectal bleeding, thought to be related to the polypectomy site. The patient had normal hemoglobin and observations, and bleeding stopped spontaneously. As the patient also had lower abdominal pain, fever, and raised inflammatory markers (C-reactive protein of 180 mg/L [0–5 mg/L]), a diagnosis of diverticulitis was felt more likely. Indeed, a CT scan confirmed a diagnosis of severe sigmoid diverticulitis, without signs of perforation (Figure 4).
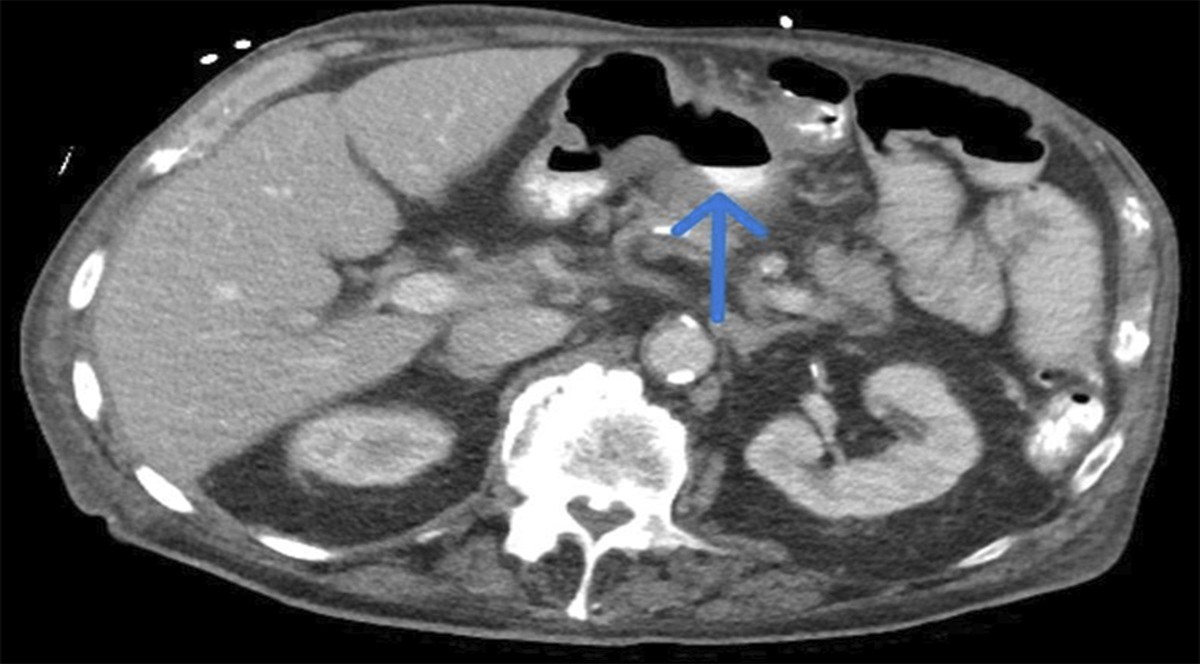
 Figure 4.:
Figure 4.: Case 2: Computed tomography 5 days after colonoscopy, following the patient presenting with symptoms of acute diverticulitis. Features of mural thickening and pericolic fat stranding (arrows).
Considering the patient's stable vital signs and relatively mild abdominal tenderness, a conservative management approach was adopted that required a 2-day hospital admission. The patient received intravenous antibiotics, namely amoxicillin-clavulanic acid and metronidazole, leading to marked clinical improvement (Table 1).
DISCUSSIONColonoscopy is generally considered a safe procedure and is extensively used for diagnostic and therapeutic purposes.8 PCD is defined as the onset of diverticulitis following a colonoscopy. Of note, the finding of acute diverticulitis during colonoscopy does not fall in the definition of PCD. Some authors propose that it should only include cases diagnosed within 3 days from colonoscopy, aligning with the 72-hour time frame proposed for postcolonoscopy appendicitis, as these conditions may share certain mechanisms of how they develop.5,9,10
Several mechanisms of PCD have been described, such as changes in intraluminal pressure due to gas insufflation, accidental insertion of the colonoscope into a diverticulum, and introduction of hard pieces of stool (fecoliths) that may lead to de novo inflammation within diverticula or worsening of existing but subtle inflammatory changes.9 A diagnosis is based on clinical examination, laboratory tests typically suggestive of systemic inflammation, and cross-sectional imaging (CT). Management can be conservative with bowel rest, parenteral hydration, and broad-spectrum antibiotics or surgical in complicated cases (perforation, abscess, or fistula formation) and when symptoms do not resolve with conservative treatment.3
In a systematic review of PCD literature, a prospective study, 4 retrospective cohort studies, and 4 case reports were included.1,5,8,9,11-14 It is worth mentioning that all the reported cases were published by US and Asia Pacific sites and none from UK practices.5
Among the reviewed studies, the 4 case reports highlighted cases of PCD with atypical presentations, characterized by elevated inflammatory markers only.13 Throughout the cases included in the systematic review, diagnostic methods varied, with most of the patients diagnosed through CT. In the group of patients who had scans, some were uncomplicated while others were complicated cases.13 Management approaches varied across studies, including oral antibiotics on an outpatient basis, percutaneous drainage in some cases, and surgery in others. Interestingly, one study noted a significant recurrence rate among patients with PCD during follow-up.9
As PCD typically presents with abdominal pain and systemic symptoms such as fever and malaise, it can mimic postpolypectomy perforation, postpolypectomy coagulation syndrome (PPCS), and postcolonoscopy appendicitis.
PPCS results from thermal damage to the colonic/rectal wall by electrocoagulation during polypectomy. Typically, patients exhibit fever, abdominal pain, signs of localized peritonitis, and elevated white blood cell counts within 1–5 days from interventional colonoscopy. CT scan is often performed that may show localized, limited periluminal gas at areas of endoscopic intervention, but typically shows no signs of free perforation. Management involves hydration, antibiotics, and bowel rest until symptoms settle.15
We acknowledge the similarities in clinical presentation between PPCS and PCD, and some features that may help differentiate between these 2 entities are as follows: PPCS is typically associated with larger or challenging-to-remove polyps with aggressive electrocoagulation techniques. In our first case, all polyps were small and resected with cold polypectomy. The second patient did have a large polyp resected, although resection per se was not reported as challenging by the endoscopist. Of note, the onset of symptoms in our second patient did not align with the typical 12–24-hour time frame seen in PPCS. Furthermore, CT scan findings in our 2 cases were more in keeping with diverticulitis, rather than PPCS, including the fact that CT findings were in keeping with sigmoid colonic inflammation when the first patient's polyps were scattered across the colon and the second patient's large EMR was in the transverse colon.
Postcolonoscopy appendicitis is a rare complication of colonoscopy, to the extent that the link between the procedure and its causation has not been sufficiently established.16
Both of our PCD cases had a DICA score of 2 or more. This observation suggests that a DICA score of 2 or more may be a potential risk factor, regardless of other colonoscopic findings or interventions performed. Further research with a larger sample size and additional case reports would be useful in drawing more definitive conclusions.
As the number of colonoscopies performed worldwide is increasing, even rare complications become relevant and clinicians should be ready to recognize and manage them accordingly.17 In addition, the increasing life expectancy across the globe means that more and more elderly patients undergo colonoscopy and diverticular disease is more common as age advances.5
In summary, PCD is a rare postcolonoscopy complication but, as our case reports demonstrate, can occasionally be met in endoscopy practice and be confused with more common presentations such as perforation or postdiathermy syndrome. Clinicians should be aware of its existence, to identify and manage patients promptly and efficiently. There is paucity of evidence to support that the risk of PCD warrants a change in intraprocedural and postendoscopy recovery practice. However, we would encourage endoscopists to consider measures such as slimmer-diameter endoscopes, use of a scope guide to minimize looping, and water insufflation when scoping patients with known severe diverticulosis. Endoscopy and wider hospital teams should keep PCD in mind when patients present with relevant symptoms following a colonoscopy.
DISCLOSURESAuthor contributions: ME Mahmoud: wrote the manuscript and collected patient data, and is the article guarantor; I. Beintaris and MD Rutter provided patient information and revised the manuscript.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Rutter CM, Johnson E, Miglioretti DL, Mandelson MT, Inadomi J, Buist DSM. Adverse events after screening and follow-up colonoscopy. Cancer Causes Control. 2012;23(2):289–96. 2. Ko CW, Riffle S, Michaels L, et al. Serious complications within 30 days of screening and surveillance colonoscopy are uncommon. Clin Gastroenterol Hepatol. 2010;8(2):166–73. 3. Bhatia M, Mattoo A. Diverticulosis and diverticulitis: Epidemiology, pathophysiology, and current treatment trends. Cureus. 2023;15(8):e43158. 4. Tursi A, Brandimarte G, Di Mario F, et al. Development and validation of an endoscopic classification of diverticular disease of the colon: The DICA classification. Dig Dis. 2015;33(1):68–76. 5. Ng ZQ, Tan JH, Tan HCL, Theophilus M. Post-colonoscopy diverticulitis: A systematic review. World J Gastrointest Endosc. 2021;13(3):82–9. 6. Ko CW, Dominitz JA. Complications of colonoscopy: Magnitude and management. Gastrointest Endosc Clin North Am. 2010;20(4):659–71. 7. Jacobs DO. Diverticulitis. N Engl J Med. 2007;357(20):2057–66. 8. Park SR, Bae YS, Park JI, Min JS, Kim Y. Colonoscopy-Induced acute diverticulitis. J Korean Geriatr Soc. 2016;20(2):108–11. 9. Gorgun E, Isik O, Sapci I, et al. Colonoscopy-induced acute diverticulitis: Myth or reality? Surg Endosc. 2018;32(7):3290–4. 10. Ng ZQ, Elsabagh A, Wijesuriya R. Post-colonoscopy appendicitis: Systematic review of current evidence. J Gastroenterol Hepatol. 2020;35(12):2032–40. 11. Levin TR, Zhao W, Conell C, et al. Complications of colonoscopy in an integrated health care delivery system. Ann Intern Med. 2006;145(12):880–6. 12. Lin J-N, Wang C-B, Yang C-H, Lai CH, Lin HH. Risk of infection following colonoscopy and sigmoidoscopy in symptomatic patients. Endoscopy. 2017;49(8):754–64. 13. Mohan N, Goldstein J. 1638 post-colonoscopy diverticulitis: A rare complication. Am J Gastroenterol. 2019;114(1):S916. 14. Park DS, Park JW, Kim SY, et al. A case of acute colonic diverticulitis as a complication of colonoscopy. Intestinal Res. 2013;11(2):146–8. 15. Kus J, Haque S, Kazan-Tannus J, Jawahar A. Postpolypectomy coagulation syndrome-an uncommon complication of colonoscopy. Clin Imaging. 2021;79:133–5. 16. Shobar RM, Velineni S, Keshavarzian A, et al. The effects of bowel preparation on microbiota-related metrics differ in health and in inflammatory bowel disease and for the mucosal and luminal microbiota compartments. Clin Transl Gastroenterol. 2016;7(2):e143. 17. Kim SY, Kim H-S, Park HJ. Adverse events related to colonoscopy: Global trends and future challenges. World J Gastroenterol. 2019;25(2):190–204.
留言 (0)