
記住我



Clozapine is superior to other antipsychotics for treating positive symptoms of schizophrenia. There is growing evidence that it is just as effective in treating negative symptoms and decreasing relapse rates.1 However, its severe side effect profile limits its use. The following case report demonstrates that clozapine alone can worsen clozapine-induced gastrointestinal hypomotility (CIGH). Its dose increase can also worsen it independently. Its combination with medicines with anticholinergic effects such as quetiapine and benztropine can also lead to CIGH. It is shown that the case fatality rate with CIGH is higher than those with clozapine-induced agranulocytosis. Palmer et al found a mortality rate of 27.5% among patients who used clozapine and subsequently developed gastrointestinal hypomotility.2
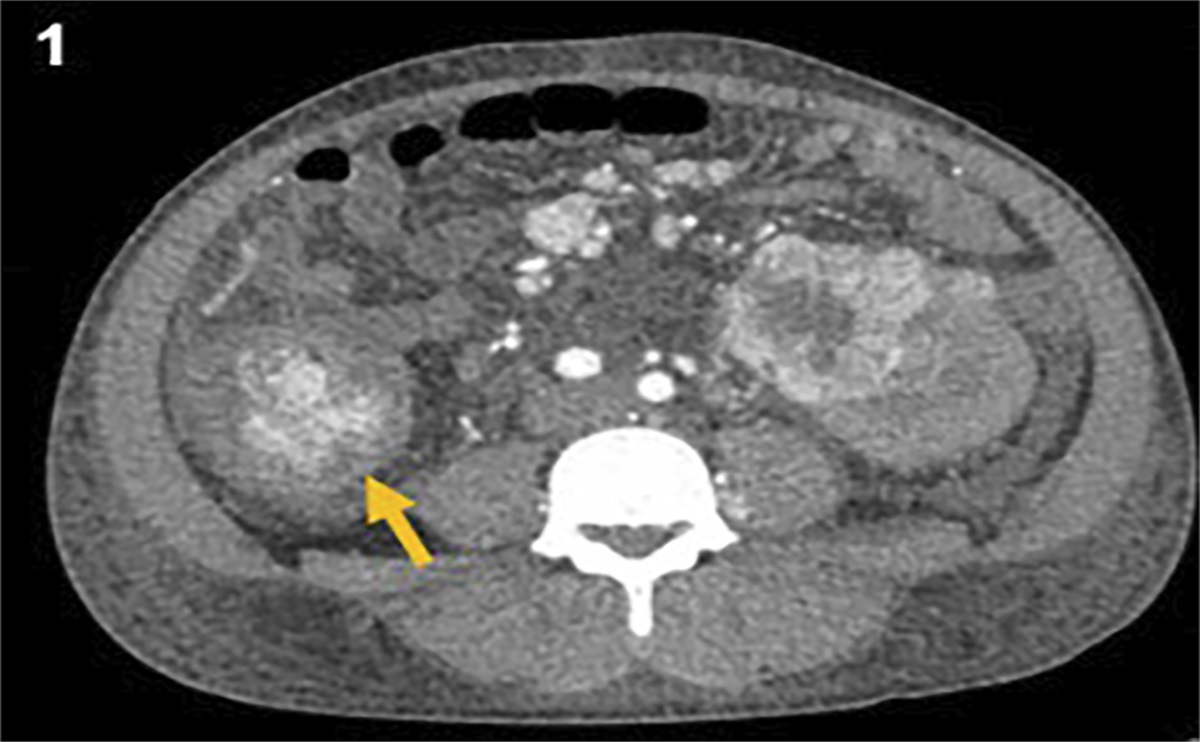
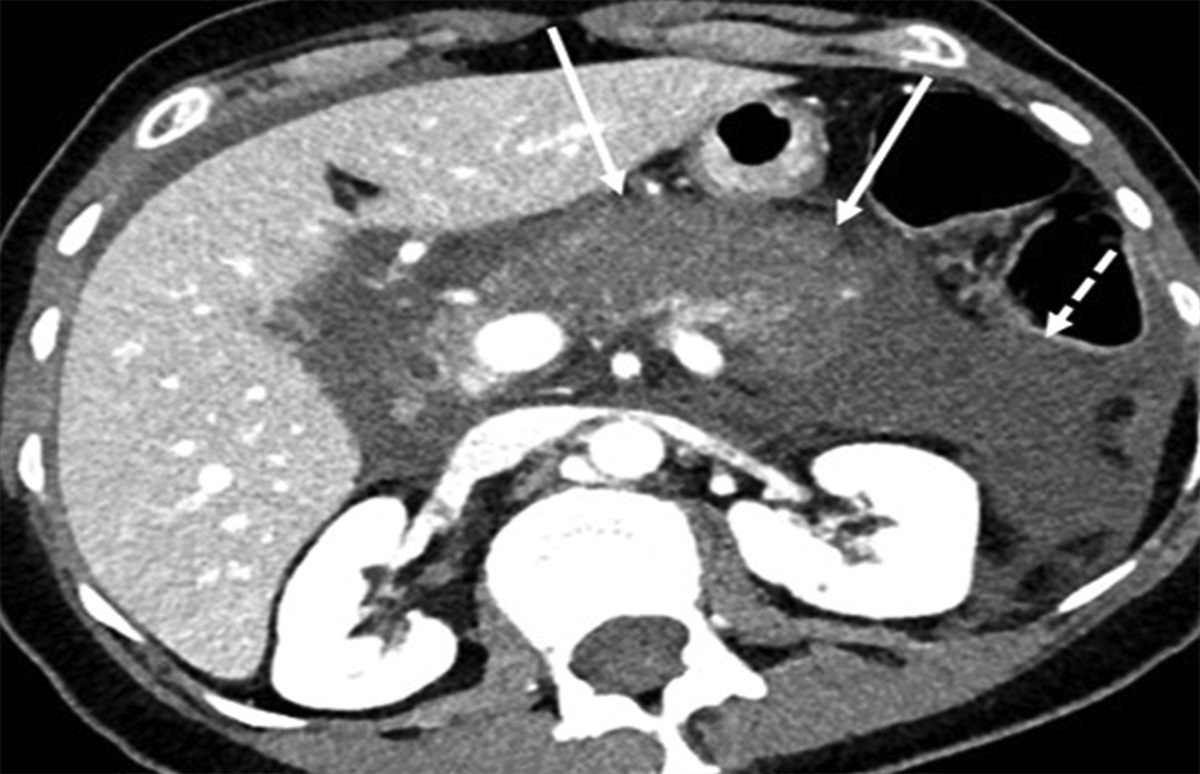
CASE REPORTA 34‐year‐old man from a group home presented to our hospital with a medical history significant for resistant bipolar disorder on quetiapine 400 mg twice daily, intellectual disability, and chronic constipation on senna. Owing to his worsening symptoms related to bipolar disorder, the treatment regimen was modified. Clozapine was added and titrated over 3 months from 100 to 450 mg daily. The bowel regimen was not modified accordingly. His extrapyramidal symptoms were controlled by the addition of benztropine. This worsened his constipation in the form of bloating with reduced frequency of bowel movement to one in every 7–10 days with fecalith. He developed severe diarrhea with multiple episodes of vomiting for 2 days and presented in an unconscious state with gross abdominal distension and thready peripheral pulses. Because of stupor, he was intubated for airway protection and transferred to the intensive care unit on mechanical ventilation. His antipsychotics were discontinued. On examination, he was dehydrated with faint bowel sounds. He was resuscitated with parenteral crystalloids and dual vasopressors due to refractory septic shock. His abdominal imaging revealed evidence of significant bowel distension and fecal impaction (Figure 1). The laboratory results were significant for elevated creatinine at 2 mg/dL, White Blood Cell Count (WBC) of 18,000/mm3, and lactic acid of 10.67 mmol/L. Stool Polymerase Chain Reaction (PCR) was positive for Clostridioides difficile. C. difficile infection and overflow diarrhea due to fecal impaction contributed to profound dehydration. C. difficile infection with functional bowel obstruction explained ongoing vomiting. He was treated accordingly with enteral vancomycin, parenteral metronidazole, bowel rest, nasogastric decompression, mineral oil enema, and manual disimpaction.
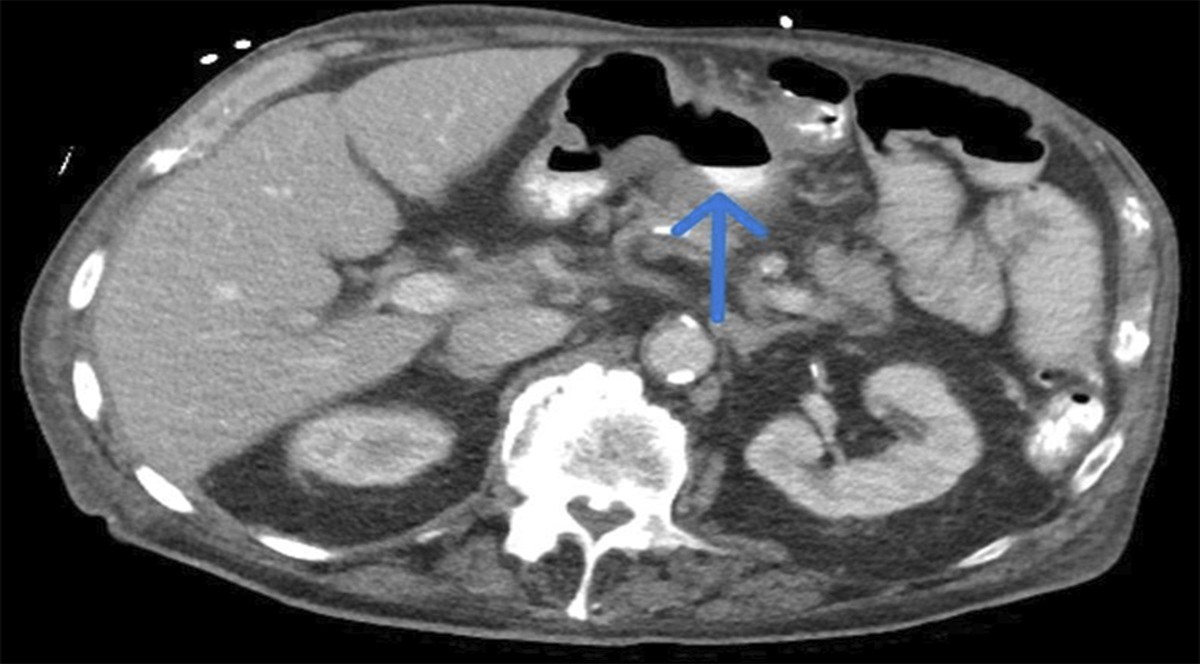
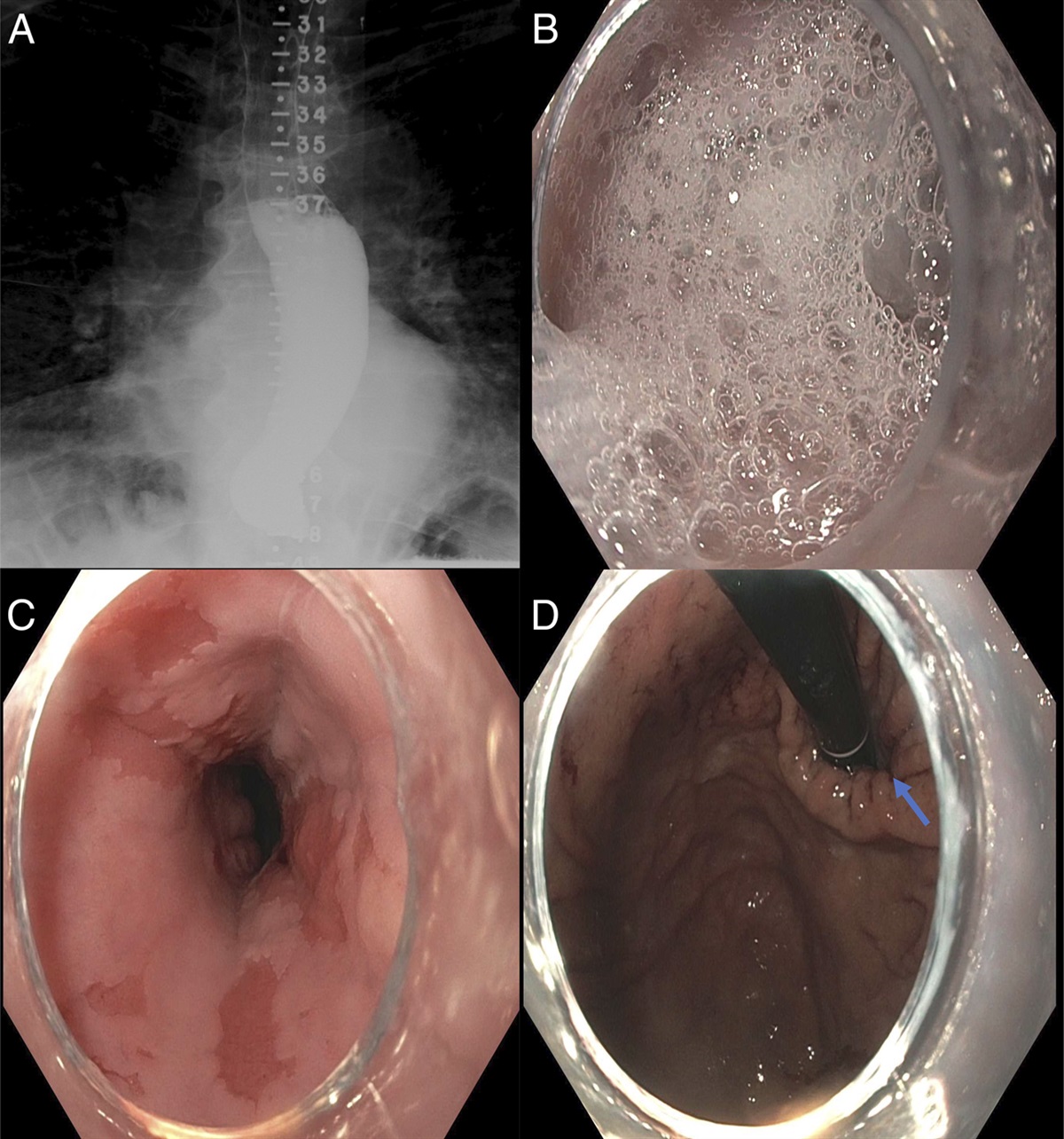
 Figure 1.:
Figure 1.: (A and B) Computed tomography of the abdomen and pelvis without contrast shows a huge rectal stool burden representative of constipation with possible impaction. There are upstream small bowel loops with diffuse heterogeneous mucosal wall thickening consistent with enteritis with possible developing colonic obstruction. (C) X-ray of the abdomen supine shows scattered air and stool-filled mildly dilated small and large bowel loops seen throughout the abdomen suspicious for ileus.
Enteral feeding was gradually advanced. He was weaned off vasopressors on day 5 and from the ventilator on day 7. In-house psychiatry and physical therapy aided in his adequate recovery. He was put on oral sodium valproate 250 mg 4 times daily and lorazepam 1 mg to control his agitation and anxiety, respectively, which was continued on an outpatient basis.
The patient was transferred to the step-down unit on day 10. Clozapine was reintroduced at low dose of 50 mg daily and gradually titrated up to 50 mg 3 times a day in 2 weeks. Quetiapine 50 mg daily and benztropine 1 mg twice daily were added along with citalopram 10 mg daily, polyethylene glycol, senna, and docusate. He was scheduled for outpatient follow-up in 2 weeks with serum clozapine levels. His group home was advised to record his daily bowel movements in a bowel diary.
DISCUSSIONClozapine is the drug of choice in refractory cases of schizophrenia and bipolar disorder, as per the US Clozaril study.3 Its efficacy is noninferior to other antipsychotics for first-line use.4 Clozapine has shown a significant decrease in hospitalization and cost of treatment with a concomitant increase in quality-adjusted life years.1,5–7 Its increased use has also shed light on its lesser known side effect of CIGH.
A 2016 study by Palmer et al showed a possible correlation between colonic transit time and serum clozapine levels.8 Other causes of bowel hypomotility should also be considered. Many patients on clozapine are less communicative, have low functional activity and poor intake of fiber-rich diet, and are on several medications, including opioids. Clozapine does, however, produce a dose-dependent increase in anticholinergic activity. Its side effect on the gut is amplified with an increase in serum concentration of clozapine and norclozapine when used concomitantly with medications having anticholinergic properties such as benztropine and quetiapine.9,10 The prevalence of intestinal side effects, ranging from constipation to bowel perforation, has been reported as high as 33% on clozapine therapy alone.11–13
CIGH is shown to be the most frequent during the first 4 years of starting clozapine.14 Countries such as the United Kingdom, New Zealand, and Australia have already started monitoring bowel health in patients on multiple antipsychotics, including clozapine. In the United States, we have dedicated clozapine risk evaluation and mitigation strategies for monitoring agranulocytosis. No comparable strategies exist for bowel surveillance. The US Food and Drug Administration has definitive guidelines for laxatives when initiating an opioid regimen. Providers are aware of prescribing a stool softener for these patients. With this case report, we strive to bring attention to the importance of monitoring bowel motility in clozapine users to decrease morbidity and mortality due to its adverse effects. Measures targeting gut health and improved motility have resulted in a significant decline in both the prevalence of constipation and hospitalizations for the treatment of CIGH. Adequate use of laxatives decreases cost of health care and increases the quality of life without inhibiting clozapine's psychoactive properties.15
We recommend the following suggestions when prescribing clozapine.
Consider increased bowel habit surveillance at each health visit. Monitor closely for worsening constipation. Serial laboratory results to include serum clozapine levels and complete blood count. Bowel surveillance by diary entry on healthcare follow-up. X-ray of abdomen or intestinal US quarterly for first year, then only if new symptoms arise, and change in medication or medication dosing, or bowel habits. Preemptively add laxative with clozapine prescription. Do bowel monitoring and check bowel frequency, consistency, and defecation symptoms. Utilization of the F3 approach—fluids, fibers, and improvement in functional status. DISCLOSURESAuthor contributions: All authors were involved in conceptualization, reviewing the intellectual content, and determining the accuracy and integrity of the content to be finalized for submission as per the ICMJE guidelines. All authors reviewed and approved the final draft. A. Tiwari is the article guarantor.
Previous presentation: American College of Physicians Michigan chapter; October 20, 2023; Bellaire, Michigan. American Medical Association virtual poster competition; October 19, 2023.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Wagner E, Siafis S, Fernando P, et al. Efficacy and safety of clozapine in psychotic disorders-a systematic quantitative meta-review. Transl Psychiatry. 2021;11(1):487. 2. Palmer SE, McLean RM, Ellis PM, Harrison-Woolrych M. Life-threatening clozapine-induced gastrointestinal hypomotility: An analysis of 102 cases. J Clin Psychiatry. 2008;69(5):759–68. 3. Meltzer HY. Clozapine: Balancing safety with superior antipsychotic efficacy. Clin Schizophr Relat Psychoses. 2012;6(3):134–44. 4. Okhuijsen-Pfeifer C, Huijsman EAH, Hasan A, et al. Clozapine as a first- or second-line treatment in schizophrenia: A systematic review and meta-analysis. Acta Psychiatr Scand. 2018;138(4):281–8. 5. Butler E, Pillinger T, Brown K, et al. Real-world clinical and cost-effectiveness of community clozapine initiation: Mirror cohort study. Br J Psychiatry. 2022;221(6):740–7. 6. Ninomiya K, Saito T, Okochi T, et al. Cost effectiveness of pharmacogenetic-guided clozapine administration based on risk of HLA variants in Japan and the UK. Transl Psychiatry. 2021;11(1):362. 7. Rosenheck R, Cramer J, Allan E, et al. Cost-effectiveness of clozapine in patients with high and low levels of hospital use. Department of veterans affairs cooperative study group on clozapine in refractory schizophrenia. Arch Gen Psychiatry. 1999;56(6):565–72. 8. Every-Palmer S, Nowitz M, Stanley J, et al. Clozapine-treated patients have marked gastrointestinal hypomotility, the probable basis of life-threatening gastrointestinal complications: A cross sectional study. EBioMedicine. 2016;5:125–34. 9. Chew ML, Mulsant BH, Pollock BG, et al. A model of anticholinergic activity of atypical antipsychotic medications. Schizophr Res. 2006;88(1-3):63–72. 10. de Leon J, Odom-White A, Josiassen RC, Diaz FJ, Cooper TB, Simpson GM. Serum antimuscarinic activity during clozapine treatment. J Clin Psychopharmacol. 2003;23(4):336–41. 11. Drew L, Herdson P. Clozapine and constipation: A serious issue. Aust N Z J Psychiatry. 1997;31(1):149–50. 12. Tang WK, Ungvari GS. Clozapine-induced intestinal obstruction. Aust N Z J Med. 1999;29(4):560. 13. Stroup TS, Gray N. Management of common adverse effects of antipsychotic medications. World Psychiatry. 2018;17(3):341–56. 14. Ali RJ, Dalton HR. Gastrointestinal drugs, Aronson JK (ed). Side Effects of Drugs Annual, Vol 31, Elsevier, 2009, pp 573–87 (https://www.sciencedirect.com/science/article/pii/S0378608009031365). Accessed February 21, 2024. 15. Meier P, Seiler WO, Stähelin HB. Bulk-forming agents as laxatives in geriatric patients [in German]. Schweiz Med Wochenschr. 1990;120(9):314–7.
留言 (0)