
記住我



Endometriosis is a benign condition where endometrial glands and stroma grow ectopically outside the uterus in an estrogen-dependent manner. Endometriosis most often occurs in the reproductive years with declining prevalence after menopause as estrogen levels decrease.1,2 Ectopic endometrial tissue is found most frequently within the pelvis and nearby areas such as the sigmoid colon, dome of the bladder, ovaries, and pelvic ligaments; however, extragenital lesions have been reported less commonly in the upper gastrointestinal (GI) tract, diaphragm, urinary tract, and lungs.3 The pathogenesis of endometriosis is complex and yet to be fully elucidated; however, in postmenopausal women, the mechanism is even more undefined. We describe a case of a postmenopausal patient with no known history of endometriosis who presented with hematochezia and abdominal pain, found on esophagogastroduodenoscopy (EGD) to have a 5-mm gastric pyloric polyp consistent with endometriosis on histopathology.
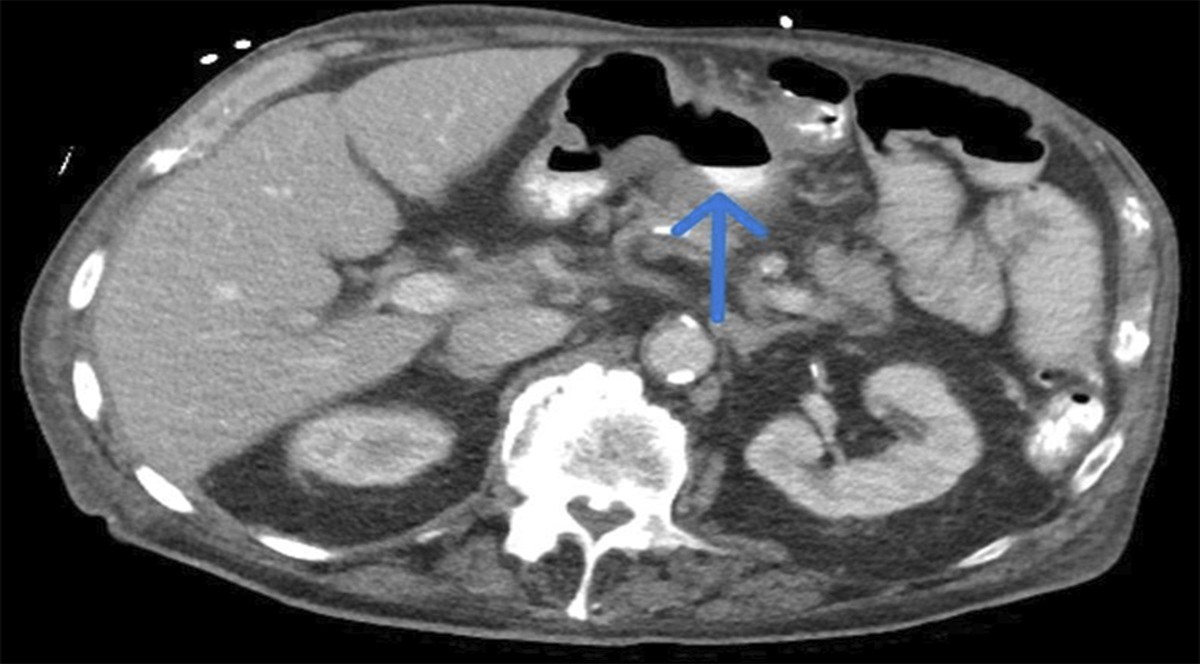
CASE REPORTA 71-year-old postmenopausal woman presented with acute hematochezia and diffuse abdominal pain beginning 3 hours before her visit to the emergency department. She had no fevers, chills, night sweats, nausea, vomiting, dizziness, or unsteadiness. She felt well before this presentation with no history of polyps, GI bleeding, hemorrhoids, or abdominal surgery. She was up-to-date with colorectal cancer screening. While in the emergency department, she had a large bloody bowel movement with associated hypotension (blood pressure 66/45 mm Hg) and a drop in hemoglobin (Hgb) from a previous baseline of 10.0 to 7.0 g/dL. The patient has chronic kidney disease and a chronically elevated blood urea nitrogen (BUN) that rose from 31 to 37 mg/dL with a concurrent rise in creatinine from 1.8 to 2.7 mg/dL during the initial part of her hospitalization. She received 2 units of packed red blood cells with a subsequent hemoglobin increase to 9.6 g/dL. An abdominal/pelvic computed tomography showed uterine calcifications likely representing fibroids, but no other significant abnormal GI findings, adrenal lesions, or a source of bleeding. Helicobacter pylori testing was not obtained. She required admission to the intensive care unit and underwent an EGD and colonoscopy. The EGD was notable for a 5-mm nonbleeding inflammatory-appearing polyp in the pylorus that was removed without complication (Figure 1). The colonoscopy was significant for nonbleeding diverticulosis of the ascending and transverse colon and nonbleeding small internal hemorrhoids. Pathology from the polyp showed variably sized glands lined by cuboidal cells in a crushed cellular stroma, without cytologic atypia (Figure 2). The stromal cells were initially interpreted as an atypical lymphoid proliferation with residual atrophic gastric mucosa. Immunohistochemistry showed stromal cells to be positive for estrogen receptor and CD10, but negative for cytokeratin, and glands positive for estrogen receptor and CD56, markers often positive in endometriosis and adenomyosis (Figure 3). Taken together, these findings were consistent with endometriosis.
 Figure 1.:
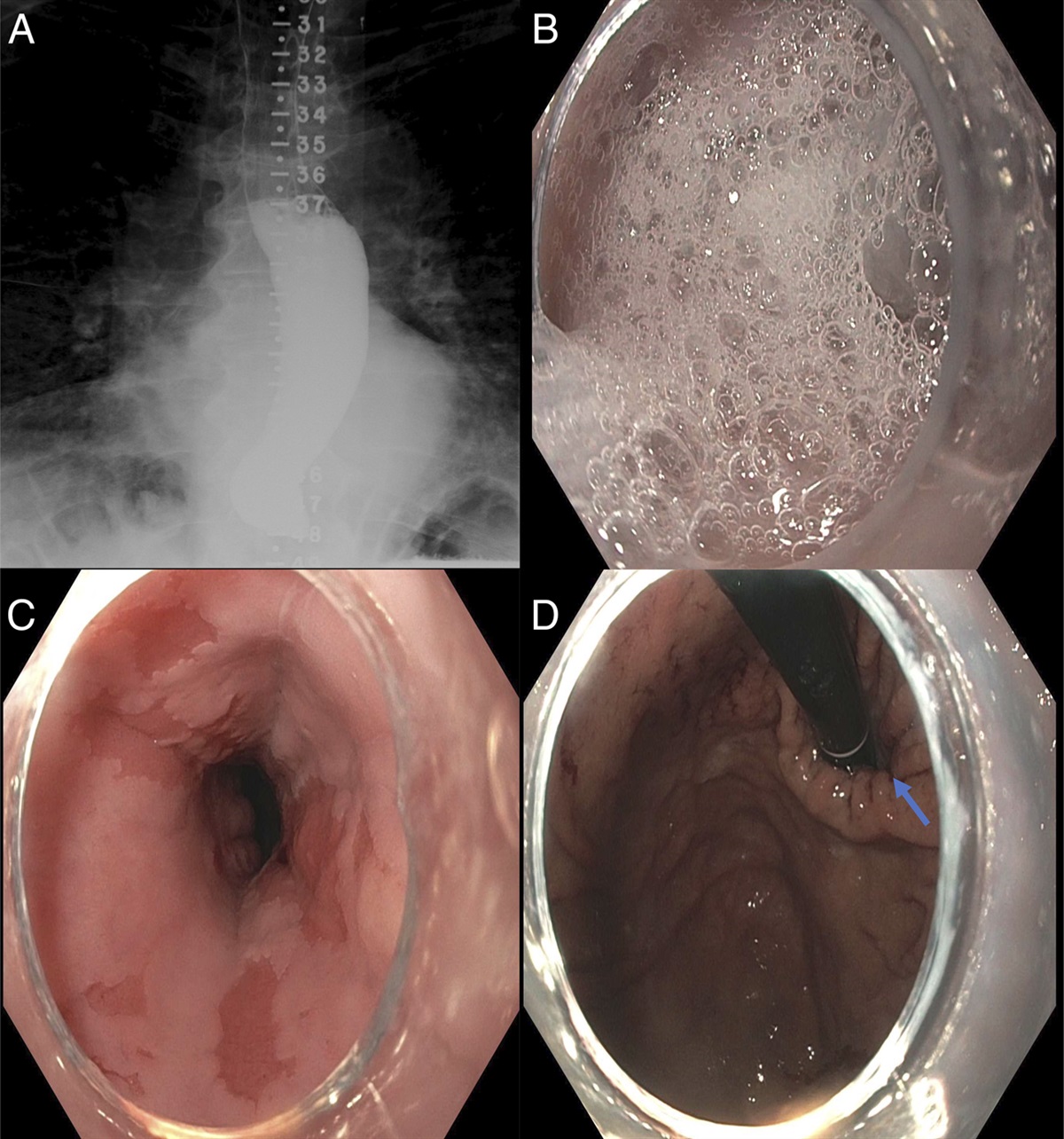
Figure 1.: Esophagogastroduodenoscopy images depicting a 5-mm nonbleeding polyp in the pylorus. View from the antrum (A) and view from the inlet to the pylorus (B).
 Figure 2.:
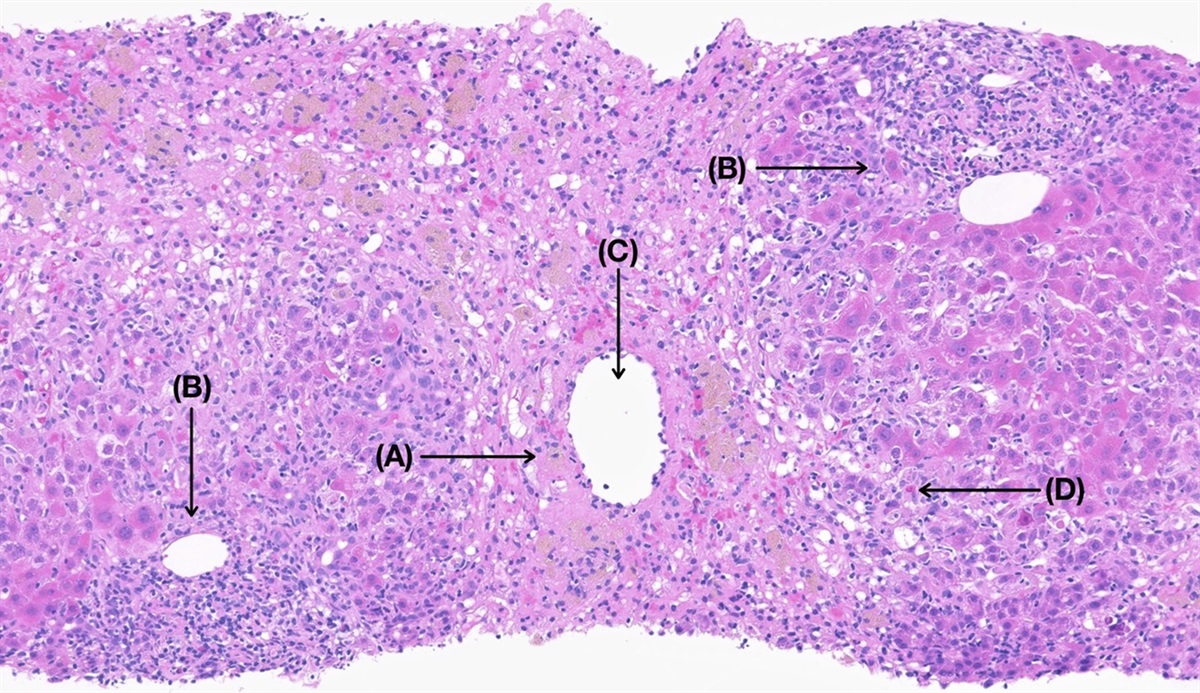
Figure 2.: Histologic section of the polyp demonstrating variably sized glands (arrows) lined by cuboidal cells in a crushed cellular stroma. Panel (A) is stained with hematoxylin and eosin (H&E). Panel (B) is stained with hematoxylin only. Magnification (200×, 20× objective).
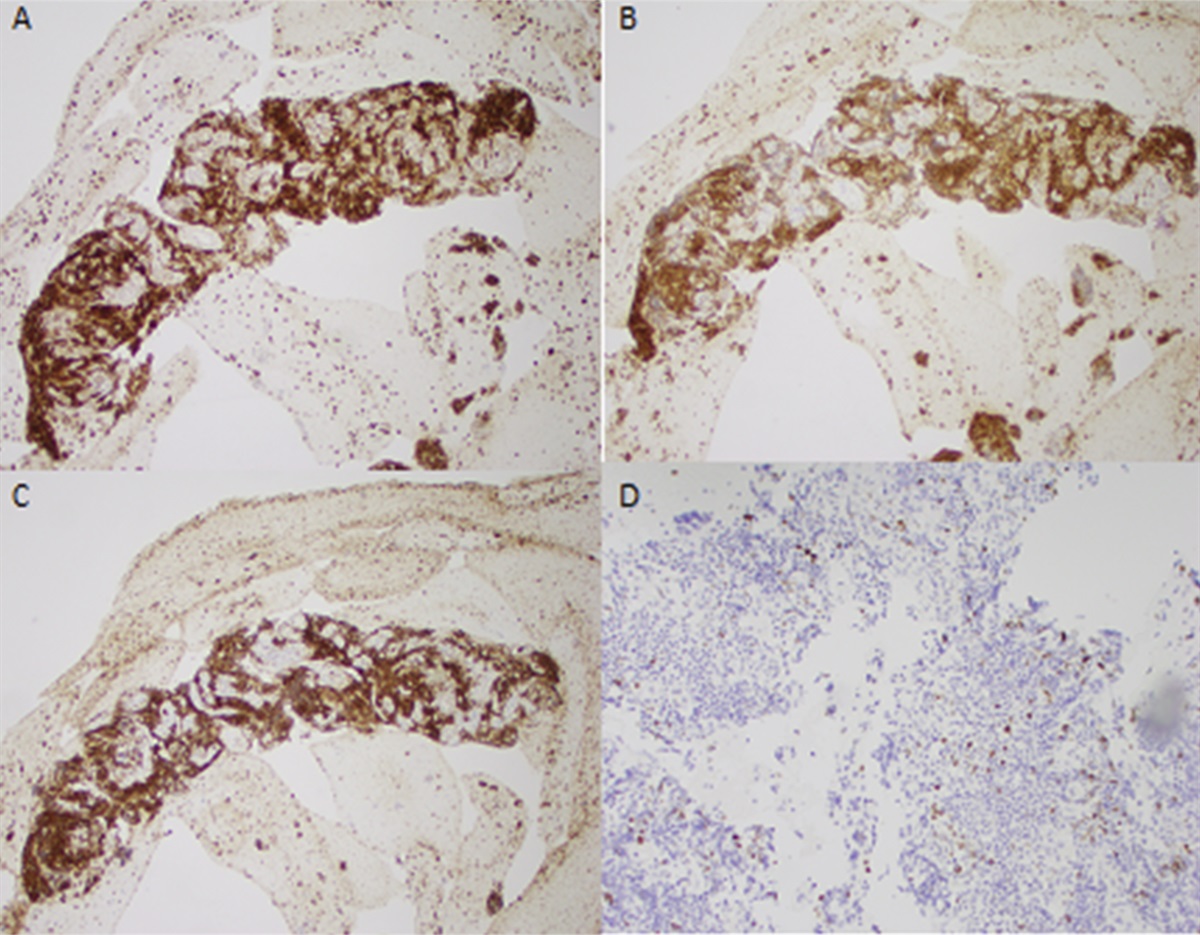
 Figure 3.:
Figure 3.: Immunohistochemistry stains using antibodies as indicated in each panel (CD10, CD56, estrogen receptor, and leukocyte common antigen). Endometrial-type stromal cells are positive for estrogen receptor and CD10 but negative for leukocyte common antigen. Glands are positive for estrogen receptor and CD56, and markers are often positive in endometriosis. Magnification 400×, 40× objective; counterstained with hematoxylin.
DISCUSSIONEndometriosis is defined by the presence of extrauterine endometrial tissue and a subsequent inflammatory response. In reproductive-age women, the prevalence of endometriosis ranges between 6% and 10%, and as women transition into postmenopausal years and estrogen levels naturally decrease, the reported prevalence of endometriosis falls to 2%–5%.2,4 The pathogenesis of endometriosis is complicated and continues to be studied, but current mechanisms include retrograde menstruation of hormone-sensitive endometrial cells into the peritoneal space, differentiation of stem cells that lead to growth of ectopic endometrial tissue, impaired immune regulation and inflammation, genetic mutation, and environmental factors.4–6 Endometriomas are most often found in the pelvic organs but have also been reported in various areas of the GI tract, especially in the sigmoid colon, rectum, and appendix.7
The heterogeneity of endometriosis exists not only in lesion sites but also in reported symptoms and treatment modalities. Some patients remain relatively asymptomatic, whereas others can experience significant and severe symptoms, including abdominal pain, changes in bowel habits or urinary habits, abnormal bleeding, and infertility.8 The most conclusive method of diagnosis and staging for endometriosis is surgical visualization, although magnetic resonance imaging and ultrasonography can also be used.4 Treatment for endometriosis often involves medical and surgical therapy. Pain control with nonsteroidal anti-inflammatory drugs along with hormonal regulation with combined oral contraceptives, progestin therapy, GnRH agonists, and aromatase inhibitors are the most common medical options. However, surgical treatment strategies, which are more definitive for disease management, involve local excision or ablation of ectopic endometrial lesions, oophorectomy, or hysterectomy, if necessary.4 Treatment of these lesions is important for pain control and improvement in infertility but also to prevent malignant transformation of endometrial tissue.9
The case we present is unique for several reasons. This patient presents with endometriosis for the first time when she is postmenopausal. It remains unclear how endometrial tissue grows ectopically in postmenopausal patients who are relatively hypoestrogenic compared with reproductive-age women. In postmenopausal women, estrogen production is mediated by peripheral aromatase conversion of adrenally produced androstenedione.10 There are theories that local estrogen acts on steroid-sensitive receptors and enhances neurogenesis and neovascularization pathways to promote the development of endometriomas, but research continues to be ongoing in this area.2 Furthermore, postmenopausal endometriosis is most often found in the ovaries, although there have been case reports of appendiceal, colonic, and ureteric endometriosis.9,11–13 It seems quite rare to discover endometrial tissue within the stomach pylorus, and to the best of our knowledge, there have been no other published reports of this finding.
Ultimately, despite this patient's presentation, no definitive source of bleeding was identified. From a GI standpoint, it is possible that the pyloric polyp of endometrial tissue was the cause of bleeding, but it remains unknown. If suspicion remains high, an endoscopic ultrasound could be obtained to determine the full extent of the known lesion. Should this patient have recurrent episodes of overt GI bleeding, a repeat EGD followed by capsule endoscopy to evaluate the small bowel would be indicated. If there is clear evidence of bleeding from pyloric endometrial tissue, initial management should focus on controlling the bleed, followed by endoscopic ultrasound to further characterize the extent of the endometrial tissue. Resection with endoscopic mucosal resection is recommended if the endometrial tissue is confined to the submucosa and does not extend beyond 20 mm in depth.14 For endometrial tissue that is between 20 and 30 mm in depth without extending beyond the submucosa, we recommend endoscopic submucosal dissection.14 Finally, for endometrial tissue involving the serosa, we recommend endoscopic full-thickness resection.15 Lesions >5 cm are typically referred for surgical intervention.14
If the endometrial tissue is unable to be removed endoscopically, it will be important to have goals of care discussions regarding the risks/benefits of surgical intervention. This patient will require close primary care and gynecological follow-up along with a pelvic magnetic resonance imaging, which has not been obtained at the time of publication. Typically, routine surveillance is not indicated after the initial staging pelvic magnetic resonance imaging. We want to bring this case to light as symptoms of endometriosis commonly mimic those of GI disease, and we believe that gastroenterologists should be familiar with the basics of endometriosis symptoms, diagnosis, and management.
DISCLOSURESAuthor contributions: SB Minchenberg, L. Burdine, and JL Hecht: wrote the manuscript and approved the final manuscript; KR Falchuk: approved the final manuscript; JL Wolf: edited the manuscript and approved final manuscript.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Mcleod BS, Retzloff MG. Epidemiology of endometriosis: An assessment of risk factors. Clin Obstet Gynecol. 2010;53(2):389–96. 2. Ladanyi C, Boyd S, Sticco P, Mohling S. Postmenopausal endometriosis, where are we now? Curr Opin Obstet Gynecol. 2019;31(4):267–78. 3. Chamié LP, Ribeiro DMFR, Tiferes DA, Macedo Neto AC, Serafini PC. Atypical sites of deeply infiltrative endometriosis: Clinical characteristics and imaging findings. RadioGraphics. 2018;38(1):309–28. 4. Zondervan KT, Becker CM, Missmer SA. Endometriosis. N Engl J Med. 2020;382(13):1244–56. 5. Burney RO, Giudice LC. Pathogenesis and pathophysiology of endometriosis. Fertil Steril. 2012;98(3):511–9. 6. Yu V, McHenry N, Proctor S, Wolf J, Nee J. Gastroenterologist primer: Endometriosis for gastroenterologists. Dig Dis Sci. 2023;68(6):2482–92. 7. Zwas FR, Lyon DT. Endometriosis. An important condition in clinical gastroenterology. Dig Dis Sci. 1991;36(3):353–64. 8. Ballard K, Seaman H, De Vries C, Wright J. Can symptomatology help in the diagnosis of endometriosis? Findings from a national case–control study—Part 1. BJOG Int J Obstet Gynaecol. 2008;115(11):1382–91. 9. Oxholm D, Knudsen UB, Kryger-Baggesen N, Ravn P. Postmenopausal endometriosis. Acta Obstet Gynecol Scand. 2007;86(10):1158–64. 10. MacDonald PC, Rombaut RP, Siiteri PK. Plasma precursors of estrogen. I. Extent of conversion of plasma delta-4-androstenedione to estrone in normal males and nonpregnant normal, castrate and adrenalectomized females. J Clin Endocrinol Metab. 1967;27(8):1103–11. 11. Sooklal S, Ahmad A. Endometriosis of the appendix. Clin Gastroenterol Hepatol. 2021;19(9):e89. 12. Arjonilla M, Khander A, Pal T, Jamorabo D. Intestinal endometriosis leading to recurrent hematochezia. ACG Case Rep J. 2022;9(10):e00872. 13. Zhuang L, Eisinger D, Jaworski R. A case of ureteric polypoid endometriosis presenting in a post-menopausal woman. Pathology (Phila). 2017;49(4):441–4. 14. ASGE standards of practice committee, Forbes N, Elhanafi SE, Al-Haddad MA, et al. American society for gastrointestinal endoscopy guideline on endoscopic submucosal dissection for the management of early esophageal and gastric cancers: Summary and recommendations. Gastrointest Endosc. 2023;98(3):271–84. 15. Cai MY, Martin Carreras-Presas F, Zhou PH. Endoscopic full-thickness resection for gastrointestinal submucosal tumors. Dig Endosc. 2018;30(Suppl 1):17–24.
留言 (0)