Accurate diagnosis and management of patients with 46 XY DSD and chromosomal DSD is very challenging, as it impacts the sex assessment in addition to gonadal management [13]. MDRs in those categories of DSD can present with two different entities: enlarged prostatic utricles (PUs) or vagina masculina (VM) that can arise from the posterior and bulbar urethra, and Müllerian duct cysts (MDCs) which don’t communicate with the urethra [14]. AMH secreted substantially by fetal and prepubertal Sertoli cells plays a pivotal role in activating the regression of the fetal Müllerian duct in males. Moreover, androgens secreted by Leydig cells control the stabilization and differentiation of the Wolffian duct structures and the virilization of the external genitalia. Therefore, MDRs persistence is attributed to either: AMH deficiency or AMH receptor insensitivity [15].
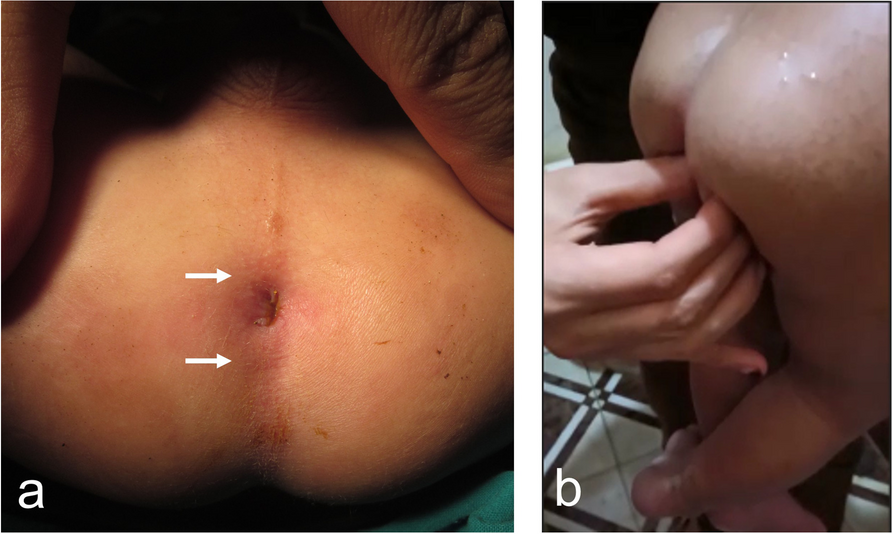
MDRs association with DSD is common, and they have different presentations, among them is accidental discovery during inguinal surgery for palpable gonads. In our study, this was encountered in 3 cases (15%), however, Farikullah et al. (2012) reported 3 cases out of 8 with the same presentation [16]. In our study, 5 cases (25%) had a micropenis and 17 cases (85%) had a hypospadias, with variable severity degrees from mid-shaft to perineal hypospadias. This was in contrast to Sancar et al. (2018), where all cases presented without hypospadias (six cases) [17]. In the current series, 40% of cases presented with a bifid scrotum, 60% with bilateral undescended testis and 40% with unilateral undescended testis. This is comparable to Lima et al. (2004), where 50% of cases presented with a unilateral undescended testis and 50% with bilateral undescended testes [18]. On the other hand, Okur et al. (2003), reported that 100% of cases presented with unilateral undescended testes [19].
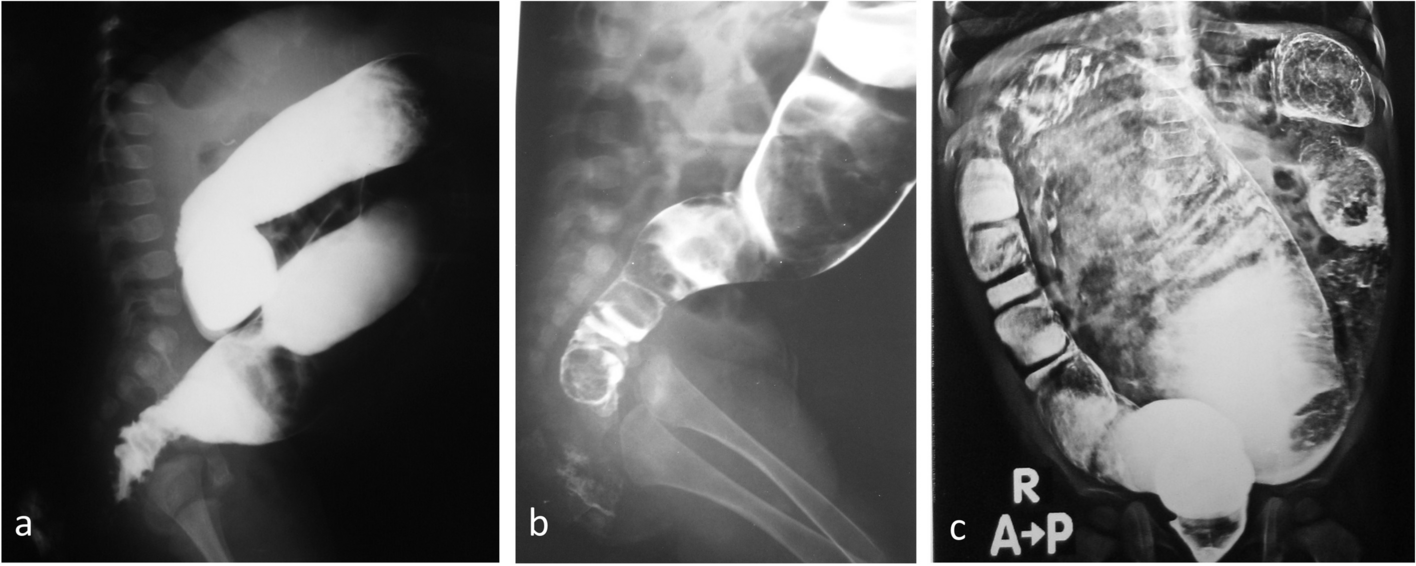
Among patients with 46 XY DSD and mixed gonadal dysgenesis, there is substantial variation regarding the extent of external masculinization and internal anatomy. The role of imaging modality is pivotal to delineate the pelvic anatomy, also to visualize the MDRs [20]. Although US is quick, affordable, available and specific imagining method; it is less sensitive to detect MDRs [20]. The value of US in visualization of MDRs and intra-abdominal gonads is a point of debate. In our work, its value for intra-abdominal gonadal visualization was limited (sensitivity: 36% and specificity: 75%). This was comparable to Shepard et al. (2017) (sensitivity: 38% and specificity: 78%) [21]. Additionally, limited value of US was found in MDRs visualization among our cohort (sensitivity: 25%, 5 out of 20 cases). Previous reports mentioned comparable sensitivity and specificity of US in visualization of MDRs. Steven et al. (2012), mentioned that US succeeded to visualize MDRs in 7 out of 15 cases (47%) and Lima et al. (2004), where US was diagnostic in 2 of the 6 cases (33.3%), equating to a 66.6% false-negative findings [11, 18].
In the current series, laparoscopy successfully visualized MDRs and gonads in all patients. There was a statistically significant difference between laparoscopy and US regarding gonadal and MDRs visualization, being understandably visualized more with laparoscopy, with p values of 0.0180 and 0.001, respectively.
Our finding was supported by previous reports [16, 22] which suggested that pelvic US can be useful preoperative modality but laparoscopy is the gold standard method for proper visualization of MDRs in patients with complex DSD.
However, a larger study is required to compare different modalities such as laparoscopy, MRI and ultrasonography for the evaluation of Müllerian structures in children with complex DSD.



留言 (0)