
記住我
The COVID-19 pandemic has had far-reaching effects on societies, including their health systems and populations. Measures or restrictions implemented to mitigate transmission and reduce the impact of COVID-19 on health systems may have unintentionally led to an increase in illness and death from other causes, that is, HIV/AIDS, tuberculosis, and malaria.1–3 More specifically, the international community feared the pandemic could thwart ongoing efforts globally to prevent HIV infections and ensure access to treatment and care.4 Early studies modeling the potential impact of disruptions in health services in resource-limited settings, taking into account a range of parameters, suggested that in settings with a substantial burden of HIV, tuberculosis, and malaria, mortality from these diseases could increase by 10%, 20%, and 36%, respectively, over a period of 5 years as a result of the COVID-19 pandemic.5,6 Furthermore, early empirical evidence from the Global Fund highlighted the pandemic's impact on prevention and screening services (eg, voluntary male circumcision, the prevention of mother-to-child transmission, HIV self-testing), documenting decreases in access compared with the previous year. HIV testing in particular fell by 22% between 2019 and 2020, resulting in declines in treatment initiation indicators.1,7
West Africa is home to 5 million people living with HIV, two-thirds of whom reside in 5 of the 16 countries in the region.8 The Joint United Nations Programme on HIV/AIDS (UNAIDS) 90–90–90 targets had not yet been achieved before the pandemic despite improvements in timely screening, linkage to care, and sustained access to antiretroviral therapy (ART) in the region.8 While there is evidence that many clinics either closed or reduced their services during the pandemic,9 a large multiregional survey conducted within the International epidemiologic Database to Evaluate AIDS (IeDEA) consortium found that HIV programs in high prevalence and low-income settings introduced or expanded measures to ensure ART adherence and engagement in care.10 Nevertheless, as local program representatives have raised concerns regarding the pandemic's impact on access to HIV viral load (VL) monitoring, the assessment of patient-level data is needed to understand the pandemic period's impact on the provision of HIV care in the region.
We aimed to analyze and document the impact of the COVID-19 pandemic on the number of ART initiations and VL tests conducted before and during the pandemic in adults living with HIV (ALWH) initiating care in urban clinics in Burkina Faso, Côte d’Ivoire, and Nigeria.
METHODS Study Design and PopulationThe IeDEA West Africa (IeDEA-WA) collaboration gathers, harmonizes, and aggregates routinely collected epidemiological and clinical data from 7 HIV programs in Benin, Burkina Faso, Côte d’Ivoire, Nigeria, and Togo. The IeDEA-WA database comprises nearly 50,000 ALWH (18 years or older) who have ever started ART. The collaboration's overarching aim is to identify individual and structural barriers associated with the continuum of HIV care throughout West Africa (http://iedea-wa.org). Moreover, the IeDEA consortium conducts periodic assessments of its participating sites to better understand HIV-related health services delivery. In 2020, specific questions regarding the COVID-19 pandemic were added to the site assessment survey to better comprehend how the pandemic period had affected the availability, accessibility, acceptability, and the quality of HIV services.10 For this analysis, data from the last version of the IeDEA-WA Merger (version 8, April 13, 2022) were used. Owing to missing values and inconsistencies in data from 2 sites, we have restricted this analysis to 5 participating sites in 3 countries: Burkina Faso (Hôpital De Jour, Bobo Dioulasso), Côte d’Ivoire (Centre de Prise en charge de Recherche et de Formation, Centre Intégré de Recherches Biocliniques d’Abidjan, Centre National de Transfusion Sanguine, Abidjan), and Nigeria (The Nigerian Institute of Medical Research, Lagos). We included ART-naïve ALWH with a first visit date after January 1, 2018, and followed them until date of database closure (June 14, 2021, in Burkina Faso, May 12, 2021, in Côte d’Ivoire and April 14, 2022, in Nigeria).
In Burkina Faso, HIV services have been expanded, both decentralized to lower-level health facilities and integrated into primary care. In 2018, 70% of PLWH knew their HIV status and 88% of them were on ART.11
Similarly, in Côte d'Ivoire, achieving the UNAIDS 90–90–90 targets has been prioritized. The national HIV program that includes prevention, testing, and treatment services has been integrated into the broader health system since 2003. Notably, the Ministry of Health has centralized VL monitoring at the national laboratory. In 2018, 63% of PLWH knew their HIV status, 87% of them were on ART, and 75% of those on treatment had suppressed viral loads.11
In Nigeria, HIV prevalence was estimated at 1.4% nationally in 2018, representing 1.9 million PLWH and the highest HIV burden in the region.11 While significant progress has been made in expanding access to HIV services, PLWH's access to HIV care and treatment services continues to be hindered by various factors, including geographical disparities, limited resources, and societal challenges. Efforts have been made to address these barriers and improve access to HIV services with significant success. In 2018, 67% of PLWH knew their HIV status, 80% were on ART, and of those on ART, 80% were virally suppressed.12
Demographics, ART Initiation, and HIV VLSex and age were documented at enrollment date and the latter categorized in 4 categories: 18–24, 25–34, 35–39, and 40+ years old. We defined enrollment in care as date of first visit in the center, date of database closure as the last visit date documented in the merger, and the date of the start of the pandemic as date of first distancing measures put in place in the country.13 ART initiation was defined as the first date of ART treatment documented in the database and HIV VL monitoring as each documented test performed at the laboratory level.
Statistical AnalysesWe described demographic data at enrollment and summarized characteristics before and after the pandemic. We defined the beginning of the “pandemic period” as March 27, 2020, in Burkina Faso, April 9, 2020, in Côte d’Ivoire, and March 30, 2020, in Nigeria, reflecting when physical/social distancing measures were enforced nationally.14 We plotted crude summaries of the 2 outcomes by year and country. We performed a regression discontinuity analysis to estimate changes in the number of ART initiations and VL tests performed before and after the beginning of the pandemic, stratifying by country, using a regression discontinuity design.15,16 For this, we used local polynomial regression models within data-driven Imbens-Kalyanaraman bandwidth intervals, derived using a rectangular (uniform) kernel to estimate risk differences just before and just after pandemic as follows: E [Yi|Zi] = β0 + β1Zi + β2 × 1 [Zi ≥ 0] + β3Zi × 1 [Zi ≥ 0] where Yi is the probability of observing the outcome of interest, Zi is the number of days between ART initiations' date and date of start of pandemic (negative for ART initiation before), and 1[Zi ≥ 0] indicates initiation on or after the date reflecting the beginning of the pandemic. Calculated using the subset of observations within Imbens-Kalyanaraman bandwidth intervals, the effect of interest is the difference in local linear predictions at the threshold (ie, as the threshold is approached from above vs below). We used the Rdrobust function to implement conventional local polynomial regression discontinuity (RD) effect point estimators and confidence intervals to assess differences in crude point (p) changes per week in testing in the prepandemic and postpandemic periods. To present the effect of the pandemic on the 2 outcomes of interest, we plotted binned sample means, tracing out the underlying regression function. All statistical analyses were performed using STATA 16.1 (StataCorp, College Station, TX).
Ethics StatementThe IeDEA-WA Collaboration was granted approval from the Ethics committee “Comite de Protection des Personnes Sud-Ouest et Outre-mer III” in Bordeaux, France (IRB00012788), to collect, merge, and analyze deidentified data from involved HIV clinics in West Africa. Moreover, each participating site obtained approvals from their National Ethics committees (Côte d’Ivoire: IRB00009111; Burkina Faso: IRB00004738; Nigeria (NIMR): IRB00003224). Written informed consent requirements were deferred to the local Institutional Review Boards. The analysis only used deidentified data collected from routine clinical care.
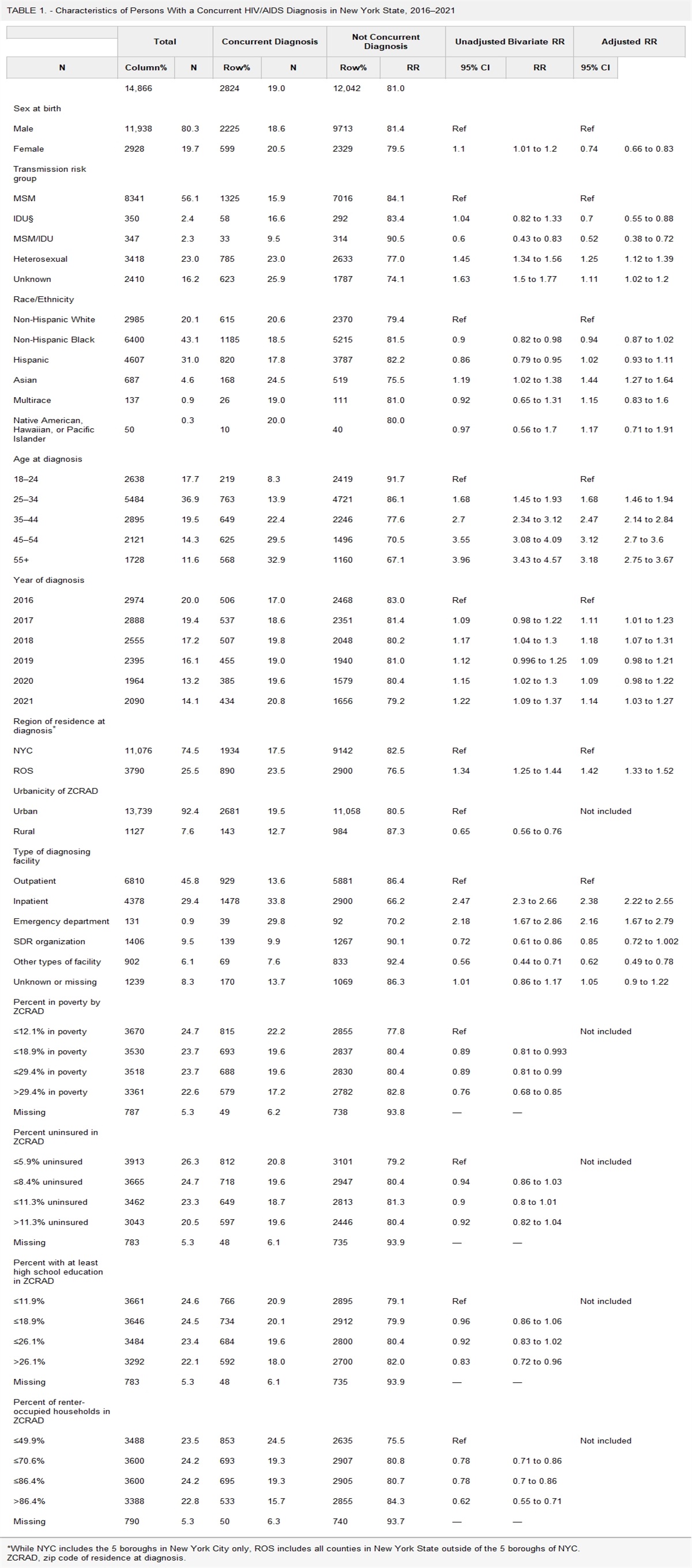
RESULTSA total of 3734 ALWH initiated ART between the January 1, 2018, and the database closures: 832 (22.3%) in Burkina Faso, 1562 (41.8%) in Côte d’Ivoire, and 1340 (35.9%) in Nigeria. ALWH initiating ART were of similar in terms of age before and during the pandemic period in clinics in Burkina Faso and Côte d’Ivoire, while in the clinic in Nigeria, they were older before compared with during pandemic period (median age 39 [interquartile range 30–46] versus 51 [interquartile range 46–57], respectively, P < 0.001). No differences in terms of sex at ART initiation were found in clinics in Burkina Faso; however, in the Nigerian clinic, fewer were men (37.0% versus 42.4%, respectively, P = 0.05) and in Ivoirian clinics, fewer were women (57.4% versus 66.4%, P = 0.002) during pandemic compared with before (Table 1).
TABLE 1. - Sex and Age of ALWH Initiated on ART* (N = 3734), by Period and Site Bobo Dioulasso*Initiated between January 1, 2018, and date of database closure for each country—Database close in Burkina Faso June 14, 2021, Côte d’Ivoire May 12, 2021 (first closure date of 1 of the 3 sites), Nigeria April 14, 2022.
†Pre-COVID in Burkina Faso <March 27, 2020, pre-COVID in Côte d’Ivoire <April 9, 2020, pre-COVID in Nigeria <March 30, 2020.
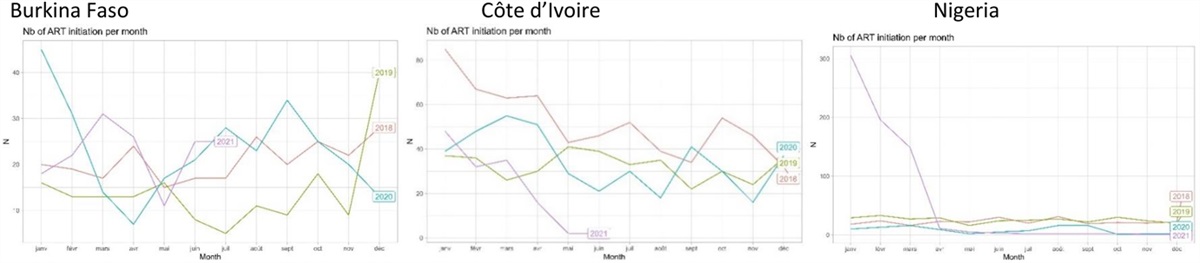
In Figures 1 and 2, we describe the numbers of ART initiations and VL tests performed, by year and by country. In Burkina Faso, the number of ART initiations remained relatively stable over the years, with a decrease observed at the beginning of the pandemic period (April 2020). Similarly, in Côte d'Ivoire, the number of ART initiations showed a consistent pattern, with a slight decline during the pandemic (May–July 2020 and April 2021). In Nigeria, there was a notable increase in the number of ART initiations in the beginning of 2021, above prepandemic levels.
 FIGURE 1.:
FIGURE 1.: Evolution of ART initiations, by year and country.
 FIGURE 2.:
FIGURE 2.: Evolution of VL monitoring, by year and country.
Regarding VL monitoring, in Burkina Faso, the number of VL tests performed declined drastically after the beginning of the pandemic and remained below the prepandemic levels. In Côte d'Ivoire, the number of VL tests remained stable with a slight decrease at the beginning of the pandemic and a sharp decline in April, 2021. In Nigeria, the number of VL tests declined during the pandemic, with a dip observed at the beginning of the pandemic, but eventually returning to prepandemic levels in 2021.
We plotted the results of the regression discontinuity for the number of ART initiations (Fig. 3) and the number of VL tests performed (Fig. 4) for each country. In Burkina Faso and Côte d’Ivoire, the number of ART initiations per week did not significantly change throughout the pandemic period, with a change of −0.24 p and −0.9 p, respectively (95% CI: −5.5 to 5.9 and −8.5 to 8.6, respectively). By contrast, at the clinic in Nigeria, we found the number of ART initiations to have significantly decreased (−6.3 p [95% CI: −10.8 to −1 0.7]), although the number appears to gradually increase over the course of the pandemic period (Fig. 3). By contrast, in all 3 countries, the number of VL tests decreased significantly during the pandemic compared with the prepandemic period, representing −17.0 p (95% CI: −25.3 to −8.6) in Burkina Faso, −118.4 p (95% CI: −171.1 to −65.8) in Côte d’Ivoire, and −169.1 p (95% CI: −282.6 to −55.6) in Nigeria.
 FIGURE 3.:
FIGURE 3.: Plots of regression discontinuity analysis for ART initiations by country.
 FIGURE 4.:
FIGURE 4.: Plots of regression discontinuity analysis for VL monitoring by country.
DISCUSSIONDespite strict physical and social distancing measures and reported reduced availability of HIV services, we found evidence to support that access to ART was maintained for ALWH in clinics in Côte d’Ivoire and Burkina Faso but was somewhat disrupted in the clinic in Nigeria. By contrast, VL monitoring was found to be severely compromised in all settings during the pandemic period. Furthermore, VL monitoring did not return to prepandemic levels 1 year after start of the COVID-19 pandemic. Examining actual changes in individual patient-level data, we have provided a more comprehensive understanding of the pandemic's impact in major centers for HIV care in Burkina Faso, Côte d'Ivoire, and Nigeria. Our study confirms predicted impacts on HIV services while highlighting country-specific challenges and the importance of tailored strategies during crises like the COVID-19 pandemic.
Our analysis of the site assessment (see Table 1, Supplemental Digital Content, https://links.lww.com/QAI/C257) corroborated observed disruptions in HIV services during the COVID-19 pandemic. HIV testing/diagnostic services, enrollment of new patients, and HIV VL monitoring were suspended or limited in the 3 countries. Stockouts of supplies for VL testing were also reported. As previously described, HIV testing and diagnostic services were suspended or reduced in a considerable number of countries within the IeDEA consortium.10 This is of great concern as it can impede timely diagnosis and ART initiation, threatening ALWH's prognosis. Furthermore, the suspension of HIV VL collection and longer turnaround times for results may have implications for treatment monitoring and timely adjustment of ART regimens, potentially leading to suboptimal treatment outcomes. In addition, our study focused on ART initiations, providing insight into treatment uptake among individuals diagnosed with HIV. However, it does not directly reflect access to HIV testing during the pandemic. Further investigation is warranted to examine the extent to which testing activities were affected and whether there were any disparities in HIV testing rates across different age groups. An understanding of the dynamics between HIV testing and ART initiations would provide a more comprehensive picture of the impact of the pandemic on the HIV care continuum and guide targeted interventions to address gaps in testing and treatment access. In other regions, significant reductions in HIV testing activities have been described and highlighted as a consequence of the COVID-19 pandemic.17,18
While no significant differences in the average number of ART initiations per week by period were found in the clinics in Burkina Faso and Côte d'Ivoire, the clinic in Nigeria did experience a significant decrease in the number ART initiations during the pandemic period compared with the prepandemic period, albeit with a gradual recovery over time. The maintenance of levels of ART initiations in Burkina Faso and Côte d’Ivoire is consistent with a recent President's Emergency Plan for AIDS Relief report, which confirms the effectiveness of HIV programs in mitigating the impact of the COVID-19 pandemic.19 Furthermore, in Côte d’Ivoire, investigators in 1 of the 3 clinics reported that community ART pick-up points had been set-up to ensure continued access to ART in the context of social distancing measures (see Table 1, Supplemental Digital Content, https://links.lww.com/QAI/C257), pointing to healthcare providers' adaptability and resourcefulness. The decrease in ART initiations in the clinic in Nigeria may reflect disruptions in access to the clinic or other barriers encountered by ALWH during the pandemic (eg, fear of infection). Another possible explanation may be fewer diagnosed HIV infections in 2021, which have been reported in Nigeria, resulting in the observed difference in the average number of ART initiations.4 Key strategies, including community-based HIV care, may have helped to maintain access to ART during the pandemic despite restricted access to clinics.19 Nonetheless, the significant drop in ART initiations in the clinic in Nigeria together with the higher proportion of women initiating ART during the pandemic may be in line with results of previous studies finding poor access to HIV testing services among men in Nigeria.19–21 Targeted interventions are needed to ensure continued access to HIV testing and ART initiation, including proactive measures to reach those who may have not been tested as a result of these service disruptions.
All clinics experienced a significant reduction in the volume of HIV VL testing during the pandemic. This decline in testing raises concerns about the effectiveness of treatment monitoring among ALWH and its impact on clinical outcomes and long-term prognosis.22,23 HIV VL monitoring is a crucial component of HIV care, enabling healthcare providers to assess treatment response, detect virologic failure, and optimize treatment regimens.24 Furthermore, all 3 countries follow World Health Organization guidance calling for HIV VL testing at 6 months after ART initiation and viral suppression at 1 year.25 The observed decreases in HIV VL testing underscores the need to strengthen laboratory services, ensuring consistent availability of testing supplies, and addressing logistical challenges to maintain reliable and timely testing services. The survey conducted by the IeDEA consortium also found similar disruptions, including the suspension of VL monitoring, longer turnaround times for results, stock outs of essential supplies, and laboratories not accepting HIV VL samples.10 These documented operational challenges likely underlie our findings. Furthermore, our findings are consistent with reports from other African settings that have highlighted the impact of the pandemic on HIV VL monitoring and subsequent management of treatment failure.26,27 While it is possible that the pandemic period affected ART adherence despite evidence of maintained access to ART, interruptions in VL monitoring hamper an in-depth assessment of the proportion of those in care who have achieved/maintained virological suppression.
Further research is needed and will be conducted in a multiregional analysis across low- and middle-income countries within the IeDEA consortium. This will provide a broader perspective on the challenges faced in different settings. A comprehensive understanding of the medium to long-term consequences of the pandemic on HIV care requires examining a larger sample of countries and considering additional outcomes. This research will provide insights into the evolving landscape of HIV services, enabling targeted interventions.
Strengths and LimitationsOur study provides complementary evidence regarding the impact of the COVID-19 pandemic on ART initiations and VL monitoring in major urban clinics in 3 West African countries, highlighting similarities but also intraregional differences. While mathematical models had predicted a potential impact on HIV services at the beginning of the pandemic, our analysis goes beyond assumptions and examines the actual changes observed. It uses routine programmatic data, providing insights into the “real-world” implementation of HIV services both before and during the pandemic. This approach has contributed to the generalizability of our findings.
Nevertheless, our findings should be interpreted with some caution. First, this analysis relied on routine programmatic data which, while valuable for assessing real-world trends, may be subject to incomplete or missing data, variations in data collection practices across different healthcare facilities, and reporting biases. As our collaboration relies on data from a limited number of clinical centers in each country, we acknowledge the risk of information bias. For example, ALWH may initiate care (ART) at one clinic and then be followed-up at another. Unfortunately, the transfer of ALWH between clinical centers is not captured. While these transfers are not uncommon in ALWH on ART, they are less likely among those starting ART. It is unclear whether this phenomenon (patient transfer) was more or less likely during the pandemic compared with the prepandemic period. Second, as only limited demographic characteristics were available, our ability to capture individual-level variations or factors influencing ART initiations and HIV VL monitoring was limited. In addition, our findings are based on data from urban clinics and may not be fully representative of dynamics in clinics nationally, particularly those in primary or secondary care in rural settings. The characteristics and challenges of HIV services in rural or remote areas could differ significantly, and therefore, caution should be exercised when generalizing the results nationally.
As the experiences of these clinical settings during the COVID-19 pandemic and their responses varied, it is crucial to recognize that the impact on HIV services and the effectiveness of programmatic adaptations may differ across the West African region. Furthermore, the timing of the database closure varied across countries, which may have influenced the completeness and comparability of the data. While our study has primarily focused on average changes in volume before and during the pandemic, contributing valuable, albeit macro-level, insights regarding the COVID-19 pandemic's impact on HIV services, it does not consider the perspectives of ALWH, which could provide additional insights into the challenges faced during the pandemic.
CONCLUSIONSHIV clinics in 2 of 3 countries in West Africa demonstrated resilience as they successfully maintained access to ART for ALWH despite the challenges imposed by the pandemic. However, the pandemic and associated measures had a significant effect on HIV VL monitoring across all 3 countries and did not return to prepandemic levels 1 year after the beginning of pandemic. It is critical to closely monitor the HIV care continuum in the postpandemic era to ensure that the documented disruptions in services do not have enduring effects on ALWH's virological and clinical outcomes.
Patient and Public InvolvementPatients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
ACKNOWLEDGMENTSThe IeDEA West Africa Collaboration 2021–2026: Site investigators and cohorts: Adult cohorts: Marcel Djimon Zannou; CNHU, Cotonou, Benin; Armel Poda, CHU Souro Sanou, Bobo Dioulasso, Burkina Faso: Oliver Ezechi, National Institute of Medical Research (NIMR), Lagos, Nigeria. Eugene Messou, ACONDA CePReF, Abidjan, Côte d’Ivoire: Henri Chenal; CIRBA, Abidjan, Côte d’Ivoire: Kla Albert Minga; CMSDS, Abidjan, Côte d’Ivoire: Aristophane Tanon; CHU Treichville, Côte d’Ivoire: Moussa Seydi; CHU de Fann, Dakar, Senegal: Ephrem Mensah, Clinique EVT, Lomé, Togo. Pediatric cohorts: Caroline Yonaba, CHU Yalgado Ouadraogo, Ouagadougou, Burkina Faso: Lehila Bagnan Tossa, CNHU, Cotonou, Benin: Jocelyn Dame, Korle Bu Hospital, Accra, Ghana: Sylvie Marie N’Gbeche; ACONDA CePReF, Abidjan, Côte d’Ivoire: Kouadio Kouakou; CIRBA, Abidjan, Côte d’Ivoire: Madeleine Amorissani Folquet; CHU de Cocody, Abidjan, Côte d’Ivoire: François Tanoh Eboua, CHU de Yopougon, Abidjan, Côte d’Ivoire: Fatoumata Dicko Traore, Hopital Gabriel Toure, Bamako, Mali: Agatha David, NIMR, Lagos, Nigeria: Elom Takassi, CHU Sylvanus Olympio, Lomé,Togo. Coordination and data centers: Antoine Jaquet (PI), Didier Koumavi Ekouevi (PI), François Dabis, Renaud Becquet, Charlotte Bernard, Karen Malateste, Olivier Marcy, Marie Kerbie Plaisy, Elodie Rabourdin, Thierry Tiendrebeogo, ADERA, ISPED & INSERM U1219/IRD, Bordeaux, France. Désiré Dahourou, Sophie Desmonde, Julie Jesson, Valeriane Leroy, Inserm U1295, Toulouse, France: Raoul Moh, Jean-Claude Azani, Jean Jacques Koffi, Eric Komena, Maika Bengali, Abdoulaye Cissé, Guy Gnepa, Apollinaire Horo, Simon Boni, Eulalie Kangah, Corinne Moh, Jeanne Eliam, PACCI, CHU Treichville, Abidjan, Côte d’Ivoire Partner institutions Ighovwerha Ofotokun (PI), Chris Martin, Emory University: Noelle Benzekri, Geoffrey Goettlieb; Washington University; Olivia Keiser, Geneva University. Executive committee: Antoine Jaquet, Didier Ekouevi, Ighovwerha Ofotokun, François Dabis, Valériane Leroy Steering committee: Renaud Becquet, Noelle Benzekri, Charlotte Bernard, Simon Boni, François Dabis, Désiré Dahourou, Sophie Desmonde, Didier Koumavi Ekouevi, Antoine Jaquet, Julie Jesson, Eric Komena, Valeriane Leroy, Karen Malateste, Ighovwerha Ofotokun, Marie Kerbie Plaisy, Elodie Rabourdin, Thierry Tiendrebeogo. Epicentre: Mathidle Mousset, Epicentre Médecins Sans Frontières, Paris, France.
REFERENCES 1. The Global Fund. The Impact of Covid-19 on HIV, TB and Malaria Services and Systems for Health: A Snapshot from 502 Health Facilities. Glob Fund to Fight AIDS Malaria, Tuberc [Internet]; 2021. Available at: https://reliefweb.int/sites/reliefweb.int/files/resources/covid-19_2020-disruption-impact_report_en.pdf. Accessed November, 2022. 2. ECOWAS; WFP; ECA. Monitoring Report on the Impacts of COVID-19 in West Africa. ECOWAS; 2021. 3. Amimo F, Lambert B, Magit A. What does the COVID-19 pandemic mean for HIV, tuberculosis, and malaria control? Trop Med Health. 2020;48:32. 4. UNAIDS. Global HIV Statistics [Internet]; 2022. Available at: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf. Accessed May, 2023. 5. Jewell BL, Mudimu E, Stover J, et al. Potential effects of disruption to HIV programmes in sub-Saharan Africa caused by COVID-19: results from multiple mathematical models. Lancet HIV. 2020;7:e629–e640. 6. Hogan AB, Jewell BL, Sherrard-Smith E, et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: a modelling study. Lancet Glob Health. 2020;8:e1132–e1141. 7. Global Fund. The Global Fund 20 Years of Impact: Results Report 2021; 2021:98. Available at: https://www.theglobalfund.org/media/11304/corporate_2021resultsreport_report_en.pdf. Accessed May, 2023. 8. UNAIDS 2022. UNAIDS [Internet]; 2022:1–446. Available at: https://www.unaids.org/en/resources/documents/2023/2022_unaids_data. Accessed May, 2023. 9. Global HIV Prevention Coalition. Preventing HIV infections at the time of a new pandemic. UNAIDS; 2020:1–54. 10. Brazier E, Ajeh R, Maruri F, et al. Service delivery challenges in HIV care during the first year of the COVID-19 pandemic: results from a site assessment survey across the global IeDEA consortium. J Int AIDS Soc. 2022;25:e26036. 11. UNAIDS. Press release. New Survey Results Indicate that Nigeria Has an HIV Prevalence of 1.4%; 2019. Available at: https://www.unaids.org/en/resources/presscentre/pressreleaseandstatementarchive/2019/march/20190314_nigeria. 13. WHO. A Global Database of Public Health and Social Measures Applied During the COVID-19 Pandemic [Internet]. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/phsm. Accessed May, 2023. 14. WHO. WHO Public Health and Social Measures [Internet]. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/phsm. Accessed May, 2023. 15. Calonico S, Cattaneo MD, Farrell MH, et al. Rdrobust: software for regression-discontinuity designs. Stata J. 2017;17:372–404. 16. Calonico S, Cattaneo MD, Titiunik R. Robust data-driven inference in the regression-discontinuity design. Stata J. 2014;14:909–946. 17. Jardim CGR, Zamani R, Akrami M. Evaluating the impact of the COVID-19 pandemic on accessing HIV services in South Africa: a systematic review. Int J Environ Res Public Health. 2022;19:11899. 18. Lagat H, Sharma M, Kariithi E, et al. Impact of the COVID-19 pandemic on HIV testing and assisted partner notification services, Western Kenya. AIDS Behav. 2020;24:3010–3013. 19. Boyd AT, Jahun I, Dirlikov E, et al. Expanding access to HIV services during the COVID-19 pandemic—Nigeria, 2020. AIDS Res Ther. 2021;18:62–68. 20. Folayan MO, Arije O, Enemo A, et al. Factors associated with poor access to HIV and sexual and reproductive health services in Nigeria for women and girls living with HIV during the COVID-19 pandemic. Afr J AIDS Res AJAR. 2022;21:171–182. 21. Olakunde BO, Adeyinka DA, Olawepo JO, et al. HIV testing among men in Nigeria: a comparative analysis between young people and adults. AIDS Care. 2020;32:155–162. 22. Bekker LG, Alleyne G, Baral S, et al. Advancing global health and strengthening the HIV response in the era of the Sustainable Development Goals: the International AIDS Society-Lancet Commission. Lancet. 2018;392:312–358. 23. WHO. The Use of Antiretroviral Drugs for Treating and Preventing HIV Infection. World Health Organization; 2016. 24. Pham MD, Nguyen HV, Anderson D, et al. Viral load monitoring for people living with HIV in the era of test and treat: progress made and challenges ahead—a systematic review. BMC Public Health. 2022;22:1203. 25. WHO. Consolidated Guidelines on HIV Prevention, Diagnosis, Treatment and Care for Key Populations; 2016. Available at: https://iris.who.int/bitstream/handle/10665/246200/9789241511124-eng.pdf. 26. SeyedAlinaghi S, Mirzapour P, Pashaei Z, et al. The impacts of COVID-19 pandemic on service delivery and treatment outcomes in people living with HIV: a systematic review. AIDS Res Ther. 2023;20:4. 27. Kalua T, Egger M, Jahn A, et al. HIV suppression was maintained during the COVID-19 pandemic in Malawi: a program-level cohort study. J Clin Epidemiol. 2022;150:116–125.
留言 (0)