
記住我
Emergency departments (EDs) provide care to underserved patients at higher risk for HIV acquisition, and for many of these patients, the ED serves as their sole contact with the healthcare system.1 ED HIV screening programs have primarily focused on the identification of newly diagnosed individuals, while result disclosure, prevention counseling, and delivery of prevention services for patients screening HIV negative have not been prioritized.2–4
Studies have demonstrated that HIV preexposure prophylaxis (PrEP) is safe, well-tolerated, and efficacious among populations at higher risk of acquiring HIV.5–7 According to the US Public Health Service Task Force, there are an estimated 1.2 million US adults with indications for PrEP.8 Although PrEP uptake has increased over time, overall prescribing rates remain low and modeling data suggests that expanding the number of persons taking PrEP could have a major impact on US HIV incidence.9,10 EDs, in the context of HIV screening programs, may have an important role in ending the HIV epidemic through routine PrEP assessment and referral of negative patients at higher risk for acquiring HIV infection.
In 2021, the Alameda Health System (AHS) expanded its ED HIV screening program to include the HIV PreventED Program to increase access to HIV prevention services, including PrEP. The HIV PreventED Program utilized an HIV prevention navigator to identify patients who tested HIV negative but are at higher risk of acquiring HIV, perform patient-tailored risk prevention education, and provide outpatient referrals to a network of community HIV prevention specialists.
Study HypothesisWe hypothesized that ED patients who were identified as being at higher risk for acquiring HIV infection would be willing to participate in navigator-facilitated HIV prevention services and that the uptake of outpatient referrals, including PrEP initiation, would be high.
METHODS Study DesignThis was a cross-sectional study using data collected from navigator-administered questionnaires, medical record reviews, and a clinical database of patient information maintained by the HIV PreventED program navigator. The Institutional Review Board at the AHS approved this study. We report the first 9 months of the program, April 1, 2022–December 31, 2022.
HIV PreventED Program FundingImplementation of the HIV PreventED program was supported by a Gilead Sciences FOCUS grant and administered by 1 clinical operations lead (D.A.E.W.), 1 full-time ED HIV prevention navigator (C.M.P.), and 1 full-time ED HIV screening project coordinator (M.J.). The FOCUS program is a public health initiative that supports HIV, hepatitis C virus, and hepatitis B virus (HBV) screening, prevention, and linkage to a first appointment.11 FOCUS funding does not support activities beyond linkage to a first appointment.
HIV PreventED Program Policy and ProceduresThe HIV PreventED policy and procedures were developed by the clinical operations lead and informed by consultation with physicians with experience providing comprehensive HIV prevention services and recommendations published by the East Bay Getting to Zero collaborative.12 The prevention navigator, a recent college graduate without healthcare experience who was bilingual in English and Spanish, worked Monday through Friday, 9 am–5 pm. The navigator was trained by the clinical operations lead and the program coordinator in motivational interviewing techniques, survey administration, and basic HIV prevention assessments and interventions.12,13 The navigator completed the online HIV PrEP Navigator certification program.14
SettingThis project took place at the AHS, Highland Hospital ED, a level 1 trauma center with an annual patient census of 57,000 visits and an Accreditation Council for Graduate Medical Education-Affiliated ED residency program. Opt-out HIV screening is integrated into standard processes for eligible adult patients aged 18–65 years undergoing laboratory testing using an automated electronic health record (EHR) algorithm (Epic Systems Corporation).
SubjectsAll ED patients testing HIV negative were eligible to be assessed by the ED HIV prevention navigator if they were ≥18 and ≤55 years old and not acutely ill or confused. Patients who were currently incarcerated, with language barriers, COVID-19 positive, or evaluated for sexual assault were excluded from navigator assessments. We excluded patients >55 years old from HIV prevention navigator assessments based on a 1-month pilot program that demonstrated our navigator could not complete HIV prevention assessments for all ED patients who tested HIV negative coupled with the findings that this age cohort seemed generally less interested in participating in HIV prevention assessments and was almost always identified to be at lower risk for acquiring HIV.
Subject RecruitmentThe ED HIV prevention navigator first identified patients screening HIV negative through real-time EHR review of all current patients in the ED as well as through an automated process that routed HIV test results to their EPIC in the basket. The navigator then performed a chart review to identify patients who might be eligible for a risk assessment (excluding those who were critically ill, confused/altered, COVID positive, incarcerated, evaluated for sexual assault, or with language barriers), and then the navigator attempted to contact all potentially eligible patients either in the ED or through phone to participate in the HIV risk assessment and the ED HIV prevention counseling session. After contact with the patient, additional consent for the research study was obtained to collect risk assessment data and tracking of programmatic outcomes. Participation in this study was not a requirement to receive HIV prevention services and had no impact on the services provided.
ProceduresAfter consent to participate, the HIV prevention navigator administered a survey using questions adapted from the Centers for Disease Control and Prevention (CDC) 2017 PrEP clinical practice guidelines to help assess the patient's risk of acquiring HIV infection.15 The results of HB this survey were used by the navigator to guide the need for, and scope of, HIV education and prevention services. All patients, regardless of risk for acquiring HIV, received basic HIV prevention education, which included information on HIV transmission, HIV testing, and postexposure prophylaxis (PEP) and PrEP treatment. Patients seen in the ED also received this information in the form of a printed informational handout.
Patients who were identified as being at higher risk for acquiring HIV were notified of this and underwent more comprehensive risk reduction counseling and education (tailored to individual patient needs), which included detailed information on PrEP, safer injection practices, and substance use treatment needs. These patients were then offered to be referred to outpatient HIV prevention services, where PrEP could be provided. The ED prevention navigator actively referred patients interested in outpatient prevention services within a network of local federally qualified health centers (FQHC) identified from the East Bay Getting to Zero collaborative.16 The ED prevention navigator assisted interested patients at higher risk for acquiring HIV by arranging outpatient linkage to HIV prevention services, working directly with navigators at partnering FQHCs. Navigators tracked the outcomes of these referrals through a combination of EHR review and telephone follow-up with patients and the outpatient clinics.
Survey ContentA standardized data collection instrument was used. The data collection instrument collected information on demographic characteristics (age, sex, and race/ethnicity), past medical history, HIV testing history, HIV risk behavior, sexually transmitted infection (STI) history, substance use history, categorization as higher or lower risk for HIV acquisition, and willingness to be referred to outpatient HIV prevention services, if applicable. The risk survey has been previously described and included questions adapted from the 2017 CDC guidelines for PrEP, as well as 2 site-specific risk factors, sex while using stimulants in the past 6 months and requesting PrEP after meeting with the prevention navigator in the absence of other reported risk behaviors.15,17 Patients reporting ≥1 risk behavior elicited in the survey were categorized at higher risk for acquiring HIV, all others were categorized at lower risk for acquiring HIV (see Table, Supplemental Digital Content, https://links.lww.com/QAI/C264).
Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at the AHS.18,19
Data Analysis Outcome MeasuresThe primary outcome measure was the number and proportion of ED patients at higher risk for HIV acquisition that followed up for outpatient HIV prevention services. The secondary outcome measure was the number and proportion of ED patients at higher risk for HIV acquisition who received PrEP. Characteristics of patients are reported at major stages of the ED HIV prevention care continuum (defined below).
DefinitionsOutpatient prevention services were defined as clinics that provide a range of prevention services, including HIV education, risk reduction counseling, instruction on proper condom use, undetectable = untransmissible messaging, PEP/PrEP education and treatment, substance use counseling and referral, and information on safe injection practices, with the capacity to follow patients longitudinally.
Patients were identified as at higher risk for HIV acquisition if they reported one or more risk factors or, if in the absence of reported risk, they requested PrEP upon completion of the navigator assessment (see Table, Supplemental Digital Content, https://links.lww.com/QAI/C264).
Acceptance of referral to outpatient HIV prevention services was defined as an ED patient at higher risk for HIV acquisition agreeing to have the prevention navigator facilitate appointment scheduling with a clinic that provides outpatient prevention services, including PrEP.
Referred to outpatient HIV prevention services was defined as any attempt by the ED prevention navigator to contact a clinic on behalf of the ED patient to facilitate appointment scheduling for outpatient prevention services, including PrEP.
Receipt of outpatient HIV prevention services was defined as the ED patient attending an outpatient clinic appointment for prevention services.
Receipt of PrEP was defined as the ED patient receiving a prescription for PrEP at the outpatient clinic.
Time to linkage was measured from the date the referral was made to the date the patient attended their first outpatient HIV prevention services appointment.
Patients were classified as not receiving outpatient HIV prevention services if their attendance could not be confirmed through EHR review or after phone follow-up with the ED navigator. Patients were classified as not receiving PrEP if it could not be confirmed through EHR review or after phone follow-up with the ED navigator that PrEP was prescribed.
Statistical MethodsAll statistical analyses were performed using Stata (Version 14, Stata Corporation, College Station, TX). For continuous data that are normally distributed, means with SDs were reported. For continuous data that are not normally distributed or ordinal data, medians with interquartile ranges were reported.
RESULTSThe figure shows the outcomes at each step of the ED HIV prevention care cascade. During the 9-month study period, 19,614 unique patients aged 18–55 years received ED care and 5592 tested HIV negative. There were an additional 1247 unique patients aged >55 years who tested HIV negative but who were ineligible to receive HIV prevention navigator assessments based on age. Of the 5592 potentially age-eligible patients, 1233 consented to participate in this study and were assessed by the ED prevention navigator. The main reasons why age-eligible patients who tested HIV negative were not enrolled in this study were as follows: patient unavailable (37%), patient declined assessment (25%), language barrier (15%), and medical acuity/confusion (13%).
Of the 1233 patients completing assessments, 1040 (84.3%) were identified to be at lower risk for HIV acquisition and received basic HIV prevention education while 193 (15.7%) were identified to be at higher risk for HIV acquisition and received individualized HIV prevention counseling and offered referral for outpatient prevention services. Of these 193 patients at higher risk for HIV acquisition, 104 (53.9%) accepted and were referred for outpatient prevention services, 23 (11.9%) attended an outpatient appointment, and 13 (6.7%) received PrEP. The reasons why PrEP was not prescribed were as follows: the outpatient clinician felt that the patient was not at ongoing risk for acquiring HIV (N = 4), the patient declined a PrEP prescription (N = 3), and unknown (N = 3). Twelve of the 23 patients (52.2%) attending an outpatient appointment were linked within 1 month of their referral, with a median time to linkage of 28 days (interquartile range 15–41 days).
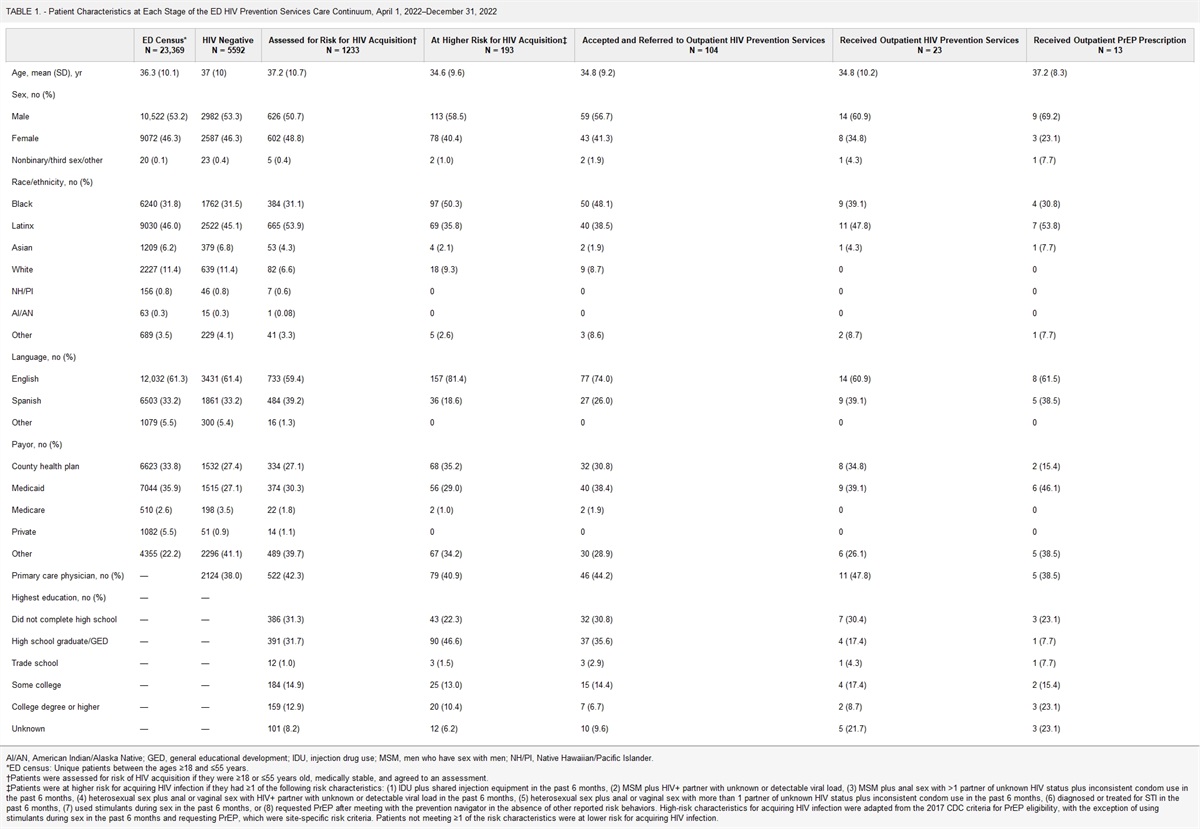
Table 1 shows the characteristics of patients at each step of the ED HIV prevention care continuum. Patients at higher risk for HIV acquisition had a mean age of 34.6 years, 58.5% were men, 50.3% were Black, 35.8% were LatinX, 40.9% had a primary care physician, and 30.8% did not complete high school.
TABLE 1. - Patient Characteristics at Each Stage of the ED HIV Prevention Services Care Continuum, April 1, 2022–December 31, 2022 ED Census*AI/AN, American Indian/Alaska Native; GED, general educational development; IDU, injection drug use; MSM, men who have sex with men; NH/PI, Native Hawaiian/Pacific Islander.
*ED census: Unique patients between the ages ≥18 and ≤55 years.
†Patients were assessed for risk of HIV acquisition if they were ≥18 or ≤55 years old, medically stable, and agreed to an assessment.
‡Patients were at higher risk for acquiring HIV infection if they had ≥1 of the following risk characteristics: (1) IDU plus shared injection equipment in the past 6 months, (2) MSM plus HIV+ partner with unknown or detectable viral load, (3) MSM plus anal sex with >1 partner of unknown HIV status plus inconsistent condom use in the past 6 months, (4) heterosexual sex plus anal or vaginal sex with HIV+ partner with unknown or detectable viral load in the past 6 months, (5) heterosexual sex plus anal or vaginal sex with more than 1 partner of unknown HIV status plus inconsistent condom use in the past 6 months, (6) diagnosed or treated for STI in the past 6 months, (7) used stimulants during sex in the past 6 months, or (8) requested PrEP after meeting with the prevention navigator in the absence of other reported risk behaviors. High-risk characteristics for acquiring HIV infection were adapted from the 2017 CDC criteria for PrEP eligibility, with the exception of using stimulants during sex in the past 6 months and requesting PrEP, which were site-specific risk criteria. Patients not meeting ≥1 of the risk characteristics were at lower risk for acquiring HIV infection.
Table 2 shows the outcomes at select stages of the ED HIV prevention care continuum, stratified by whether the navigator assessment occurred over the phone (after the patient was discharged) or in person (during the ED visit). Of the 1166 assessments performed by the ED prevention navigator for which the location of assessment was known, 763 (65.4%) were completed over the phone and 403 (34.6%) were performed in person. Care continuum outcomes were similar between groups with the exception of receipt of PrEP among those attending an outpatient prevention services appointment. PrEP was prescribed to 6/16 (37.5%) ED patients who followed up after a phone assessment compared with 7/7 (100%) who followed up after an in-person assessment, P = 0.005.
TABLE 2. - Outcomes at Select Stages of the ED HIV Prevention Services Care Continuum, Stratified by Whether the Prevention Navigator Assessment Was Performed Through Phone or in Person Total Assessments*IDU, injection drug use; MSM, men who have sex with men.
*Patients were assessed by the ED prevention navigator to determine whether they were at higher risk for acquiring HIV if they screened HIV negative, were ≥18 or ≤55 years old, and medically stable. Assessments occurred either by phone after ED discharge or in person during the ED visit. Data on assessment type were missing for 67 patients.
†Patients were at higher risk for acquiring HIV infection if they had ≥1 of the following risk characteristics: (1) IDU plus shared injection equipment in the past 6 months, (2) MSM plus HIV+ partner with unknown or detectable viral load, (3) MSM plus anal sex with >1 partner of unknown HIV status plus inconsistent condom use in the past 6 months, (4) heterosexual sex plus anal or vaginal sex with HIV+ partner with unknown or detectable viral load in the past 6 months, (5) heterosexual sex plus anal or vaginal sex with more than 1 partner of unknown HIV status plus inconsistent condom use in the past 6 months, (6) diagnosed or treated for STI in the past 6 months, (7) used stimulants during sex in the past 6 months, or (8) requested PrEP after meeting with the prevention navigator in the absence of other reported risk behaviors. High-risk characteristics for acquiring HIV infection were adapted from the 2017 CDC criteria for PrEP eligibility, with the exception of using stimulants during sex in the past 6 months and requesting PrEP, which were site-specific risk criteria. Patients not meeting ≥1 of the risk characteristics were at lower risk for acquiring HIV infection.
‡Proportion of patients at higher risk for HIV acquisition.
§Proportion of patients that accepted and referred to outpatient HIV prevention services.
||Proportion of patients that received outpatient HIV prevention services.
Table 3 shows the outcomes of the risk factor assessments, stratified by whether patients were identified to be at higher or lower risk for acquiring HIV infection. The most common reasons 193 patients were classified at higher risk were as follows: being recently diagnosed or treated for an STI (N = 89, 46%), using stimulants during sex in the past 6 months (N = 69, 36%), or requesting PrEP after meeting with the navigator, in the absence of other reported risk behaviors (N = 27, 14%). The 1040 patients identified at lower risk reported very few behaviors within our risk categories, with only 5 (0.5%) using injection drugs in the past 6 months and/or 28 (2.7%) identifying as men who have sex with men.
TABLE 3. - Characteristics of 1233 Emergency Department Patients Screening HIV Negative, Stratified by Risk for Acquiring HIV Infection At Higher Risk for HIV Acquisition*IDU, injection drug use; MSM, men who have sex with men.
*Patients were at higher risk for acquiring HIV infection if they had ≥1 of the following risk characteristics: (1) IDU plus shared injection equipment in the past 6 months, (2) MSM plus HIV+ partner with unknown or detectable viral load, (3) MSM plus anal sex with >1 partner of unknown HIV status plus inconsistent condom use in the past 6 months, (4) heterosexual sex plus anal or vaginal sex with HIV+ partner with unknown or detectable viral load in the past 6 months, (5) heterosexual sex plus anal or vaginal sex with more than 1 partner of unknown HIV status plus inconsistent condom use in the past 6 months, (6) diagnosed or treated for STI in the past 6 months, (7) used stimulants during sex in the past 6 months, or (8) requested PrEP after meeting with the prevention navigator in the absence of other reported risk behaviors. High-risk characteristics were adapted from the 2017 CDC criteria for PrEP eligibility, with the exception of using stimulants during sex in the past 6 months and requesting PrEP, which were site-specific risk criteria. Patients not meeting ≥1 of the risk characteristics were at lower risk for acquiring HIV infection.
†Characteristic used to identify a patient at higher risk for acquiring HIV infection.
Of the 193 patients at higher risk for HIV acquisition, 2 had indications for PEP and none had signs or symptoms consistent with acute HIV. Most patients (N = 131, 67.9%) completed HIV screening along with other blood testing while 62 (32.1%) had HIV screening tests performed as part of an STI evaluation and did not undergo other blood work. When blood testing was performed, it included an assessment of renal function 100% of the time and HBV serologies 56% (N = 73) of the time. When performed, nearly all renal function tests (130/131, 99.2%) were normal (estimated glomerular filtration rate >60 mL/min). None of the HBV surface antigen tests were reactive. Sixty-nine (35.8%) of the 193 patients at higher risk for HIV acquisition were women of reproductive age and pregnancy testing was completed in 55 (79.7%) of them, of which 8 (14.5%) were positive.
DISCUSSIONWe describe a model for integrating HIV prevention services into an ED with an existing HIV screening program that relied on 1 full-time ED HIV prevention navigator who administered risk surveys to eligible adult patients testing HIV negative, to identify a patient cohort at higher risk for acquiring HIV infection. This cohort was then targeted to receive ED-based HIV prevention services, including outpatient referrals for more comprehensive treatment, including PrEP.
Despite drop-offs at each stage of the ED HIV prevention care continuum, we show that this model was (1) acceptable: 54% of the 193 patients at higher risk for acquiring HIV accepted an outpatient referral; (2) feasible: leveraging a pool of 5592 ED patients who screened HIV negative, 1 navigator assessed HIV risk and provided HIV prevention education and information to 1233 (22%) of them; and (3) effective: over 1000 ED patients testing HIV negative and at lower risk for acquiring HIV received basic HIV counseling and prevention information and 193 patients at higher risk received comprehensive ED HIV prevention counseling, of which 23 (11.9%) participated in outpatient prevention services and 13 (6.7%) were prescribed PrEP. With this strategy, the number of ED patients testing HIV negative who needed to be screened by the prevention navigator to get 1 person on PrEP was 95. The cost-effectiveness studies are now needed to know whether this level of linkage and PrEP initiation justifies the costs.
Nearly 2/3 of the prevention assessments occurred over the phone rather than in person. Care continuum outcomes were generally similar regardless of the location of the assessment; however, a proportionately greater number of in-person assessments resulted in the receipt of an outpatient PrEP prescription compared with phone assessments. The reasons for this difference are not known but may be attributed to the better identification and counseling of PrEP-eligible patients with in-person assessments. Understanding the reasons for these differences is important in guiding whether future protocols should emphasize in-person over telehealth navigation procedures.
Assessment of an individual's risk for acquiring HIV, beyond simply screening HIV negative, is a critical step in any ED prevention program.17,20–24 We chose to determine eligibility for comprehensive prevention services and PrEP referral using a structured risk assessment administered by an ED navigator. With this strategy, 16% of ED patients completing routine HIV screening were identified as being at increased risk of acquiring HIV, a number consistent with prior studies using similar screening strategies.17 Although feasible, this approach was relatively inefficient. Over 9 months, the ED prevention navigator reviewed the charts of nearly 6000 ED patients who were HIV negative, attempted callbacks or in-person assessments 3553 times, and completed 1233 surveys, to identify 193 patients who are at high risk for HIV acquisition. Furthermore, the ED patients we identified as being at high risk for HIV acquisition most often reported being diagnosed or treated for an STI (46%), using stimulants during sex in the past 6 months (36%), or requested PrEP treatment in the absence of reported risk (14%).
Our reliance on categorizing a patient's risk for acquiring HIV based on the answers to structured surveys adapted from CDC criteria may also miss patients at higher risk for HIV acquisition due to response bias, which may limit the utility of this approach. In fact, our navigator reported that patients were often reluctant to disclose stigmatizing risks, and we often observed survey responses that were inconsistent with risk behaviors documented in the medical record (data not shown). Replacing traditional risk assessments with open-ended questions that emphasize an individual's sexual health goals and concerns may provide more accurate information about a patient's true behavior, risk, and readiness for PrEP.25 Alternatively, having patients self-administer questionnaires through waiting room kiosks or tablets may minimize stigma and bias in determining risk, compared with in-person or phone-based assessments.
Novel methods to identify ED patients who might benefit from HIV prevention services may be more efficient and less stigmatizing than our model.22,26,27 These include automating the EHR to identify patients who may be at increased risk for acquiring HIV infection.
留言 (0)