To our knowledge, this study is the first to associate detailed information about the early luteal phase levels of progesterone and 17-hydroxyprogesterone with live birth in infertile women with normal ovarian reserve undergoing IVF with fresh embryo transfer. The live birth rate in those who had an upper profile of serum progesterone and serum 17-hydroxyprogesterone based on the AUC of measurements from the time of hCG trigger until implantation was three times higher than that in women with a lower serum profile of both hormones.
We believe that the analysis of the association between values that make up the overall luteal phase hormone profiles and the live birth rate is more meaningful than associations between the hormone level at each time point and the live birth rate because one woman may have hormone levels that reflect a lower profile at one timepoint and an upper profile at another timepoint whereas the overall total luteal phase hormonal profile for each woman provides better information about hormonal level exposure and therefore better information to evaluate for correlation with the live birth rate. Next, we identified factors that were associated with a lower hormone profile across the total luteal phase found that AMH, number of oocytes, day-3 embryos and good day-3 embryos were predictors for a lower profile of serum progesterone (Table 2), and the number of follicles of ≥ 14 mm and the number of good day-3 embryos were associated with a lower profile of 17-hydroxyprogesterone (Table 3).
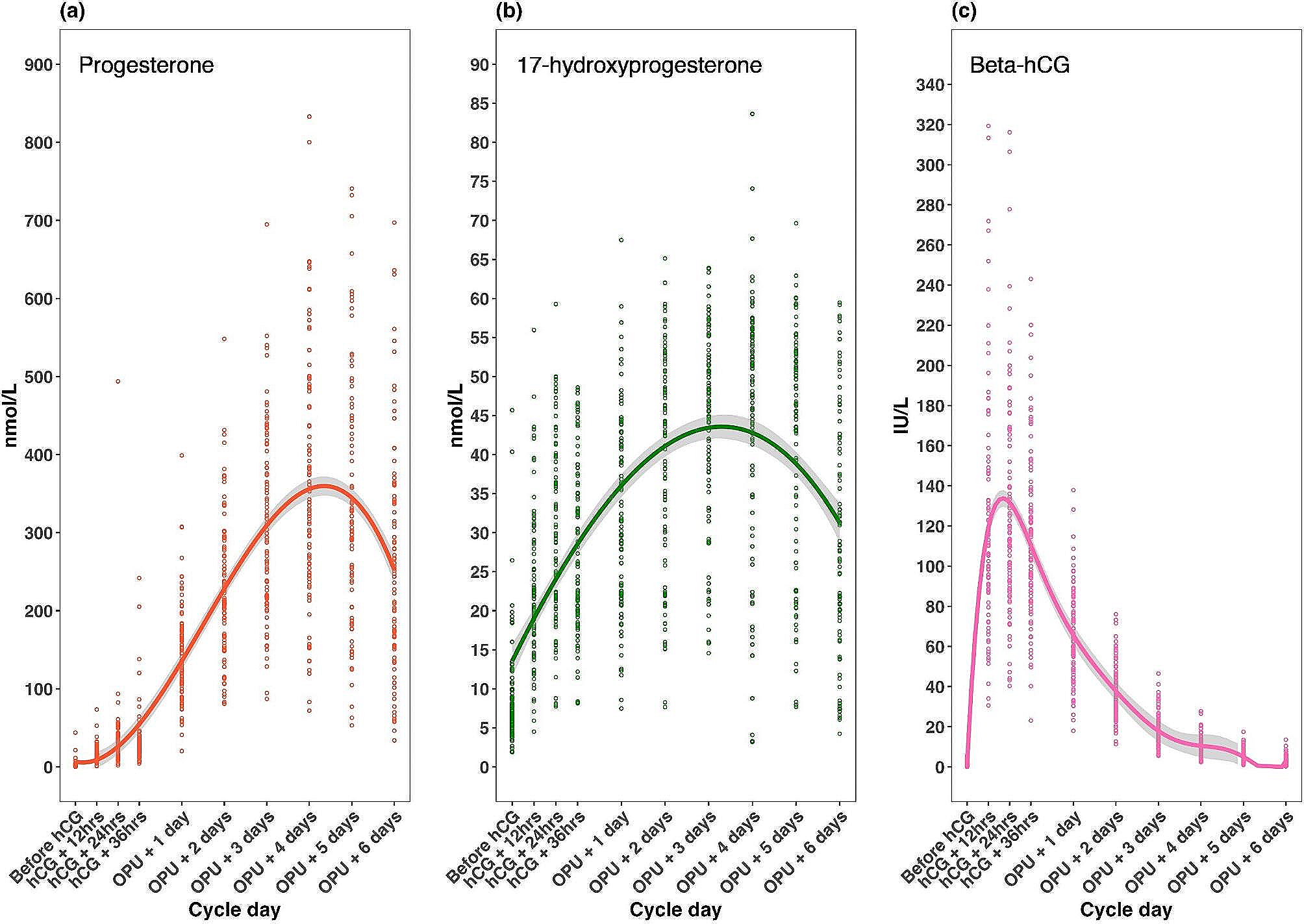
Unlike protocols for ovarian stimulation during the follicular phase (which have undergone several refinements over the last 20–30 years), there is not currently any individualization of exogenous luteal phase support after use of a bolus hCG trigger during IVF. One contributing factor may be a relative lack of information about the relationship between early luteal phase hormone levels and fertility outcomes. Our group previously evaluated the early luteal phase hormonal profile after hCG trigger [4], and found a comparable serum progesterone trajectory to that in the current study, with considerable variability in the timing of peak progesterone between individuals. Our previous data also showed marked inter-individual variation in hCG concentrations after hCG trigger [4]. However, that study was conducted in the setting of frozen embryo transfer so the influence of early phase luteal hormone levels on fertility outcomes could not be determined.
The underlying mechanism for the marked difference in pregnancy rates between the lower and upper profile groups was not determined in the current study. Both groups were similar with respect to several participant characteristics but differed significantly in the number of follicles and oocytes collected, with the upper group having significantly higher numbers. Previous studies have shown that an increase in the number of oocytes aspirated during IVF treatment is associated with improved chances of pregnancy until a plateau is reached [7]. Having more oocytes/embryos available to select from in terms of embryo transfer clearly is beneficial, but it is not clear whether, for instance, a blastocyst with equal developmental competence and morphology score (potentially also tested for normal chromosomal status) has a better chance of implantation when it comes from a larger versus smaller cohort of embryos. The current study suggests that endometrial receptivity in the subgroup with an upper serum progesterone profile may be positively affected by the higher progesterone concentration provided by a higher number of corpora lutea compared with the lower serum progesterone profile group. It is likely that the endometrium cannot distinguish between progesterone produced from a few follicles versus many follicles, but the between-group difference in numbers of follicles and oocytes collected could reflect other factors that may influence the outcome of IVF such as advanced age.
Almost one in five women in this study had a very poor luteal phase despite the administration of 6500 IU hCG, which was characterized by early peak progesterone and insufficient progesterone secretion. The hCG bolus trigger provides a strong luteotropic stimulus and concentrations of progesterone rise a lot faster after an hCG bolus trigger than in natural cycles, but the progesterone peak after hCG trigger occurs earlier than in natural cycles. Individuals with a poor luteal phase after hCG trigger are not currently recognized in the clinic and, despite having good-quality embryos, the luteal phase is not sufficient to support pregnancy. It is therefore important to identify and detect these women.
Our data showed that the percentage increase from hCG trigger to oocyte pick-up was greater for 17-hydroxyprogesterone than for progesterone, that early levels were a better predictor of later luteal phase levels for 17-hydroxyprogesterone than for progesterone, and that endogenous production of 17-hydroxyprogesterone peaked about 12 h earlier than progesterone. This means that the endometrium is slightly more advanced than previously thought based on progesterone measurements. Early markers of the subsequent luteal phase need to be determined to allow hormone level profiles to be changed to a trajectory associated with a higher chance of conception in the lower hormone profile group. We found that concentrations of 17-hydroxyprogesterone measured at 24 h after induction of final follicular maturation were a predictor of later luteal phase hormone levels in the lower hormone profile group.
From a clinical perspective, it would be useful to define an early progesterone or 17-hydroxyprogesterone level below which additional luteal phase support could be considered after oocyte pick-up. However, our data do not allow this to be determined, and further research is needed to investigate approaches to altering the post-hCG trigger trajectory of progesterone/17-hydroxyprogesterone levels in a way that enhances the chance of conception. Nevertheless, determination of serum levels of these hormones early after hCG trigger would be required to allow individualization of luteal phase support, and this represents a change from the vast majority of current clinical practice.
Our results were similar for both serum progesterone and serum 17-hydroxyprogesterone, suggesting that endogenous hormone production by the corpus luteum is the important parameter in improving reproductive outcomes. Therefore, to increase pregnancy rates, the aim would be to secure better hormone secretion from the corpus luteum rather than relying on exogenous progesterone supplementation. In addition, the importance of both progesterone and 17-hydroxyprogesterone as predictors of conception in our study could reflect the fact that optimal function of both the luteinized granulosa and theca cells (producing progesterone and 17-hydroxyprogesterone, respectively) would help to improve the chances of achieving pregnancy during IVF. However, it is interesting that women in the lower serum hCG profile group had a slightly, but not significantly higher live birth rate compared with those in the upper hormone profile group. As the lower and upper group of patients show similar BMI and have received a similar bolus of hCG, the difference is likely to reflect either an enhanced clearance or an augmented consumption. However, given that those who conceive show higher levels of progesterone, it is hypothesized that hCG is faster consumed in the good prognosis group due to the higher number of corpora lutea, which collectively will contain more cells and express more LH receptors (LHR) that will bind and internalize hCG. In addition, this may reflect that each cell in the corpora lutea expresses an increased number of LHR, which in culture experiments have shown to result in enhanced progesterone secretion [8]. Furthermore, it is interesting that the 17-OH-P4 is higher in the upper group already from the hCG trigger compared to the lower group, which is not the case for progesterone.
Collectively, these observations further indicate that hormonal interactions between hCG and the corpus luteum are important for achieving pregnancy, and therefore additional studies are needed to determine the reasons for reduced progesterone and 17-hydroxyprogesterone production in those with a lower serum profile of hCG. Women in our study who had a peak progesterone level at four days or later after oocyte pick-up had a live birth rate that was more than twice that in women with an earlier serum progesterone peak. In fact, more than 82% of all live births in the current study occurred in women whose serum progesterone/17-hydroxyprogesterone level peaked on the fourth or fifth day after oocyte pick-up. In addition, those with an early progesterone/17-hydroxyprogesterone peak had higher rates of early pregnancy loss. Half of the pregnancy loss before 12 weeks of gestation occurred in individuals who had peak progesterone level on or before the second day after oocyte pick-up. Based on this study and our previous work [4], women with a peak progesterone on or before the third day after oocyte pick-up comprise about 15–20% of the IVF population. This is not a small proportion, and it is important to identify these individuals early so that luteal phase support can be increased. Given that the best chance for live birth occurred when progesterone peaked on day four after oocyte pick-up, prompt intervention would be required to allow exogenous hormone supplementation that provides peak levels in the optimal time period.
Given the significantly higher live birth rate in individuals in the upper progesterone profile group, an important question is how to ensure that the majority of women fall into this group and therefore have a better chance of achieving pregnancy and live birth. One approach could be to use additional low-dose hCG during the early to mid-luteal phase, potentially rescuing endometrial receptivity. However, some women may not respond with increased progesterone and 17-hydroxyprogesterone output and may require exogenous progesterone. This needs to be evaluated in appropriately designed clinical studies.
A key strength of this study is that it addresses an important knowledge gap regarding associations between early luteal phase hormone levels and fertility outcomes in women undergoing IVF with fresh embryo transfer. The study had a prospective design with respect to collection of early phase luteal hormone levels, but associations between these and the live birth rate represent correlations without providing direct evidence of causality. With respect to serum hormone levels, we cannot exclude the possibility that serum progesterone levels might vary due to inter-individual differences in the absorption of vaginal progesterone provided as luteal phase support, although the influence should be similar in both post hoc defined groups. In addition, our data do not allow us to categorically determine whether the timing of the progesterone peak or the absolute progesterone concentration make the greatest contribution to the chances of achieving pregnancy/live birth; this is an area for future study. Finally, the external generalizability of the study findings is limited by the nature of the study population (all were from Vietnam).


留言 (0)