
記住我




We performed a retrospective, single-center cohort study in the Assisted Reproductive Center of Northwest Women’s and Children’s Hospital, Xi’an, China. The study protocol was approved by the Ethics Committee of Northwest Women’s and Children’s Hospital (No. 2022007).
We studied women treated between January 2017 and December 2020. Women were eligible if they met the following criteria: (1) undergoing a second IVF/ICSI cycle with a failure to achieve pregnancy in the first attempt; (2) no top-quality embryos on day 3 (grade I or II) in the first cycle [11]; and (3) age 20–45 years old. Exclusion criteria were: (1) hyperthyroidism or hypothyroidism; (2) hyperplasia of mammary glands; (3) history of malignant tumor; (4) diabetes mellitus; (5) inclusion in this study in a previous cycle.
Ovarian stimulation protocolsOvarian stimulation could be with GnRH agonist or GnRH antagonist protocols, as has been described in detail elsewhere [12]. Briefly, for the GnRH agonist protocol, pituitary down-regulation began during the mid-luteal phase of the previous menstrual cycle with the GnRH agonist at a dose of 0.1–0.05 mg/day for 14 days. Recombinant follicle-stimulating hormone (rFSH) was started at 150–225 IU/day for ovarian stimulation. The dose of rFSH could be adjusted up to 300 IU/day based on ovarian response. Recombinant luteinizing hormone (rLH) could be added at the discretion of the treating physician.
For the GnRH antagonist protocol, rFSH was started on day 2 of the menstrual cycle, with similar doses of rFSH as the GnRH agonist protocol. GnRH antagonist, 0.25 mg/day was started when the dominant follicle reached 12–14 mm. When two or more follicles reached 17 mm, human chorionic gonadotropin (hCG) was given at a dose of 4,000 to 10,000 IU, and oocyte retrieval was performed 36 h later.
Growth hormone supplementationThe choice to use GH was based on the preference of the woman and her treating physician. Women in the GH group received 2 IU recombinant human GH (Jintropin, Gensci, China) daily, from the initial day of pituitary down-regulation for the GnRH agonist protocol or day 2 of the previous menstrual cycle for the GnRH antagonist protocol until the day of the hCG trigger. Otherwise, treatment of the groups was similar.
Embryo quality assessmentEmbryo quality was assessed on day 3 at 72 h after oocyte retrieval. Embryos were scored according to a combination of blastomere number, blastomere size and fragmentation [13]. Briefly, embryos with 8–10 blastomeres, even homogeneous blastomeres < 10% cytoplasmic fragmentation were classified as grade I - embryos; embryos with 6–7 or > 10 blastomeres with even homogeneous blastomeres of no cytoplasmic fragmentation; or embryos with 8–10 blastomeres with even homogeneous blastomeres of 10%-20% cytoplasmic fragmentation were classified as grade II - embryos; embryos with 4–5 blastomeres with uneven and non-homogeneous blastomeres with 20%-50% cytoplasmic fragmentation were classified as grade III - embryos; embryos with fewer than 4 blastomeres with uneven and non-homogeneous blastomeres with > 50% cytoplasmic fragmentation were classified as grade IV—embryos (Supplementary Table 1). Only embryos classified as grade I, II, and III were available for transfer.
Embryos of grade I and II were regarded as top-quality embryos. For women with more than four top-quality cleavage embryos, all embryos were cultured to the blastocyst stage. A maximum of two embryos were transferred per transfer. The remaining embryos were frozen for future use. Women who were at risk of ovarian hyperstimulation syndrome (OHSS), women who presented with hydrosalpinx, and women who had high progesterone levels on hCG trigger day had frozen-thawed embryo transfer.
Luteal phase support and pregnancy confirmationLuteal support was given with 600 mg of vaginal progesterone and 30 mg oral progesterone daily from the day of oocyte retrieval in the fresh cycle or the day of embryo transfer in the frozen-thawed embryo transfer cycle. A pregnancy tests using serum β-hCG was performed 14 days after embryo transfer. In case of a positive pregnancy test, transvaginal ultrasound was performed 5 weeks after embryo transfer to determine the number of gestational sacs and the fetal heartbeat.
Outcome measuresThe primary outcome was cumulative live birth, defined as a live birth > 24 weeks of gestation, following the use of all fresh and frozen embryos derived from a single ovarian stimulation cycle. Secondary outcomes were biochemical pregnancy, clinical pregnancy, ongoing pregnancy, multiple pregnancy, miscarriage (defined as a pregnancy failure that occurs before 24 completed weeks of pregnancy) and ectopic pregnancy. We also assessed number of embryos, embryo quality and number of embryos available.
For women achieving live birth, we reported birth weight, fetal sex, gestational age at delivery in weeks, preterm birth (defined as delivery before 37 completed weeks of pregnancy) and type of delivery. All women in the study were followed-up until 2 years after oocyte retrieval.
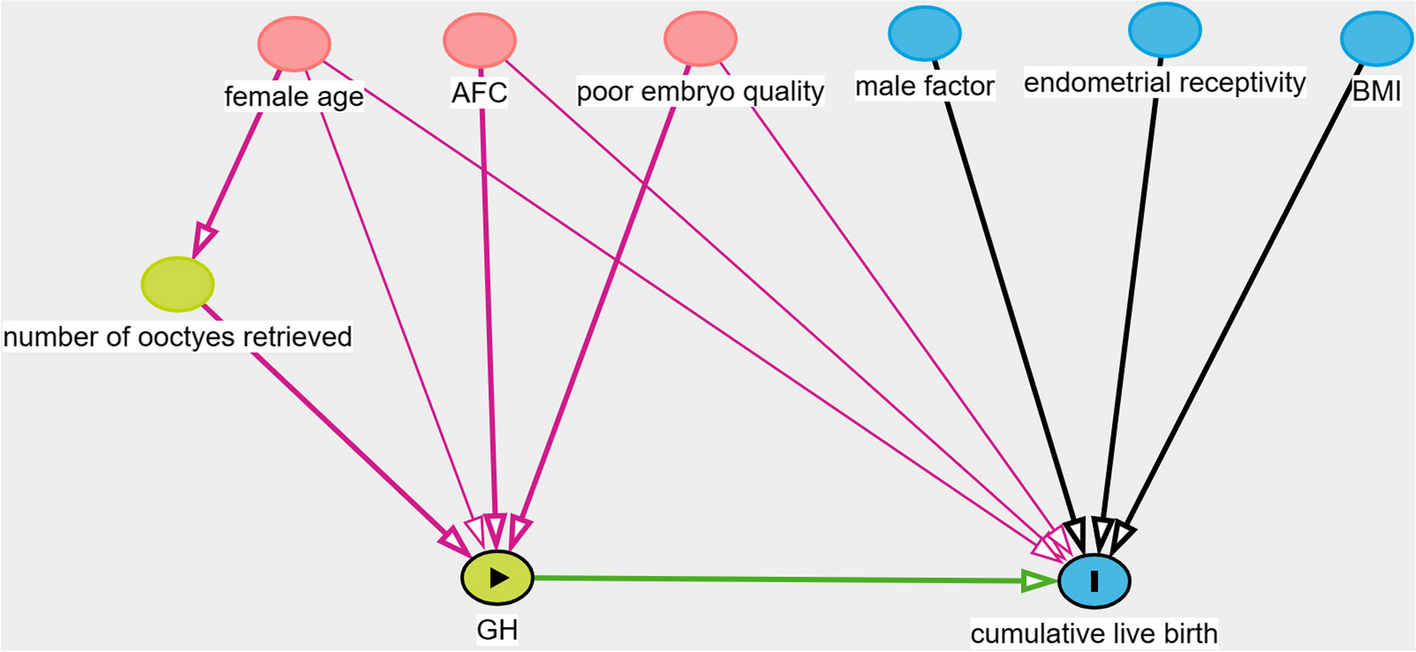
Statistical analysisPropensity score matching (PSM) was performed to match the baseline characteristics of GH and control groups. Confounding was assessed by utilizing prior knowledge with the aid of directed acyclic graphs (DAG) (Fig. 1). The subsequent covariates were contemplated for incorporation in the ultimate model to match the GH group to the control group with a 1:1 ratio: female age, AFC, and embryo quality in previous cycle.
Fig. 1
Directed acyclic graphs in identification selection of covariates
Categorical variables were expressed as percentages and were compared using the chi-square test or Fisher’s exact test. Continuous variables were expressed as mean ± SD and were compared using Student’s t test and the Mann–Whitney U test. Multivariable logistic regression analyses were used to determine the adjusted risk ratios (aRR) and 95% confidence intervals (CIs) for dichotomous outcomes. In the multivariable analyses we adjusted for female age, male age, basal FSH, AFC, body mass index (BMI), infertility duration, and infertility type. Subgroup analysis was performed with quartiles in different female age groups and AFC groups before and after PSM. Subgroup factor (female age and AFC) in the Poisson regression model was used to test the treatment-covariate interaction.
Data were analyzed with the use of the statistical packages R (The R Foundation; http://www.r-project.org.version 3.4.3) and Empower (R) (http://www.empowerstats.net/en/, X&Y solutions, inc. Boston, Massachusetts). A P-value < 0.05 was supposed to indicate statistical significance.
留言 (0)