
記住我


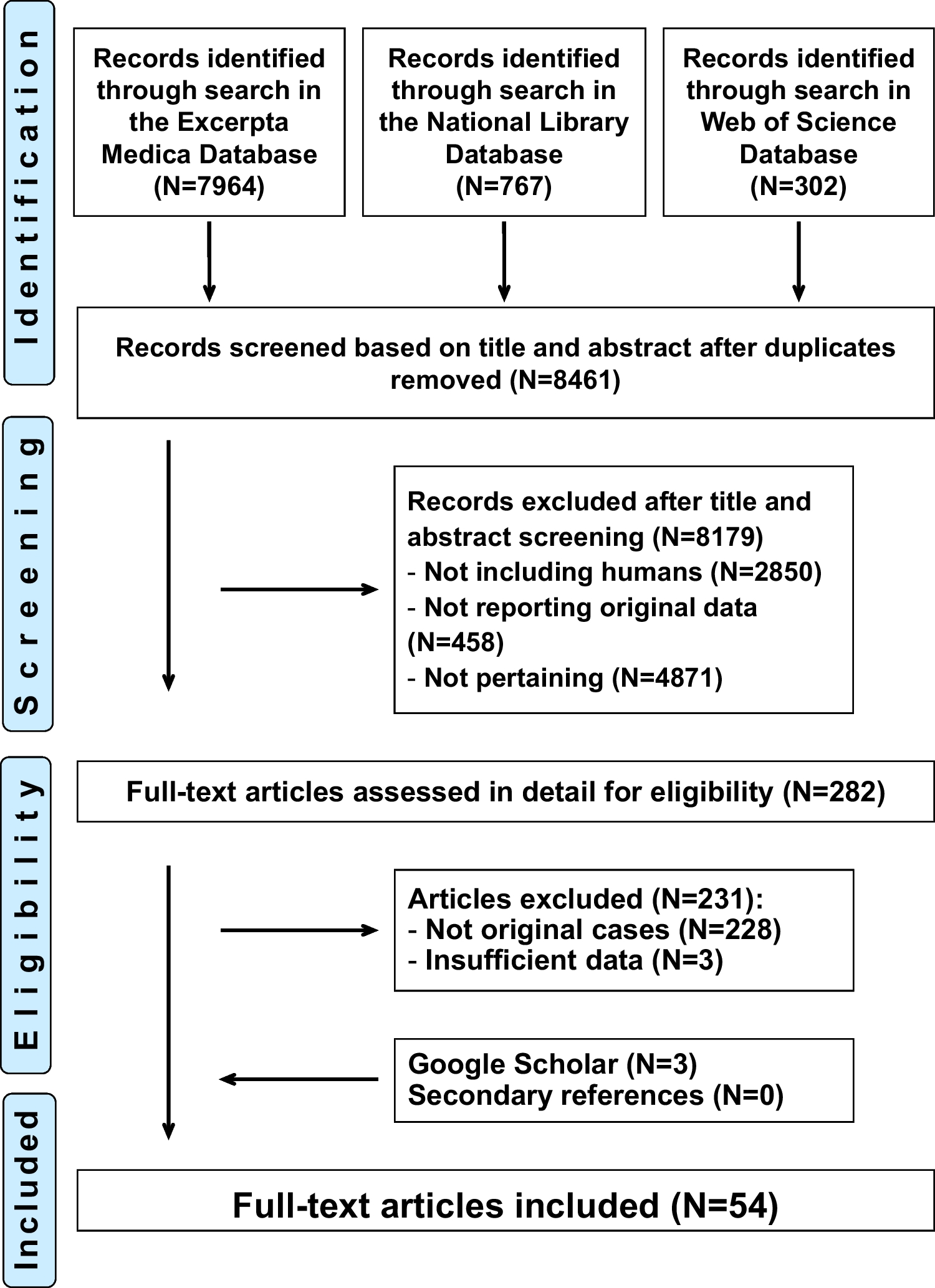
After assessing 2419 records and obtaining the full text for 6 reports, this review found no studies meeting the inclusion criteria (Fig. 1). We excluded five reports because they were cross-sectional prevalence studies with no control groups and one report for being a review (Supplementary material. Annex – Excluded studies). We assessed the review report for possible usable data or relevant references and did not find relevant information.
Fig. 1
PRISMA flow chart illustrating screening and study selection for the first PICO and question—“Should all patients who are prescribed intramuscular BPG for secondary prevention of RHD be tested for penicillin allergy and if so, which is the best method?”
Systematic Reviews and Studies with Broader PopulationAn alternative approach to run a targeted search for relevant systematic reviews with broader population found four systematic reviews, and two additional studies were suggested by experts in the field.
A Bayesian meta-analysis by Cardoso-Fernandes and colleagues [32] looked at the frequency of severe reactions following penicillin DC in 112 primary studies including 26,595 participants with a penicillin allergy label who underwent DC. The pooled frequency of severe reactions was estimated at 0.06% (95% credible interval [95% CrI] 0.01–0.13%; I2 = 57.9%). Most severe reactions (80/93; 86.0%) consisted of anaphylaxis (estimated frequency: 0.03%, 95%CrI 0 to 0.04%; I2 = 44.2%). No patients had a subsequent fatal reaction reinforcing the safety of penicillin DC. As a limitation, the systematic review excluded studies assessing patients with specific diseases or occupations (indirectness).
Harandian and colleagues published a systematic review assessing the prevalence of immediate adverse reactions to penicillin derivatives, in patients with a reported adverse reaction to these antibiotics and the effect of age on the prevalence of reactions [43] . Their main inclusion criteria were PST or oral challenge in case of negative skin tests to establish immediate reactions. Fourteen studies were included (four only on children, six for adults, and four with mixed child and adult populations). Studies were from Denmark (n = 2), Italy (n = 2), Slovenia (n = 1), Spain (n = 1), Switzerland (n = 1), Thailand (n = 1), Turkey (n = 1), and the USA (n = 5). With a wide CI and high heterogeneity (I2 = 87.2 to 97.0%), a higher prevalence of allergic reactions was observed among adults than children. The prevalence of immediate reactions to penicillin derivatives in patients reporting a β-lactam hypersensitivity is 1.98% (95% CI, 1.35%, 2.60%) among children, 7.78% (95% CI, 6.53%, 9.04%) among adults, and 2.84% (95% CI, 1.77%, 3.91%) among mixed populations. As possible limitations, the review only included English and French literature published within a 5-year period (June 2010 to May 2015) and focused on immediate adverse reactions in patients with a reported adverse reaction.
Sacco and colleagues aimed to determine whether inpatient testing for penicillin allergy affects clinical outcomes during hospitalization [31]. They included any intervention to rule out penicillin allergy. Their systematic review included 24 studies (N = 24 to 252 participants), 18 using PST with or without oral amoxicillin challenge. Negative PST ranged from 79 to 100%. The population-weighted mean for a negative PST was 95.1% [CI 93.8–96.1]. Based on four studies, the testing was associated with decreased healthcare costs. Inpatient penicillin allergy testing result in: change in antibiotic selection—greater in ICU (77.97% [CI 72.0–83.1] versus 54.73% [CI 51.2–58.2], P < 0.01); increase in prescribing cephalosporin (range 10.7–48%) and penicillin (range 9.9–49%); decrease in using vancomycin and fluoroquinolone. The authors concluded the testing to be effective and safe to rule out the penicillin allergy and a negative test rate similar to perioperative and outpatient data. As limitations, the review focused on 15 years (until 6th December 2016) and only on English literature. Included studies had mixed design and quality and they included seven conference abstracts.
A case–control study of penicillin allergic members of Kaiser Permanent Southern California compared individuals who had penicillin allergy testing, in the setting of outpatient allergy consultation, vs matched controls who did not receive testing over a mean 3.6- to 4-year follow-up period [44]. Individuals who had penicillin allergy testing had higher exposure to penicillins and 1st and 2nd generation cephalosporins, alongside with fewer outpatient and emergency department visits, and fewer hospital days. The approach was safe, with no episodes of penicillin- or cephalosporin-associated serious cutaneous adverse reactions or anaphylaxis documented.
A systematic review by Sousa-Pinto and colleagues assessed the accuracy of penicillin allergy diagnostic tests (skin tests and specific IgE quantification) in the diagnostic evaluation of patients reporting a penicillin/beta-lactam allergy [45]. The review included 105 studies in patients reporting a penicillin allergy assessed with skin tests and/or specific IgE quantification using DC results as the reference. The accuracy of diagnostic tests was assessed with bivariate random-effects meta-analyses based on 27 studies from Canada (n = 3), Denmark (n = 1), Israel (n = 2), Italy (n = 5), Slovenia (n = 1), Spain (n = 5), Sweden (n = 1), Switzerland (n = 2), Thailand (n = 1), the UK (n = 2), and the USA (n = 4). Skin tests had summary sensitivity of 30.7% (95%CI 18.9–45.9%), specificity of 96.8% (95%CI 94.2–98.3%), and moderate discriminative capacity (c-statistic 0.686; 20 studies), and specific IgE quantification had summary sensitivity of 19.3% (95%CI 12.0–29.4%), specificity of 97.4% (95%CI 95.2–98.6%) and low discriminative capacity (c-statistic 0.420; 11 studies). Unfortunately, ARF was among the exclusion criteria in this review, posing some questions regarding indirectness.
During a period of shortage of PST reagents, between January 2007 and August 2009, Macy and colleagues prospectively evaluated 150 consecutive individuals with history of penicillin allergy using both commercial anti-penicillin IgE fluorometric enzyme immunoassays and PST [46]. The fluorometric enzyme immunoassays were negative for all 6 participants with positive PST and were also negative for the 3 participants with negative PST who subsequently had a positive oral challenge (one participant developed hives and two had non-urticarial rashes). Furthermore, all four participants with positive fluorometric enzyme assays had negative PST and negative oral challenge. These results provided evidence support to PST followed by oral challenge in case of negative PST, whilst showing that commercial fluorometric enzyme immunoassays were of no use for evaluating individuals with history of penicillin allergy.
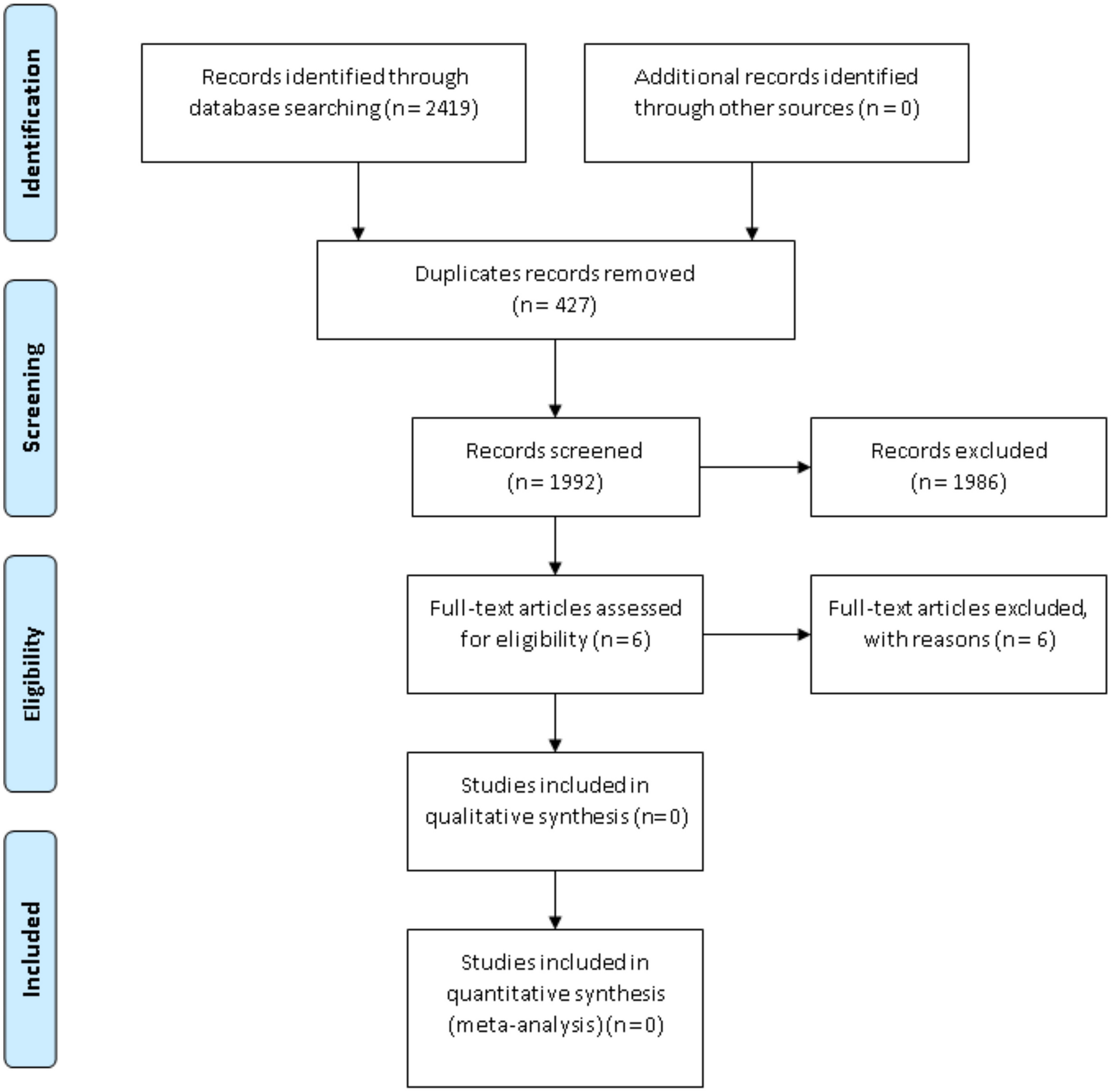
Confirmation or Delabeling of Patients with Suspected Penicillin Allergy Study Selection and DescriptionAfter assessing 516 records and obtaining the full text for 29 reports, we found five studies meeting the inclusion criteria [47,48,49,50,51] (Fig. 2). We identified 2 additional ongoing trials who seem to meet the inclusion criteria [52, 53].
Fig. 2
PRISMA flow chart illustrating screening and study selection for addressing penicillin allergy delabeling
We excluded thirteen reports because they were single-arm studies with no control groups, two studies were systematic reviews, one study had the wrong population, two studies had the wrong comparator, one study had the wrong study design, and one was a health economics analysis.
Three of the included studies were randomized controlled trials [48, 50, 51], one was a single-arm trial with historical controls [47, 54], and one was a case–control study [49]. One study [51] was a conference abstract and we contacted the authors for further information on the study.
Included participants differed across studies, with two studies [49, 51] including only adults, and the remaining [47, 48, 50] included a mix of children and adults (Table 1). One study only included pregnant patients [51].
Table 1 Study design of included studies for the second PICO and question—“In patients with suspected penicillin allergy what is the best method to delabel a penicillin allergy or to confirm a diagnosis?”Four studies included patients only with cutaneous or non-life-threatening reactions (47, 48, 50, 51). One study also included patients classified as high-risk (recent reactions/ < 1 year, and with mucosal or systemic involvement [49].
The direct DC was oral in all studies, with 2-steps in three [47, 48, 51] or 1 to 2-steps in the remainder [28, 49]. Amoxicillin only was used in two studies [26, 29], whilst the other three used other studies used other penicillin-class drugs [28, 49] and/or cephalexin [32, 47] (Table 2). A detailed description of direct DC and PST protocols is provided in Table 3.
Table 2 Interventions & baselines of participants in the included studiesTable 3 Detailed description of drug-challenge and skin testing controls Appraisal of EvidenceThe three included randomized controlled trials [48, 50, 51] had one domain with high risk of bias and ≥ 2 domains with unclear risk. The two non-randomized controlled trials [47, 49] were rated as moderate quality (Table S.1. Supplementary Material).
The GRADE framework was applied to assess the certainty of evidence (Table S.2. Supplementary Material).
Safety of the Different Delabeling StrategiesImmediate allergic reactions were observed for a minority of patients, usually of minor severity, and occurred less frequently in the DC group: 2.3% (14/604) vs. 11.5% (85/742); RR = 0.25, 95%CI 0.15–0.45, P < 0.00001 (Fig. 3A). Low heterogeneity was observed (I2 = 0%), and certainty of evidence was considered low due to double downgrading due to risk of bias.
Fig. 3
Forestplots with risk of bias assessment of the five studies (including three randomized controlled trials) for immediate allergic reactions (A) and delayed allergic reactions (B)
No deaths or cases of anaphylaxis were reported. Despite not reporting any cases of anaphylaxis, one high-risk patient undergoing oral direct DC in Stevenson et al. developed a reaction classified as severe (grade 3 out of 4: lower respiratory not responding to inhaled corticoid, or upper respiratory with airway-associated edema with/without stridor) requiring adrenaline (49). Three female patients in the low-risk group undergoing direct DC required antihistamines to deal with test-related symptoms (coughing in one, and globus sensation in two). In this retrospective study, the rate of positive tests in the PST arm was much lower in the low-risk group (9/132, with 6 with positive skin test, and 3 patients with negative skin test but reacting to subsequent DC) than in the high-risk group (52/148, with 45 positive skin tests, and 7 patients with negative skin test reacting to the DC): 6.8% vs. 35.1%. This difference was not observed for DC, with 3.6% (4/112) in the low-risk, and 3.6% (2/55) in the high-risk group.
Iammatteo et al. reported four cases with allergic reaction to direct DC: three patients with mild rash and one patient with intractable pruritus that resolved within 1 h of antihistamines. In the historical control group, out of 11 patients with allergic reactions, 2 patients required antihistamines and 1 patient required corticosteroid to deal with angioedema, rash and/or erythema (47). Mustafa et al. (2019) reported three patients with reaction to direct DC consisting of cutaneous-only manifestations, all successfully treated with oral antihistamines (48). The ten positive PST were also cutaneous only reactions. No systemic reactions or need for adrenaline were observed in this study. The PALACE trial reported only one immediate reaction to testing in each group (50). Cutaneous events occurred in both groups during the first 5 days, with 9 patients in the direct DC group and 6 in the PST requiring anti-histamines, and 1 in the PST requiring intranasal corticosteroid. In Ramsey et al. (2023), two patients had positive PST, and no serious adverse events were described in any of the groups (51).
Three studies provided data on allergic reactions beyond the initial testing. Allergic reactions reaction on the longest available follow-up are numerically lower in the DC group than in the PST group: 5.8%, 35/604, vs. 12.5%, 88/742, OR = 0.58, 95%CI 0.33–1.03, P = 0.06 (Fig. 3B). Heterogeneity was moderate (I2 = 31%), and certainty of evidence was considered very low due to downgrading based on risk of bias, inconsistency, and imprecision. Iammatteo and colleagues reported that one of the patients with normal direct DC developed a rash after concurrently receiving penicillin and lidocaine for a dental procedure (47). Stevenson et al. described 207 patients with negative DC who underwent extended challenges. Of these, 6 of 144 in the low-risk group, and 6 of 63 in the high-risk group developed mild delayed cutaneous reactions (49). In the PALACE trial, during the 5-day follow-up, there were 22 adverse events in the direct DC group, with only 8 described as allergic (immediate diffuse rash/urticaria in 2 patients, and delayed diffuse rash/urticaria in 6 patients), and 24 adverse events in the PST group, with only 4 described as allergic (immediate diffuse rash urticaria in 1 patients, and delayed diffuse rash/urticaria in 3 patients) (50).
Non-allergic adverse events were reported by two trials. Iammatteo reported 14 patients with non-allergic reactions to direct DC: oropharingeal symptoms (n = 6), pruritus (n = 5), pruritus + oropharingeal symptoms (n = 1), sinus congestion (n = 1), nausea (n = 1), and mild pruritus + mild chest tightness (n = 1). In the historical control group, tingling sensation (n = 2), gastrointestinal symptoms (n = 1), and weakness/drowsiness/lightheadedness (n = 1) were among the reported non-allergic symptoms (47). In the PALACE trial, the reported non-allergic adverse events were antibiotic-associated non-immune reactions (6 in the DC group and 2 in the PST group), nausea/vomiting/diarrhea (2 in the direct DC group), and other unspecified nonsevere adverse events (6 in the direct DC group and 18 in the control group) (50).
No studies reported any vasovagal reactions, arrhythmias, or other severe adverse events. Data on antibiotic treatment adherence and acceptability to provider and patient were not provided in any study.
Two studies provided information on costs: Mustafa et al. estimated that each PST costed $393.66 whilst each DC costed $53.66 (48), nearly 8 times lower. Ramsey et al. Reported that cost for PST per patient was $301.73 whilst DC cost per patient was $187.46 (51).
Sensitivity and Subgroup-analyses for the endpoints immediate allergic reaction and allergic reaction at the longest available follow-up are presented in Table 4. Results show lower rate of allergic reactions from most scenarios with DC, except for studies in pregnancy and adult-only populations where DC and PST have similar rate of allergic reactions. The analysis of RCT only data shows a trend for lower rate of immediate allergic reactions, and comparable rates of delayed allergic reactions.
Table 4 Sensitivity and subgroup analyses
留言 (0)