Study design
This pilot study recruited 30 children with NCFB collected from the regular patients of Pediatric Pulmonology clinic, Children’s Hospital, Ain Shams University, Cairo, Egypt from December 2020 to December 2021. Patients were enrolled if they have clinical symptoms consistent with bronchiectasis confirmed radiographically using pediatric criteria for bronchial dilation in high-resolution computed tomography (HRCT) scan and a negative sweat test [18], age between 1 and 16 years and in a clinically stable state. Exclusion criteria included presence of acute exacerbation at time of enrollement defined as increased respiratory symptoms, mainly cough, increased sputum quantity or purulence for ≥ 3 days, dyspnea or hypoxia irrespective of the duration [19], confirmed cystic fibrosis (CF) diagnosis, underlying chronic inflammatory conditions, known or suspected chromosomal abnormality, on antibiotics or anti-inflammatory drugs including inhaled and systemic steroids four weeks before the study or immunosuppressive therapy. They were compared with 30 age and sex-matched previously healthy children referred for bronchoscopy in view of suspected foreign body aspiration. Only those with normal airway anatomy, and normal microbiology BAL results were included.
Ethical considerations
Informed consent
was obtained from participants or their legal guardians before enrollment. This study was performed in line with principles of the Declaration of Helsinki 1975. Approval was granted by Research Ethics Committee of human experimentation, Faculty of Medicine, Ain shams university (FMASU MD 270/2020).
Data collection
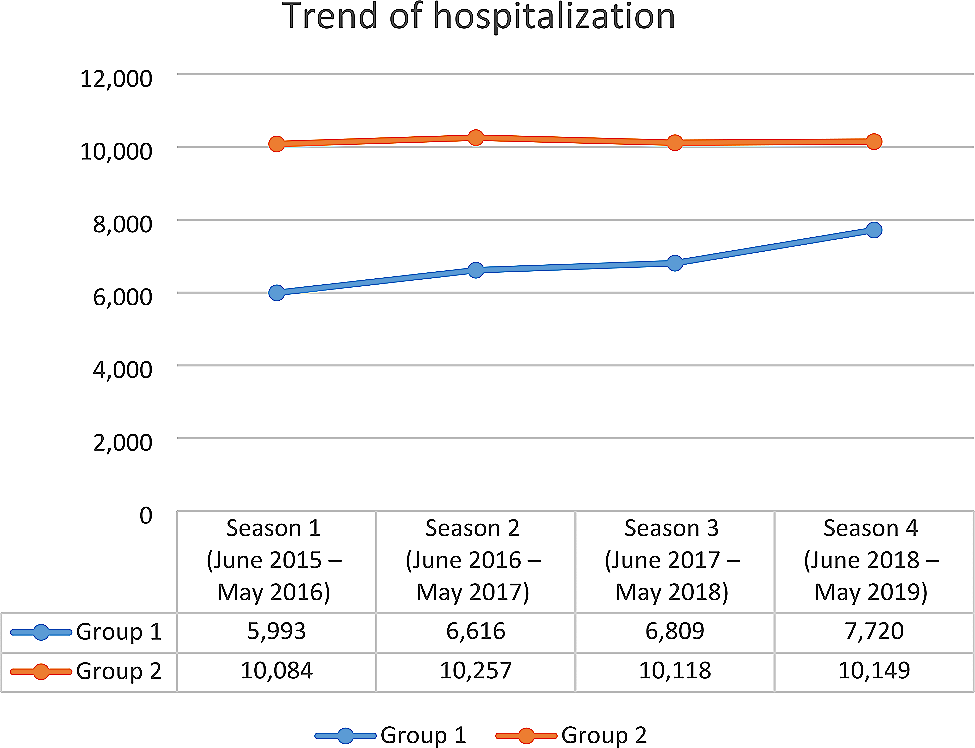
All patients were subjected to detailed history taking, laying stress on demographics, disease duration, symptoms suggestive of exacerbation, and frequency of hospitalization due to exacerbations in last 12 months. Vital data and anthropometric parameters, including weight, height, and body mass index (BMI), were recorded and plotted on centiles. Pulse oximetry was used to monitor oxygen saturation.
Routine inflammatory markers as complete blood count (CBC) and C-reactive protein (CRP) were performed at enrollment. Patients and controls with abnormal results were not included.
Non-CF bronchiectasis severity assessment tools
1.
Pulmonary function tests.
Forced spirometry was performed for enrolled subjects using JAEGER apparatus, care fusion, Germany, 2011. Standard methodology for acceptability and repeatability of spirometry was followed according to combined American thoracic society / European respiratory society guidelines [19]. The following parameters were obtained: forced vital capacity (FVC), forced expiratory volume in first second (FEV1), ratio between FEV1 and FVC (FEV1/FVC), and maximal mid-expiratory flow rate during 25–75% of expiration (MMEF25-75) and results were expressed as percentage (%) of predicted values based on age, sex, ethnicity, weight, and height. Spirometry was interpreted as normal if FEV1 and FVC % predicted were ≥ 80% and FEV1/FVC ratio > 80. Severity of obstructive ventilatory defect was graded based on FEV1% predicted values as follows: mild if > 70%, moderate if < 70 to 50%, severe if < 50 to 30% predicted [20].
2. Radiological evaluation using Modified Bhalla score and quantitative lung analysis.
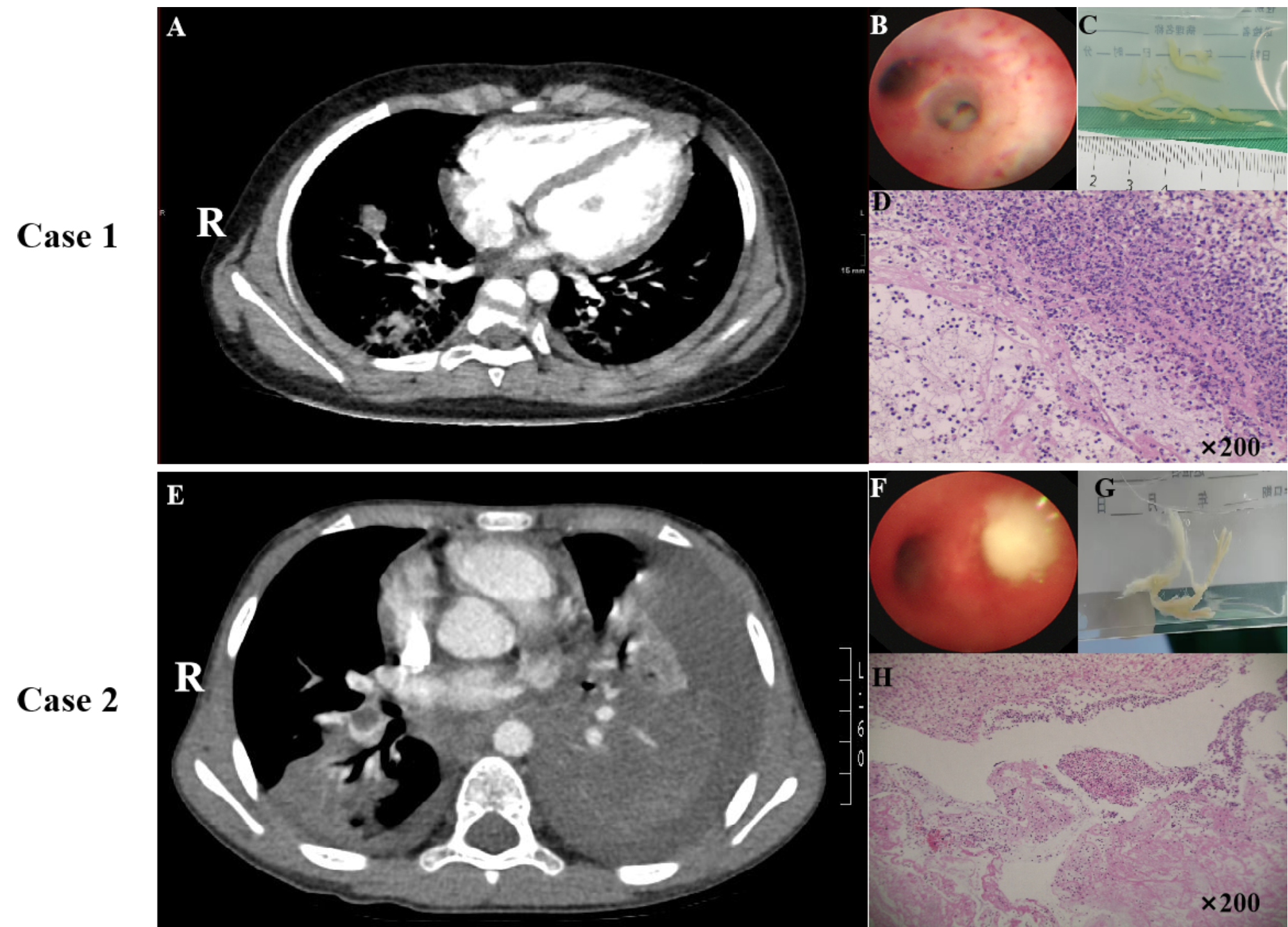
High-resolution computed tomography (HRCT) scan was performed for all enrolled patients using a 64-slice CT machine (Optima CT, GE “general electric”, USA). No specific preparations were required. Only in non-cooperative children, general anesthesia was needed to obtain scanning during suspended inspiration. In older children, scanning was taken during full inspiration. Patients were scanned in supine position with arms above the head. Image acquisition was at 1.25 mm thickness, 0.625 mm intervals using 512 × 512 matrix, tube speed 35 mm/rotation with 0.5s rotation time. The KVp and mAs were used as low as possible to limit radiation dose. Image analysis was done by an experienced radiologist blinded to patient’s condition. The following items were recorded: distribution and severity of bronchiectasis, peribronchial thickening, and severity, presence of mucus plugging, sacculations, bullae/emphysema, and consolidation/collapse. Modified Bhalla score [21] was calculated to assess radiological disease severity. Total score range from 0 to 37.
Post-processing, using Fuji 3D synapse automated software, a quantitative analysis based on CT image (CT volumetry) was performed, where volume of the diseased areas was calculated as a percentage of the total lung volume. This was referred to as percentage of lung volume affected by bronchiectasis [22].
3.
Pediatric bronchiectasis severity index.
A pediatric-specific score was adapted as an assessment tool of disease severity in studied subjects. It uses a combination of clinical (age, nutritional status, exacerbations, hospital admissions over a year period, and patient compliance), radiological and microbiological features. Depending on calculated score, disease was graded as mild if 0–4, moderate if 5–8, and severe if ≥ 9 [23]. Chronic airway colonization was determined if a pathogenic microorganism was identified in cultures from BAL and/or induced sputum samples on at least 2 occasions, 3 months apart in the previous 12 months [24].
4.
Modified medical research council (mMRC) dyspnea scale.
Degree of perceived breathlessness and respiratory dysfunction in daily living activities of enrolled patients was evaluated using mMRC scale. It is a self-reported five-statement questionnaire, ranging from grade 0 (dyspnea only on strenuous exercise) to grade 4 (dyspnea on dressing/undressing) [25].
Laboratory work-up
1.
Measurement of Lipoxin A4 level in bronchoalveolar lavage fluid (BALF).
All enrolled patients and controls underwent bronchoscopy with bronchoalveolar lavage (BALF) collection according to European respiratory society guidelines [26]. Bronchoscopy was done under general anesthesia through a laryngeal mask. Standardized protocol for BALF collection under aseptic conditions was followed by wedging in right middle lobe bronchus and lingula, then sterile normal saline (1-2 ml/kg) was instilled and suctioned immediately. Collected samples were transported in sterile containers to laboratory where total and differential cytology was immediately determined, microbiological cultures were performed and a sample was stored at -20◦C for further use. BAL samples were centrifuged for 20 min at 1000xg. The supernatants were collected for measurement of lipoxin A4 concentration using a human lipoxin A4 ELISA kit (E0612Hu, Bioassay Technology Laboratory, China). LXA4 in samples and standards competed with that is coated to wells for the Biotinylated Detection antibody specific to LXA4. After a washing step, an Avidin-Horseradish peroxidase (HRP) conjugate was added and incubated followed by addition of a TMB substrate solution. The reaction was terminated after 10 min by the stop solution. The optical density was measured at 450 nm and concentration of LXA4 was calculated using a standard curve with an intra- & inter-assay CV of 5.6 & 7.7 respectively, a range of 5-2000 ng/ml and sensitivity of 2.47ng/l.
2.
Genotyping of ALOX-15,c.-292 C > T (rs2072510) single nucleotide polymorphism (SNP) using TaqMan-based Real-time PCR.
Venous blood samples were collected from all participants under aseptic conditions in EDTA-containing tubes and stored at -20◦C. DNA was extracted from plasma samples using QIAamp DNA blood kits, catalog no: 51,104 (Qiagen, Hilden, Germany). DNA concentration of 50 ug/ml was determined and DNA purity was detected by determination of A260/A280 ratio. All patients and controls were genotyped for ALOX-15,c.-292 C > T SNP using Applied Biosystems TaqMan SNP genotyping assays ”ALOX-15 C/T rs2072510, catalog no:4,351,379 (ThermoFisher Scientific, Germany) and PCR TaqMan Genotyping Master Mix kit, cat no:4,371,353 (ThermoFisher, Germany). The thermal cycling protocol was optimized as follows: 95◦C for 10 min for AmpliTaq Gold, UP enzyme activation, followed by denaturation step at 95◦C for 15 s and annealing/extension at 60◦C for 1 min for 40 cycles. The qPCR was performed on Applied Biosystems PCR instrument (ThermoFisher Scientific, Germany).
Statistical analysis
There were no previous data to inform a power calculation, so sample size in this pilot study is opportunistic based on availability of samples. 60 participants is a conservative estimate to detect a statistically significant result. Statistical package for social science, version 23.0 (SPSS Inc., Chicago, Illinois, USA) was used for data management and statistical analysis. Quantitative variables were presented as mean, standard deviation (SD), and ranges when parametric, median, and interquartile range (IQR) when non-parametric. Categorical variables were presented as numbers (n) and percentages (%). Chi-square test was used for comparison between 2 groups regarding qualitative data. For comparison between 2 groups with quantitative variables, independent t-test (parametric) and Mann-Whitney test (non-parametric) were used. Kruskall-Wallis test was used for comparison between more than 2 quantitative variables (non-parametric). Alleles frequency was calculated using gene counting method, Chi-square was used to test the difference between groups as regards genotypes and alleles and to prove Hardy-Weinberg equilibrium. Association of Genetic polymorphism with bronchiectasis was assessed by exact logistic regression model, odds ratio (OR), and 95% confidence interval (CI) were calculated. Spearman correlation coefficients were used for correlation analysis. Confidence interval was set at 95%, margin of error accepted was set at 5%. P-value was considered significant if < 0.05.



留言 (0)