
記住我


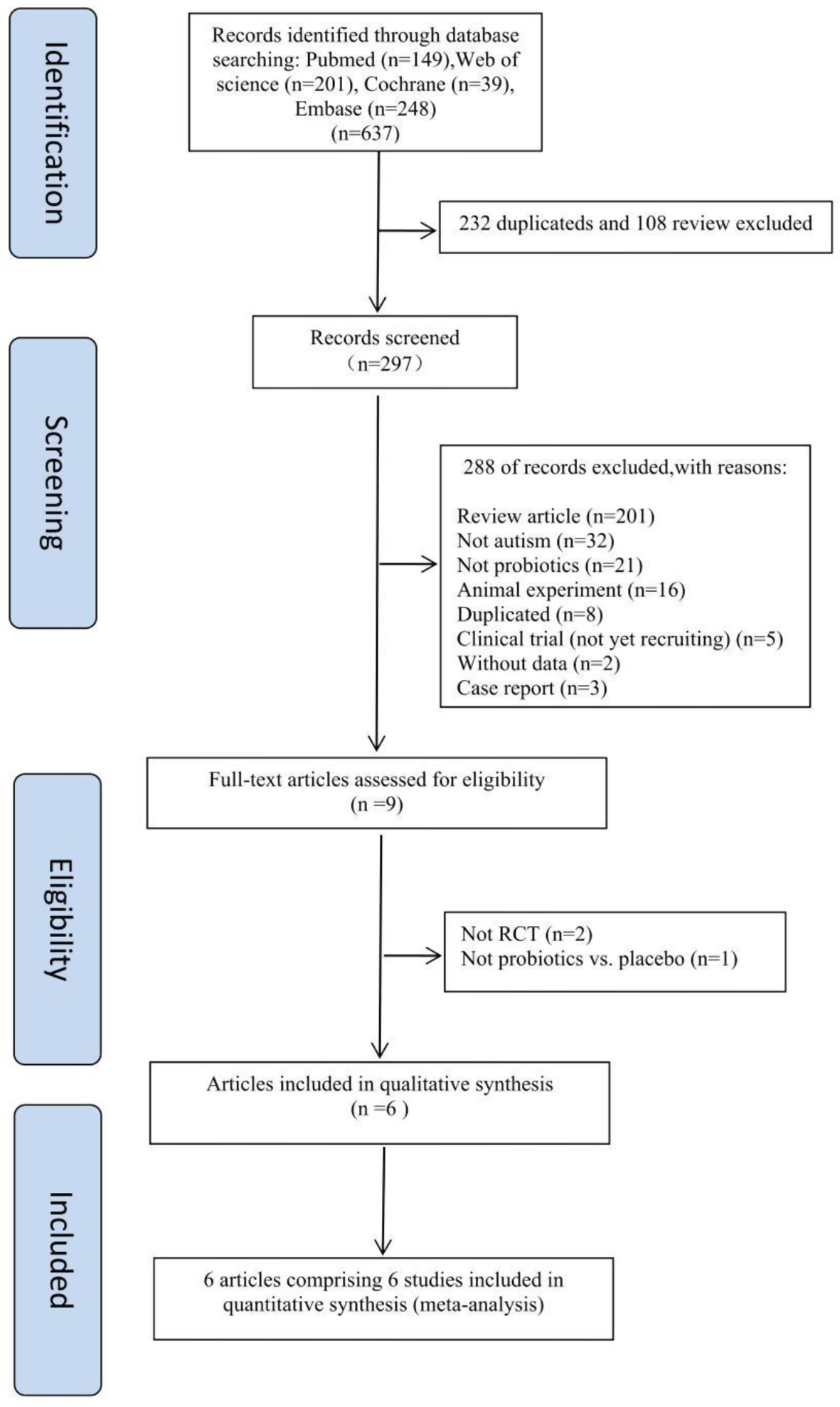
The study selection process is illustrated in Fig. 1, according to PRISMA 2020 flow diagram for new systematic reviews. We identified 722 studies (664 on PubMed, 58 on Scopus). We merged the two databases and removed 174 duplicates. In the identification phase, 548 records were included based on titles and abstracts, while 489 records were excluded because they did not match the aims of the study. In the screening phase 59 studies were included, while 2 studies were excluded because they were not available in NILDE (Network for Inter-Library Document Exchange). A total of 57 studies were assessed for eligibility by full-text reading and 48 studies were excluded considering the following criteria: follow up < 2 years (n = 25), not exclusive breastfeeding (n = 9), did not report effect of breastfeeding and long-term outcome (n = 5), did not assess SGA or IUGR infant (n = 9). Reviews (n = 4) and commentary (n = 1) were excluded and none of the secondary references were eligible for our study [8, 20,21,23]. Finally, 9 studies were included in the analysis.
Fig. 1
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only
Study characteristicsGeneral characteristics of the analysed studies were reported in Table 2. The nine studies that were included in the final analysis range from 2002 to 2021 [24,25,26,27,28,29,30,31,32]. Three studies analysed benefits associated with breastfeeding in SGA and adequate for gestational age (AGA) newborns [25, 28, 31]. Three studies executed a comparison between exclusive breastfed and non-exclusive breastfed SGA newborns [26, 30, 32]. One study compared exclusively breastfed longer than 12 weeks and breastfed for shorter periods SGA newborns [27]. One study performed a comparison between breastfed longer than 6 months and breastfed for shorter periods in foetal growth restriction (FGR) newborns [29]. One study compared SGA newborns who were breastfed or not breastfed during hospitalisation [24]. Exclusively one research studied the use of donor breast milk [32]. There was wide variability in sample size: the smallest study included 30 infants (20 SGA vs. 10 AGA) [28], while Rao et al. conducted the largest one comprising 568 newborns, including 243 SGA newborns [27]. Furthermore, among the 9 selected studies, 7 were prospective cohort studies, 1 was a case-control study, 1 was a randomized controlled trial. All the studies were written in English, except for one which was published in Spanish and English.
Table 2 Table of evidence of included studiesRisk of bias in studiesROBINS-I was used to determine the risk of bias for studies and it was reported in Table 2. The Cochrane Risk of Bias tool (RoB V.2.0) was used to determine the risk of bias for randomized controlled trials (Table 2). Level of quality of evidence and studies bias assessment were reported in Table 2.
Results of individual studies and synthesis of resultsThe nine studies which fulfilled inclusion criteria were related to four health domains based on literature research: Neurodevelopment, Cardiovascular, Somatic growth and Bone mineralization, Atopy. They were summarized in Tables 2 and 3 according to the same classification. In the Cochrane Handbook for Systematic Reviews of Interventions is stated that meta-analysis should only be executed if studies included are sufficiently homogeneous in terms of participants, interventions and outcomes to provide a meaningful summary [33]. Different topics in our systematic review have been analysed and presented separately but a meta-analysis was not performed because the study groups were not homogeneous and contained some grade of clinical diversity.
Table 3 Main results of the studies included in the systematic reviewNeurodevelopmentIn 2015, Gibertoni et al. examined the impact of human milk feeding on neurodevelopment at 24 months corrected age in SGA and AGA preterm newborns. The in-hospital feeding protocol prioritised human milk whenever possible. Newborns were fed in 34.5%, 36.1% and 29.4% of the cases by breast milk, mixed milk, or formula milk, respectively. The babies fed by breastfeeding did not take fortified milk. Fortification of bottle-administered human milk was routinely done during hospitalisation at standard dosage with a commercial preparation. Fortification began when enteral intake reached 100 ml/kg and it was interrupted when a body weight of 3.5 kg was achieved. During hospitalisation, it was administered preterm formula milk which contained 80–90 kcal/100 ml and proteins 2–2.3 g/100 ml. After discharge, it was recommended post-discharge formula milk which contained 72–74 Kcal/100 ml and proteins 1.8–1.9 g/100 ml until the weight of 3.5 kg was achieved. The results showed that infants who were fed with human milk scored approximately 3.80 points higher on the Griffiths Mental Development Scale compared to those who received formula milk. This effect remained significant even after adjusting the analysis for complications, growth restriction, and socio-economic status. SGA newborns were associated with a higher probability of complications, including sepsis and the need of mechanical ventilation. They were directly linked to poorer neurodevelopmental outcomes. However, the use of human milk during hospitalisation helped to mitigate the negative effects of lower gestational age and being SGA, resulting in improved neurodevelopmental outcomes (p = 0.050). In this study a considerable loss to follow-up (28.6%) was registered. In the analysis there was lack of detailed information about human milk feeding (e.g. duration and dosage) and timing of switching from human to formula feeding. We have identified a significant degree of indirectness in the assessment of bias-related risks [24]. Savchev et al. led a prospective cohort study, the aim was to evaluate the neurodevelopment of SGA vs. AGA term infants in the absence of placental insufficiency. Neurodevelopmental outcome was evaluated at 24 months corrected age using the 3rd edition Bayley Scales of Infant and Toddler Development, which evaluated cognitive, language, motor, social-emotional and adaptive. A total of 223 infants (112 SGA and 111 AGA) were included. The groups differed significantly by socioeconomic status and gestational age at delivery. All neurodevelopmental domains studied were poorer in the SGA group, reaching significance for cognitive (92.9 vs. 100.2, p = 0.027), language (94.7 vs. 101, p = 0.025), motor (94.2 vs. 100, p = 0.027) and adaptive scores (89.2 vs. 96.5, p = 0.012). Likewise, the SGA group had a higher risk of low scores in language (OR = 2.63; p = 0.045) and adaptive (OR = 2.72; p = 0.009) domains. The study showed that breastfeeding did not significantly influence the score in any domain as the percentage of breastfed children was comparable in both groups. Anyway, Bayley Scales could be imprecise as it could underestimate neurodevelopmental disorders in infants or detect differences in neurodevelopmental performance which are clinically irrelevant. Moreover, the lower socioeconomic status of the SGA group was a confounding factor [25]. A study conducted by Slykermann et al. investigated the relationship between breastfeeding and intelligence test scores in 223 versus 308 children who were born SGA and AGA, respectively. Researchers used the Stanford Binet Intelligence Scale. The results demonstrated a significant association between breastfeeding and higher intelligence scores at the age of 3–5 years in SGA children. The study showed that in SGA infants there was a significant positive correlation between average intelligence score and exclusive breastfeeding duration in the univariate (p = 0.02) and multivariate (p = 0.03) study. In fact, children from the SGA group who were exclusively breastfed for 5 months or longer, had the highest intelligence scores among all the groups (mean = 113.2). However, SGA children were breastfed for shorter periods compared to AGA children. It was not found a difference in intelligence scores between SGA and AGA children. In the analysis anthropometric parameters, which were relevant in this type of population, were not reported (e.g. birthweight) [26]. Rao et al. performed a cohort study to evaluate the effect of exclusive breastfeeding on cognitive development in SGA and AGA term infants, also considering sociodemographic and maternal factors. This study was conducted on a final sample of 519 infants (220 SGA births and 299 AGA). It was assessed IQ at 5 years of age according to the Bayley Scales of Infant Development. This study found that longer duration of exclusive breastfeeding was associated with higher IQ scores at 5 years of age for both groups. The benefits of exclusive breastfeeding on cognitive development were particularly significant for SGA infants. SGA infants exclusively breastfed for more than 12 weeks (mean 109, SD 16) had a significantly higher total IQ compared to those breastfed for shorter periods (mean 100, SD 14; p < 0.0001). The study also found a significant association between exclusive breastfeeding duration and factors such as maternal IQ, maternal education, family income, and the child’s attendance at kindergarten. Overall, these findings supported the recommendation to exclusively breastfeed infants for at least 24 weeks to promote cognitive development. In this study, a potential confounding factor was the lack of information about indicators that reflected parenting attitudes, home environment and child-rearing practices. Moreover, maternal education was not determined for enrolled women [27].
CardiovascularIn a small sample of breastfed SGA and AGA term babies, Santiago et al. recently evaluated the linkage between the duration of breastfeeding and cardiometabolic parameters until pre-school age. All children were breastfed for at least 6 months, but 36.9% and 41.7% of newborns received complementary feeding in the SGA and AGA group, respectively. It was observed a lower adiposity in the SGA group compared than AGA group at preschool age (percentage of fat in SGA and AGA group, median (interquartile range) = 8.2 (5.7–13.9) and 14.7 (12.01–19.39), respectively; p = 0.005). A strong positive correlation was found between body mass index (BMI) at the age of 4–6 years and body fat indicators in SGA group [cephalic perimeter (r = 0.7, p = 0.001), waist circumference (r = 0.6, p = 0.002), arm circumference (r = 0.9, p < 0.001), mid-upper arm muscle area (MUAMA) (r = 0.9, p < 0.001) and sum of skinfolds (r = 0.7, p = 0.001)] and in AGA group (cephalic perimeter (r = 0.62, p = 0.03), cephalic circumference (r = 0.9, p < 0.001), arm circumference = 0.8, p = 0.003) and MUAMA (r = 0.6, p = 0.03)]. In the SGA, there was no relation between breastfeeding time and BMI, cephalic circumference, cephalic perimeter, and skinfolds, while a strong negative correlation was found in the AGA group between breastfeeding and BMI (r = -0.8, p = 0.001), cephalic circumference (r = -0.7, p = 0.007) 0.7, p = 0.009), MUAMA (r = -0.7, p = 0.01). This study had several limitations: the sample size was small and dropout rate during follow-up was high (45% of the initial population), family-related factors that could influence the outcome were not considered in the analysis (e.g. familiar lifestyle of recurrence of metabolic disorders), there was not a control group of non-breastfed babies and there was a lack of details about the complementary-fed group (e.g. duration, proportion of formula milk). Finally, the analysis was not completely reported and part of the object of the present review was evaluated indirectly [28]. In 2016, Rodriguez-Lopez et al. conducted a cohort study that explored the influence of postnatal nutrition on cardiovascular remodelling induced by FGR in comparison with AGA newborns. The two groups were breastfed for a similar duration (median = 4 months, IQR 2–8). The authors confirmed that FGR is the strongest predictor of left ventricular sphericity index (LVSI) (coefficient: −0.4038, 95% CI − 0.4610; −0.3467; p < 0.001). Regarding postnatal nutrition, in the overall analysis of the entire sample, only prolonged breastfeeding (> 6 months) showed an independent positive association to LVSI (coefficient: 0.0982, 95% CI 0.0133–0.0183; p = 0.02). Breastfeeding was not statistically associated with carotid intima-media thickness (cIMT) and blood pressure (BP). Finally, the combined effect induced by breastfeeding, healthy-fat dietary intake, and overweight/obesity on LVSI and cIMT in FGR children was assessed. It was found that FGR children who were breastfed > 6 months and had a healthy-fat dietary intake showed LVSI and cIMT values closer to AGA newborns. Several data were not considered in the analysis, such as information on potential maternal and family-related factors. Blood pressure was evaluated through a single time point value, which could ignore daily fluctuations [29].
Somatic growth and bone mineralizationVizzari et al. in 2022 studied factors associated with failure to perform catch-up growth in a cohort of 175 SGA late-preterm babies. At the time of hospital discharge, the newborns were fed exclusively by human milk, complementary feeding, or exclusive formula milk in 18%, 36% and 46% of the cases, respectively. Enteral feeding was started within the first 24 h of life in all newborns who were in stable clinical conditions. Fresh mother’s milk represented the first choice and mothers were encouraged to directly breastfed their infants or, when this was not possible, to express their milk soon after birth. According to the nutritional procedure of their center, human milk was fortified with bovine milk-based fortifiers in all newborns with weight ≤ 1800 g and with enteral intake ≥ 80 ml/kg/day. Breast milk was more than 50% of the total intake. If breastmilk was insufficient or not available, formula milk feeding was started. It was demonstrated that infants who had not successfully caught-up weight at 12 months were at higher risk of not reaching catch-up growth at 36 months both for weight (OR = 9.31, 95% IC 4.28–20.28; p < 0.001) and length (OR = 34.65, 95% IC 11.46-104.77; p < 0.001). In this study, logistic regression also demonstrated a significant association between the type of feeding during hospitalisation and the probability of having worse growth trajectories during the entire follow-up: in fact, neonates who did not receive any human milk during hospital stay had lower probability of reaching the 10th percentile for weight (OR = 0.59, 95% IC 0.40–0.9; p = 0.011) and length (OR = 0.57, 95% IC 0.33–0.99; p = 0.046) at 36 months. Furthermore, this study did not test the association between the type of feeding and head circumference growth in SGA babies. In the current study, it was missing a body composition assessment and analysis of breastfeeding duration to evaluate a possible dose-dependent effect of human milk. Factors that could interfere with feeding decisions (e.g. jaundice, hypoglycaemia) were not considered in the analysis [30]. A randomized trial conducted by Fewtrell et al. in 2009 evaluated the effect of early diet in infants born preterm (< 37 weeks) and birthweight < 1850 g on peak bone mass at 20 years. A total of 201 infants were enrolled, of whom 34 were born SGA, and they were followed-up for 20 years. They were randomized according to the type of feeding in banked donor breast milk (BBM) group or preterm formula (PTF) group. Bone area (BA) and Bone Mineral Content (BMC) were evaluated by Dual X-ray Absorptiometry. At follow-up, BA and BMC were higher in the BBM group by 5.7% for whole body BA, 6% for whole body BMC, 8.6% for lumbar spine BA and 7.7% for lumbar spine BMC (80% statistical power, p = 0.05). There were no significant differences in bone turnover markers between groups. Results of the randomized dietary comparisons did not differ between SGA babies below or above 1250 g, and between SGA and AGA babies. There was no significant interaction between the birthweight category and randomized diet group on later bone outcome. In the most vulnerable group of newborns– those born SGA with birthweight < 1250 g– there was no significant differences nor trends in bone outcome measures according to early diet: 7 received BBM (50 kCal/100 mL, 1.3 gr of proteins/100 mL, 33 mg of Calcium/100 mL, 14 mg of Phosphorus/100 mL, without mineral or nutrient fortification), 12 TF (68 kCal/100 mL, 1.45 gr of proteins/100 mL, 35 mg of Calcium/100 mL, 29 mg of Phosphorus/100 mL) and 11 PTF (80 kCal/100 mL, 2 gr of proteins/100 mL, 70 mg of Calcium/100 mL, 35 mg of Phosphorus/100 mL). The authors conducted a punctual analysis of the study biases and limitations, which mainly were selection population bias, generalisability of the results and detrition of information due to long follow-up [32].
AtopyA New Zealand case-control study evaluated the prevalence of Atopic Dermatitis (AD) in 3–5 years infants born SGA and AGA. It was discovered that babies breastfed for more than 6 months had an increased risk of AD compared to those not breastfed (OR 9.95, 95% CI 2.66–37.14; p = 0.002). Furthermore, no significant difference in the AD prevalence between AGA and SGA infants was reported (16,7% and 14.7%, respectively; p = 0.52). The study highlighted how breastfeeding did not worsen atopy outcome in infants born SGA, in fact they had equivalent risk as breastfed AGA. Even if it was not found any association between low birthweight and AD at 3–5 years, it could not be distinguished whether this phenomenon could be observed only for some forms of atopic disease or whether it appeared after the follow-up time. The main limitation of this research was dropout rate of subjects during the follow-up and a homogeneous population (mostly New-Zealand Europeans), with a high mean socioeconomic status [31].
留言 (0)