Mosaic overgrowth syndromes are a group of uncommon diseases presenting as asymmetric, segmental, and often progressive overgrowth involving any tissue type. Clinical presentations are discordant ranging from isolated malformations to life-threatening conditions. These syndromes result from mosaic somatic, post-zygotic mutations in genes involved in cell growth and proliferation. The PI3K/AKT/mTOR signaling pathway is mainly involved. Proteus syndrome is an AKT1-related syndrome [5].
PS was rarely reported in Tunisian children. This syndrome remains little-known in our country, and our case report emphasizes an illustrative phenotype. In addition, our case is not limited to the clinical presentation but specifies the radiological particularities, a key point in the diagnosis and management of this syndrome. Our main limitation is the absence of a genetic study, but this does not hinder the diagnosis.
Proteus syndrome (OMIM # 176,920) is a rare overgrowth condition. It was first described in 1979, by Hayden and Cohen, in two patients [1]. It is a highly polymorph and complex disease that associates overgrowth of multiple tissues and malformations. No two patients with PS are exactly alike. Most of the affected persons appear healthy at birth, but typically during the child’s first year, some parts of their bodies begin to grow faster and larger than they should [6].
Diagnosis of PS is challenging and evolving. Its intrinsic variability made it necessary to establish diagnostic criteria in 1999 [7]. These criteria were revised in 2006 [4].
A mosaic activating AKT1 mutation (c.49G > A, p.Glu17Lys) was identified in PS. This was first published in 2011 [8].
Biesecker et al. in a study published in 2019 presented a new approach to diagnose PS. Most of the diagnosis criteria were used unmodified (Biesecker, 2006; Biesecker et al., 1999). However, other factors were added. It was about pulmonary embolism, vein thrombosis, and other tumor types testicular cystadenomas/adenocarcinomas and meningiomas. Cardiac septal lipoma was also added in the category “lipomas/dysregulated adipose. Finally, the authors added two negative criteria: substantial prenatal extracranial overgrowth and ballooning overgrowth since uncommon in PS. Subsequently, they set a boundary at ≥ 15 points to consider an individual to have a clinical diagnosis of PS in the absence of an AKT1 variant. Individuals with a score of ≥ 10 points and a pathogenic mosaic variant in AKT1 were considered as having AKT1-related PS. In the case of a score of 2 to 9 points associated with pathogenic mosaic variant in AKT1, the diagnosis of AKT1-related overgrowth spectrum was retained [9]. The diagnosis of PS was retained in our patient in 2008 based on the Biesecker et al. 2006 criteria [4]. This diagnosis was reassessed according to Biesecker et al. 2019 criteria [9]. According to this new approach, our patient has a score of 16 (all general criteria; asymmetric, disproportionate overgrowth of limbs, and scoliosis (5 points); overgrowth of adenoids and liver (5 points); lipomas (2 points); linear epidermal nevus (2 points); and venous malformations (2 points)). Screening for AKT1 mutation has not been done due to financial considerations. Although we have no genetic confirmation for PS, this diagnosis was retained since we have a score of 16. Other syndromes partially superimposable to PS such as CLOVES syndrome, neurofibromatosis 1, or PTEN hamartoma tumor [10] were excluded based on clinical, histological, and radiological presentation in our patient.
PS is also characterized by orthopedic complications which are one of the most challenging medical problems. Various cutaneous and subcutaneous lesions (lipomas, vascular malformations and several types of nevi) are also evocative. Most commonly vascular malformations are of capillary type. However, some patients have venous malformations. Arterial vascular malformations are uncommon in PS. Intracranial arteriovenous malformations were described in one case [6, 7].
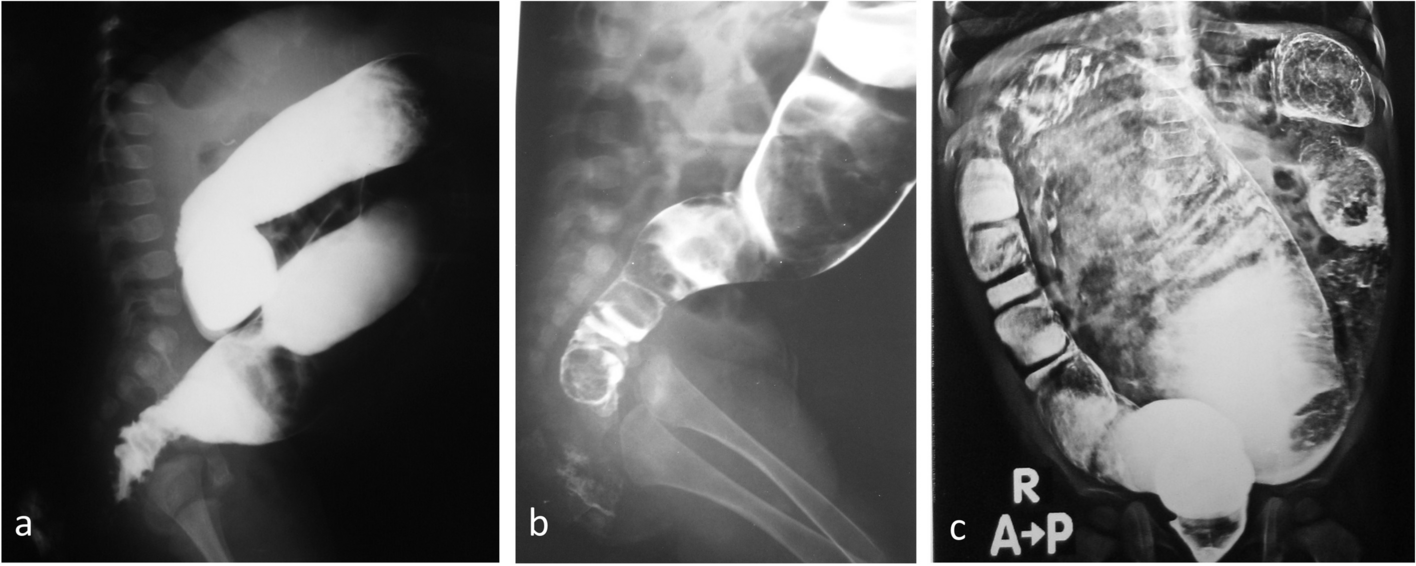
The typical ultrasound aspect of venous malformation is a polycystic, sponge-like, pseudo-tumorous lesion positioned subcutaneously and composed of complex and communicating venous vessels [2, 11]. The separating walls may be of variable thickness which renders the B-mode appearance very inhomogeneous. Thrombotic precipitates filling the vascular lumen are sometimes found. They are due to vascular wall abnormalities and to very low blood flow velocities. Indeed, patients with PS are at risk to get deep vein thrombosis, which can lead to pulmonary embolism [12]. Males appear to be at greater risk for thrombosis than females. It is important for doctors caring for people with PS to be aware of this risk [13]. Our patient presented a thrombosis 8 years after initial diagnosis.
Accurate management of patients with PS can be very well assessed through several imaging modalities.
Multiple imaging techniques are useful in the evaluation of PS. A radiograph skeletal survey is needed to identify bone anomalies. CT of the chest is helpful in the evaluation for pulmonary embolism. Abdominal and pelvic CT or MRI can be used to evaluate visceromegaly and to search for asymptomatic but potentially aggressive lipomatosis. Central nervous system MRI is needed to identify brain anomalies in patients with neurologic symptoms [2, 11].
Ultrasonography is very useful to characterize the subcutaneous lesions. Besides, it offers, with the use of the Doppler, the possibility to assess vascular malformations and to easily diagnose venous thrombosis. The latter occurs at an increased frequency in PS and exposed to pulmonary embolism major cause of premature death.
The 2004 guidelines indicate for patient assessment [2]:
–Serial clinical photography
–Initial skeletal survey with targeted follow-up radiographs
–MR imaging of clinically affected areas and in asymptomatic patient, an MRI of chest and abdomen
–Dermatologic and orthopedic consultations as long with a pediatric management
Radiologic findings are multiple. Table 2 summarizes the most common ones in patient with PS [2]. The current treatment of PS is mainly symptomatic and aims to decrease disability and promote a better quality of life. AKT1 inhibitor miransertib seems to be an interesting molecule to investigate [13].
Table 2 Radiologic findings in Proteus syndrome



留言 (0)