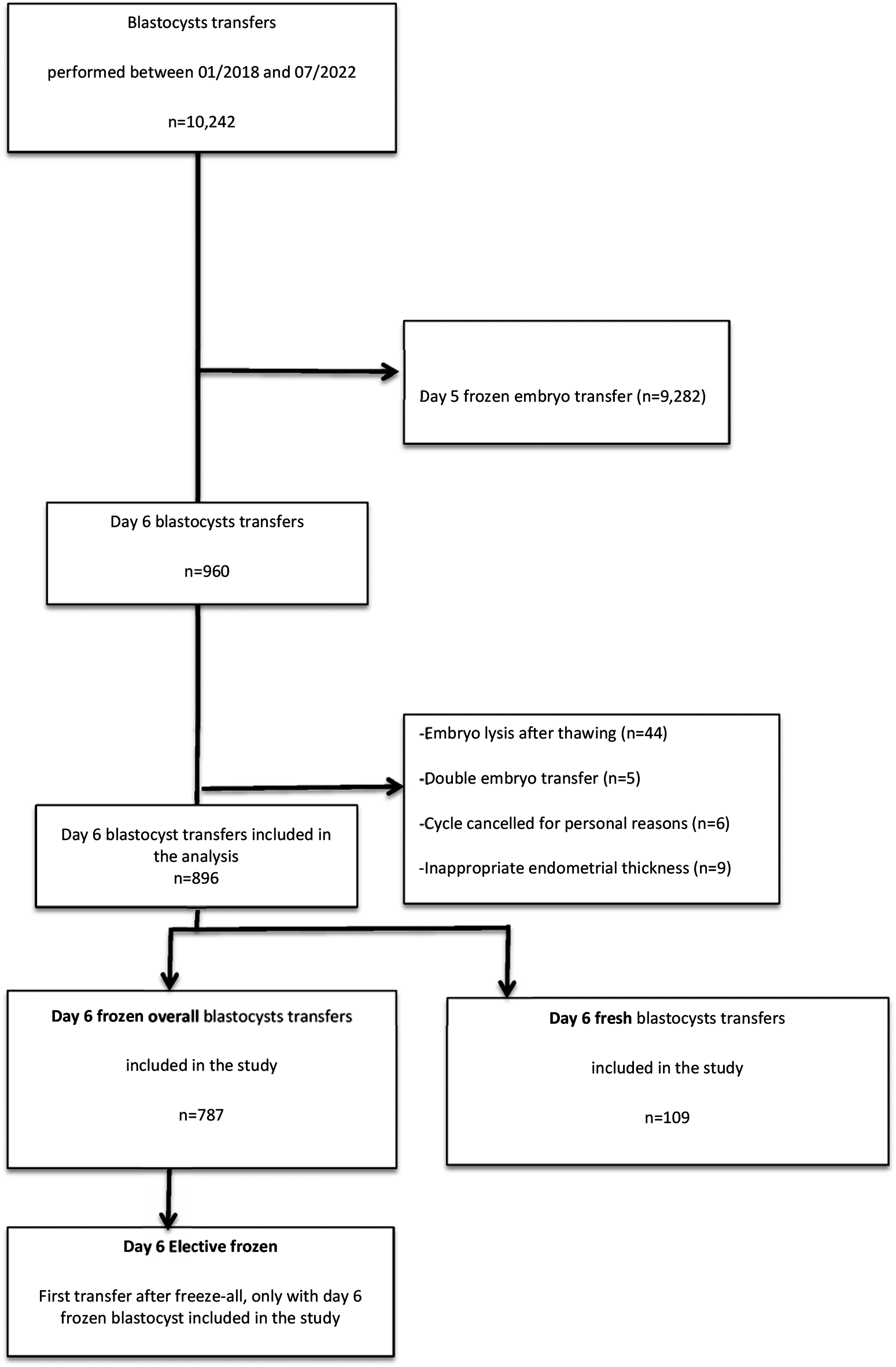
We conducted an observational, retrospective, cohort study that included infertile patients for whom a blastocyst transfer after an IVF/intracytoplasmic sperm injection (ICSI) cycle was performed in our Assisted Reproductive Technology (ART) center between 01/01/2018 and 01/07/2022. The inclusion criteria were: women ≤ 42 years of age, having one or more slow-growing blastocysts expanded on D6 available for transfer; and a single D6 blastocyst transfer (≥ B3 according to the Gardner classification). The exclusion criteria were as follows: embryo lysis after thawing, double embryo transfer, cycle canceled for personal reasons, or inappropriate endometrial thickness (< 6 mm). Patients were only included once in the analysis.
The study was approved by local ethics committees (Ethics Committee of Cochin Hospital, Research License AAA-2023-09021) and the National Data Protection Authority (Commission Nationale de l’Informatique et des Libertés, CNIL n°1,988,293 v0).
Data collection
After a medical consultation, the following data were prospectively collected for the patients: age (years), IVF/ICSI rank, type of infertility (primary or secondary), infertility causes (e.g., ovulatory disorder, male factor, tubal factor, endometriosis, premature ovarian failure, or idiopathic) [8], body mass index (BMI), smoking habits, day 3 FSH and estradiol, antral follicle count (AFC), and AMH (Anti-Müllerian Hormone) level.
Controlled ovarian stimulation (COS) protocol
Women were stimulated, monitored, and managed according to our institutional clinical protocols as reported previously [9]. Final oocyte maturation was triggered when ≥ 3 ovarian follicles with a diameter of ≥ 17 mm were visible by ultrasound and when the estradiol (E2) levels were ≥ 1000 pg/mL. Final oocyte maturation was achieved using either a single injection of 0.2 mg of gonadotropin-releasing hormone (GnRH) agonist (triptorelin, Decapeptyl®, Ibsen France) or 250 µg of recombinant human chorionic gonadotropin (rhCG) (Ovitrelle, Serono, France). Oocyte retrieval was performed under vaginal ultrasound guidance 36 ± 2 h later.
Fertilization methods and embryo culture and scoring
After retrieval, oocytes were washed and incubated in 50 µL of IVF medium droplets for 2–3 h at 37 °C (IVF, CooperSurgical, USA). IVF or ICSI was performed according to biological and clinical indications. Cumulus–oocyte complex (COC) was conventionally inseminated with nearly 6,000 motile spermatozoa/COC. Before ICSI, cumulus cells were removed mechanically after exposure to hyaluronidase (80 IU/mL) (FujiFilm, Irvine Scientific, USA). Only metaphase II oocytes were injected. Fertilization was assessed 16–18 h post insemination/injection, and zygotes were individually maintained in extended culture until the blastocyst stage in 40 µL of CSCC medium droplets (FujiFilm, Irvine Scientific, USA) under mineral oil (FujiFilm, Irvine Scientific, USA) and incubated at 37 °C in a controlled atmosphere (5.5% CO2, 5% O2). At the blastocyst stage, embryo quality was assessed on D5 and D6 according to the Gardner classification, which takes into account the expansion grade as well as the inner cell mass (ICM) and trophectoderm (TE) development [10]. Based on this classification, only expanded or hatching top- (B3 AA, B4 AA, and B5 AA), good- (B3 AB/BA/BB, B4 AB/BA/BB, and B5 AB/BA/BB), and fair- (B3 AC/BC/CA/CB, B4 AC/BC/CA/CB, and B5 AC/BC/CA/CB) quality embryos were selected for transfer and cryopreservation by vitrification. Only expanded blastocysts (≥ B3) were transferred during the study period because of our embryo observation timing policy. Indeed, before embryo transfer or vitrification, blastocysts were observed at D5 in the morning as well as in the afternoon for those that were between grades B2 and B3 in the morning. Slowly developing blastocysts at D5 (B1 and B2 grade) were maintained in culture until D6 for fresh transfer, cryopreservation, or destruction.
Blastocyst vitrification and thawing procedures
Blastocyst vitrification was performed using closed CBS-VIT High Security (HS) straws (Cryo Bio System, France) in combination with DMSO-EG-S as the cryoprotectants (Vitrification Freeze Kit, FujiFilm, Irvine Scientific, USA). The first step of the vitrification procedure consisted of exposing the embryos to cryoprotectants, and this was carried out at room temperature (approximately 20 °C). Each blastocyst was first incubated for 1 min in a 50 µL droplet of HEPES-buffered culture medium. It was then transferred into two 50 µL droplets of diluted equilibration solution (ES) containing 7.5% (v/v) DMSO and 7.5% (v/v) ethylene glycol, and incubated for 2 min in each droplet before being transferred into a third 50 µL droplet of ES solution and incubated for a further 10 min. The blastocyst was then transferred consecutively into four 25 µL droplets of vitrification solution (VS) containing 15% (v/v) DMSO, 15% (v/v) ethylene glycol, and 0.5 M sucrose and then immediately loaded onto the CBS-HS straw. Each straw containing a single blastocyst was then sealed and plunged into liquid nitrogen.
On the day of embryo transfer, the selected blastocyst with the highest score was thawed using an Irvine Scientific Thaw Kit (FujiFilm, Irvine Scientific© Thaw Kit, USA). A Petri dish containing one 300 µL droplet of thawing solution (TS: 1.0 M sucrose in HEPES-buffered HTF medium) was heated and maintained at 37 °C. The straw was transferred from the liquid nitrogen storage container. After cutting the straw and pulling out the capillary from the straw, the gutter was immediately placed in the heated TS droplet, allowing the blastocyst to be released from the gutter and maintained at 37 °C for 1 min. The blastocyst was then incubated twice for 1 min at room temperature in two 50 µL TS droplets and transferred to the first of two 50 µL dilution solution droplets (DS: 0.5 M sucrose in HEPES-buffered HTF medium) followed by a 2 min incubation in a second DS droplet. Finally, the blastocyst was washed in three droplets (50 µL each) of wash solution (HEPES-buffered HTF medium) for 3 min. The blastocyst was then transferred into a CSCC culture medium (CSCC, FujiFilm, Irvine Scientific, USA) droplet in a culture dish. After warming, the blastocyst quality was evaluated when re-expansion occurred, in which case the quality was always the same as before vitrification. In case of ICM and/or trophectoderm lysis, the blastocyst was discarded and another one was warmed when available. After survival assessment, the blastocyst was maintained in an incubator before intrauterine transfer 2–4 h hours later under ultrasound guidance.
Endometrial preparation before embryo transfer (ET)
For fresh ET, the women began progesterone treatment (800 mg vaginal capsule, Utrogestan® Besins International, Montrouge, France), the day of the oocyte retrieval (i.e. fresh transfer occur on the 6th day of progesterone exposure), and E2 was delivered transdermally (2 mg/day, through two 100 systems simultaneously, Femsept® Theramex, La Defense, France) one day before the ET.
For frozen ET, the endometrium was prepared either with (i) hormonal replacement therapy (HRT) preceded by a degree of down-regulation with a GnRH agonist (a single dose of 11.25 mg IM, Decapeptyl®; Ipsen Pharma, Boulogne-Billancourt, France), or (ii) a modified natural or (iii) a stimulated cycle regimen. The protocol for HRT cycles has been described previously [11]. Briefly, progesterone supplementation began five days before the embryo transfer with vaginal progesterone at 800 mg daily (Utrogestan®, Besins International, Montrouge, France) without any change in the progesterone dose during the treatment. The last dose before the embryo transfer was administered on the morning of the embryo transfer (between 7 and 9 a.m.). The blastocysts were warmed on the day of transfer, i.e., on the 6th day of progesterone exposure. For a stimulated cycle, 25–75 IU/day of recombinant follicle-stimulating hormone (FSH) or urinary FSH (hMG) was used from day 4 of the cycle. For the modified natural and stimulated ovulatory cycle regimens, ovulation was determined by ultrasound monitoring as soon as the leading follicle was larger than 16 mm. Final oocyte maturation was achieved using rhCG triggering (Ovitrelle®; Merck Serono, Lyon, France). Vaginal progesterone at a dose of 800 mg per day (Utrogestan®, Besins International) was administrated for luteal phase support, starting 36 h after ovulation triggering. Women who became pregnant by these procedures continued with the same dose of progesterone (P) (and E2 treatment in HRT cycles) until 12 weeks of gestation.
Data analysis and statistics
For the purpose of this study, two groups were compared: (i) a group of women who received a fresh D6 blastocyst transfer (Fresh D6 group), defined as the first fresh embryo transfer, and (ii) a group composed of women who underwent a frozen-thawed D6 blastocyst transfer (Frozen overall D6 group), defined as the first warming cycle of a D6 blastocyst with possible previous fresh or frozen D5 embryo transfer. Among these D6 first warming cycles, a subgroup called “Elective frozen D6” consisting of a freeze-all cycle without any previous fresh or frozen D5 embryo transfers was analyzed and also compared with the 109 fresh D6 transfers.
The primary outcome was the live birth rate after a single D6 blastocyst transfer. A live birth corresponded to the delivery of a viable infant at ≥ 28 weeks of gestation after embryo transfer [12]. The secondary outcomes included the clinical pregnancy (cPR) and early miscarriage rates. Clinical pregnancy was determined by ultrasonographic documentation of at least one fetus with a heartbeat at 6–7 weeks of gestation [13]. The early miscarriage rate (EMR) was defined as pregnancy loss occurring after confirmed cPR, as an intrauterine pregnancy ≤ 10 weeks based on size by ultrasound [14].
The data were entered into a digital database and analyzed using SPSS software (SPSS Inc., Chicago, IL, USA). A p-value < 0.05 was considered to be statistically significant. For the univariate statistical analysis, we used specific tests: Pearson’s χ2 or Fisher’s exact test for the qualitative variables and the Kruskal–Wallis or the Mann–Whitney test for the quantitative variables, as appropriate. A logistic regression analysis was performed to determine the variables that could be independently associated with the LBR and that could affect outcomes. The variables associated with a live birth occurrence at a threshold of p ≤ 0.10 in univariate analysis and those clinically relevant were retained for the multivariate analysis. Correlation between the baseline characteristic variables was tested, and, if two variables were highly correlated, only one of them was introduced in the model. The parameter values for each of the final models were determined by the maximum likelihood method. In case of significant differences, odds ratios (OR) and their 95% confidence intervals (CI 95%) were calculated from the model’s coefficients and their standard deviations.



留言 (0)